Histopathology of an autopsy case of a leadless pacemaker system: a case report
Keigo Misonou, Takahiro Doi, Yusuke Shirai, Daigo Nagahara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
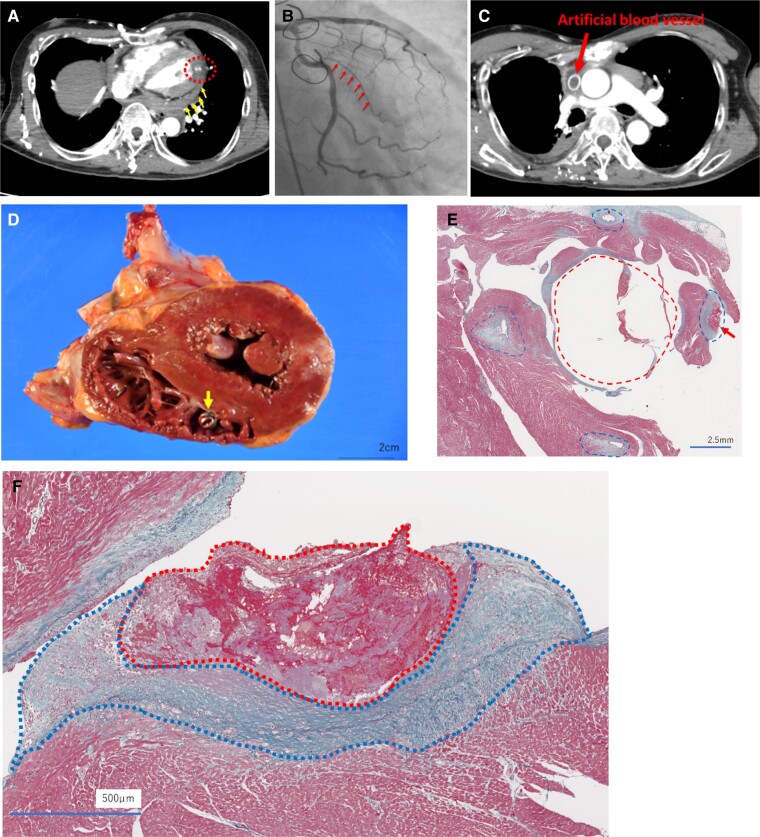 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments · Cardiomyopathy and Myosin Studies
A 60-year-old man presented to a local hospital with chest pain. A computed tomography (CT) scan revealed sub-endocardial left ventricular contrast defects in the lateral wall region and pericardial effusion (Figure 1A). Transthoracic echocardiography performed after transport to our hospital revealed abnormal wall motion of the lateral region of the left ventricle and pericardial effusion at the posterior region of the left ventricle.
Coronary angiography showed 99% stenosis in the left circumflex artery (Figure 1B). Considering the small size of the myocardial infarction and concomitant cardiac oozing rupture, conservative management was chosen. However, administration of amiodarone and beta-blockers for the treatment of refractory supraventricular and ventricular tachycardia resulted in sudden cardiac arrest due to sinus arrest on the 46th day. He became pacemaker dependent, and a leadless pacemaker system (LPS) was implanted on the 53rd day because a CT scan showed occlusion of an artificial vessel in the superior vena cava, which had been replaced 30 years earlier for treatment of a thymoma^1,2^ (Figure 1C).
However, he died of pump failure from diastolic dysfunction of both ventricles due to marked epicardial fibrosis 1 month after implantation of the pacemaker.
Autopsy showed that the LPS was implanted in the right ventricular myocardium (Figure 1D). Elastica–Masson staining (Figure 1E and F) revealed thrombus formation around the site of implantation. Endocardial fibrosis and inflammatory cell infiltration were also observed around the thrombus.
The removability of new LPSs after long-term implantation is a major problem that has yet to be resolved.^3^ At autopsy in this case, the LPS was covered with fibrotic tissue on the surface of the implantation site even only 4 weeks after implantation, raising questions about the removability of the device even after a short period. The indication for device retrieval should be carefully considered in cases with a long period after implantation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reddy VY , Exner DV, Doshi R, Tomassoni G, Bunch TJ, Estes NAM, et al Primary results on safety and efficacy from the LEADLESS II-phase 2 worldwide clinical trial. JACC Clin Electrophysiol 2022;8:115–117.34863657 10.1016/j.jacep.2021.11.002 · doi ↗ · pubmed ↗
- 2Reynolds D , Duray GZ, Omar R, Soejima K, Neuzil P, Zhang S, et al A leadless intracardiac transcatheter pacing system. N Engl J Med 2016;374:533–541.26551877 10.1056/NEJ Moa 1511643 · doi ↗ · pubmed ↗
- 3Kammler J , Blessberger H, Fellner F, Kypta A, Lambert T, Engl M, et al First autopsy description of changes 1 year after implantation of a leadless cardiac pacemaker: unexpected ingrowth and severe chronic inflammation. Can J Cardiol 2016;32:1578.e 1–1578.e 2.10.1016/j.cjca.2015.12.02826927858 · doi ↗ · pubmed ↗