Bilateral ulna hemimelia with humeroradial synostosis and oligodactyly: A case report
Yaa Achiaa Afreh, Kwasi Adjepong Twum, Adu Tutu Amankwa, Kwasi Ankomah, Obed Kojo Otoo, Caroline Oku

TL;DR
This case report describes a rare congenital limb condition in an 11-month-old girl from Ghana, involving missing ulna bones and joint abnormalities.
Contribution
The paper presents the first documented case of bilateral Type 4 ulna hemimelia in Ghana.
Findings
The patient exhibited bilateral complete ulna hemimelia, humeroradial synostosis, and oligodactyly.
Radiographs confirmed the absence of ulna and other skeletal abnormalities in both upper limbs.
The case highlights the importance of radiological assessment for accurate diagnosis and management.
Abstract
Hemimelia denotes the partial or complete absence of the distal half of a limb. Ulna hemimelia, a rare congenital anomaly, involves the complete or partial absence of the ulna in the upper limb, with an incidence of 1 in 150,000. This condition has been classified into 4 types, with the rare Type 4 variant involving humeroradial synostosis. We present a unique case of bilateral complete ulna hemimelia, humeroradial synostosis, and oligodactyly, in an 11-month-old female with bilateral upper limb shortening and restricted elbow movement since birth. Clinical examination revealed bilateral upper limb shortening, medial deviation of both wrist joints, fixed extension of both elbow joints, and bilateral absence of the cubital fossa. Radiographs confirmed bilateral micromelia, absence of ulna, humeroradial synostosis, and oligodactyly. This case, exhibiting bilateral Type 4 ulna hemimelia…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2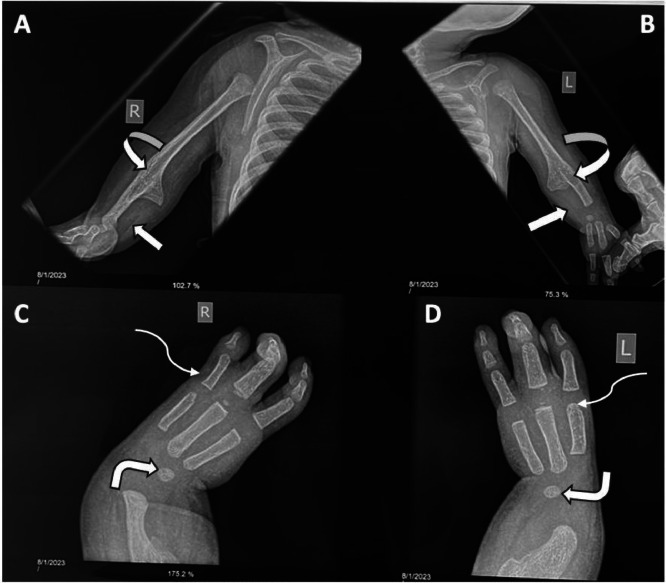 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital limb and hand anomalies · Prenatal Screening and Diagnostics
Introduction
The term “hemimelia” was coined by Isidore Geoffroy Saint-Hilaire in 1836 and refers to the partial or complete absence of the distal half of a limb [1]. Ulna hemimelia is characterized by a postaxial longitudinal deficiency in the upper limb, where the ulna is either completely or partially absent [1].
Initially documented in 1683, this congenital anomaly is rare, with an incidence of 1 in 150,000 [1]. Males are more commonly affected, exhibiting a male-to-female ratio of 3:2 [2]. Approximately 70% of cases are unilateral, often on the right side, and tend to be incomplete [2,[3]](#bib0003). While some individuals may remain asymptomatic with mild isolated ulna deficiency, complex ulna deficiencies can lead to various upper limb abnormalities, such as humeroradial synostosis, radial head dislocation, metacarpal and carpal coalition, and digital abnormalities [1]. Given the diverse nature of forearm and hand deformities, radiological investigations are crucial for accurately identifying the specific type of deficiency [1].
Although a limited number of cases have been documented in the literature [4], [5], [6], [7], [8], we present a unique instance of bilateral complete ulna hemimelia accompanied by humeroradial synostosis and oligodactyly.
Case presentation
An 11-month-old female child presented with bilateral upper limb shortening and limited elbow movement from birth. Mother was not a regular antenatal clinic attendant and pregnancy was poorly monitored. Nevertheless, she delivered in a health facility. There was no history of drug or alcohol abuse during pregnancy.
Upon examination, bilateral upper limb shortening with medial deviation of both wrist joints was observed (Fig. 1). While shoulder and wrist movements were within normal limits, there was a fixed extension of the elbow joints bilaterally, and no elbow joint movement was noted. Both upper limbs were internally rotated, and the cubital fossa was absent bilaterally (Figs. 1 and 2). No other major anomalies were evident. Radiographs of the vertebral column revealed no abnormalities, and both echocardiography and renal ultrasound results were within normal limits.Fig. 1. Clinical photograph of patient showing bilateral upper limb shortening and extension, absence of cubital fossae (curved arrows) and medial deviation of the wrist joints (block arrows).Fig 1. Fig. 2Clinical photograph showing internal rotation of both upper limbs (curved arrows).Fig 2
Anteroposterior radiographs of both upper limbs indicated bilateral micromelia, with the absence of the ulna bilaterally and shortening of the radii. The upper limbs were fixed in an extended position, and bilateral humeroradial synostoses were also present (Fig. 3 A and B). Additionally, anteroposterior radiographs of both wrist joints and hands revealed ulna deviation of the wrist joints bilaterally, with only one carpal bone visible per wrist. Furthermore, both hands displayed 3 digits (Fig. 3 C and D).Fig. 3(A-D): Antero-posterior radiographs of both upper limbs (A and B) showing absence of the ulna bilaterally (block arrows) with elbow fixed in extension and bilateral humeroradial bony fusion (curved arrows). Anteroposterior radiographs of both wrists (C and D) show ulnar deviation with the presence of one carpal bone (bent arrows) and three digits (tridactyly) (squiggle arrows).Fig 3
Discussion
Ulna hemimelia is a rare congenital upper limb deficiency resulting from the incomplete formation of part or the entire ulna. The rarity of this deformity is attributed to the early development of the ulna during the embryonic period (24-36 days), corresponding to a period of high fetal mortality [9]. While often nonsyndromic, ulna hemimelia may be associated with conditions such as Poland syndrome, Goltz-Gorlin syndrome, Cornelia de Lange syndrome, or femur fibula ulna syndrome [10].
Bayne et al. [11] classified ulna hemimelia into 4 types; Type 1 refers to hypoplasia of the ulna with both the proximal and distal epiphysis being present, Type 2 partial aplasia of the ulna, Type 3 is complete absence of the ulna that is accompanied by severe carpal and digital abnormalities, and Type 4 including humeroradial synostosis.
Humeroradial synostosis, a rare condition [6], can be further classified into Class 1 (sporadic, fixed in extension with ulna ray hypoplasia) and Class 2 (familial, fixed in flexion without hypoplasia) [12]. Pffeifer and Braun Quentin also studied the genetic basis of humeroradial synostosis and categorized it into three entities, autosomal dominant ankylosis of the elbow with multiple joint synostosis, autosomal recessive humeroradial synostosis with ulna dysgenesis and possibly the femur and fibula but without digital anomalies and nongerminal humeroradial synostosis as part of ulna longitudinal dysplasia with digital anomalies [13].
Bilateral ulna hemimelia and bilateral humeroradial synostosis are uncommon, with previous studies reporting bilateral ulna hemimelia in 35.3% [4] and bilateral humeroradial synostosis in 21% [8] of cases. Our case of bilateral Type 4 ulna hemimelia with Class 1 bilateral humeroradial synostosis is a rare and complex variant, potentially the first reported in Ghana. Notably, our female patient contradicts the usual male prevalence [2], similar to what Aggarwal et al. [6] have documented, and she falls into the Pfeiffer and Braun Quentin Type 3 category, the most common in a study by El-Hassan et al, accounting for 92.8% of cases [8].
Ulna hemimelia may also be associated with complex carpal, metacarpal, and digital abnormalities. Aplasia, hypoplasia and fusion of the carpal or metacarpal bones may be present with the triquetrum and capitate being frequently absent in these patients [1]. Our case exhibited one carpal bone in the wrists bilaterally. Accounting for the age (the capitate and hamate ossification centers are expected to be present), this suggests absence of the capitate. Furthermore, our patient exhibited tridactyly (a three-fingered hand), the predominant hand anomaly linked to ulna hemimelia, with monodigital hand being the subsequent occurrence [1,[5]](#bib0005).
Although humeroradial synostosis can be associated with Antley-Bixter syndrome, a rare disorder characterized by various manifestations including humeroradial synostosis, camptodactyly, arachnodactyly, joint contractures, craniosynostosis, brachycephaly, dysplastic ears and midface hypoplasia, our patient did not exhibit other associated features. Though our patient had bilateral humeroradial synostosis we did not suspect Antley-Bixter syndrome since the other manifestations were absent.
Management of these conditions is challenging due to the complexity of abnormalities, requiring tailored approaches. Treatment typically involves passive physiotherapy to prevent disuse atrophy. Unilateral ulna hemimelia often does not require surgical intervention [5] as most patients are able to perform activities of daily living without significant restrictions [8], while bilateral cases may necessitate procedures such as soft tissue releases, humeral derotational osteotomies, or elbow disarticulation with prosthetic placement [5]. In our case, continuous passive physiotherapy was initiated, and long-term follow-up is planned to assess the need for surgical intervention and monitor overall progress.
Patient consent
A written informed consent relating to use of patient's medical history and radiological images was obtained after careful explanation to the patient's guardian that their anonymized images and clinical history will be used for publication in a scientific journal.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frantz DHO'Rahilly R Ulnar hemimelia Artif Limbs 152197125355135223 · pubmed ↗
- 2Jain SKA study of 200 cases of congenital limb deficiencies Prosthet Orthot Int 1831994174179772435010.3109/03093649409164402 · doi ↗ · pubmed ↗
- 3Rogala EJ Wynne-Davies R Littlejohn A Gormley J Congenital limb anomalies: frequency and aetiological factors: Data from the Edinburgh Register of the Newborn (1964-68)J Med Genet 1131974221233437235310.1136/jmg.11.3.221PMC 1013131 · doi ↗ · pubmed ↗
- 4Swanson AB Tada K Yonenobu K Ulnar ray deficiency: its various manifestations J Hand Surg 95198465866410.1016/s 0363-5023(84)80007-66491207 · doi ↗ · pubmed ↗
- 5Abdulkadir AY Adigun IA Ulnar hemimelia with oilgodactyly: report of two cases Radiol Case Rep 4120092402784351910.2484/rcr.v 4i 1.240PMC 5106539 · doi ↗ · pubmed ↗
- 6Aggarwal AK Ulnar hemimelia with humero-radial synostosis and oligodactyly: a rarity and review of literature Orthop Surg 5:30002020
- 7Özdemir M Turan A Kavak RP Ulnar hemimelia: a report of four cases Skeletal Radiol 4872019113711433071212310.1007/s 00256-019-3167-x · doi ↗ · pubmed ↗
- 8El Hassan B Biafora S Light T Clinical manifestations of Type IV ulna longitudinal dysplasia J Hand Surg 32720071024103010.1016/j.jhsa.2007.05.02017826557 · doi ↗ · pubmed ↗