Bilateral Inverted V-shaped High Tibial Osteotomy: A Case Report
Aboubacar Lawan Abdou, Taha El Aissaoui, Adnane Lachkar, Najib Abdeljaouad, Hicham Yacoubi

TL;DR
A young patient with bilateral knee deformity underwent staged reverse V-shaped tibial osteotomy surgeries, achieving successful correction despite complications on one side.
Contribution
The study presents a novel application of reverse V-shaped high tibial osteotomy as an effective alternative to knee replacement for varus deformities.
Findings
The patient achieved successful correction and bone consolidation despite an infection on the left side.
Reverse V-shaped osteotomy provided satisfactory functional outcomes compared to other techniques.
Preoperative planning was crucial for determining specific correction angles for each knee.
Abstract
The article describes the case of a young patient with bilateral genu varum deformity, limiting her mobility. The therapeutic decision was a staged reverse V-shaped tibial osteotomy on both knees at a six-month interval. The surgery faced infectious complications on the left side, requiring additional treatment. Despite this, the patient achieved successful correction, with wound healing and bone consolidation. Preoperative planning was crucial, determining specific correction angles for each knee. The reverse V-shaped osteotomy demonstrated satisfactory functional outcomes compared to other techniques. The conclusion emphasizes the effectiveness of reverse V-shaped high tibial osteotomy (HTO) in addressing varus tibial deformities, providing an alternative before considering total knee arthroplasty. Multicenter studies and long-term evaluations are recommended to refine this surgical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1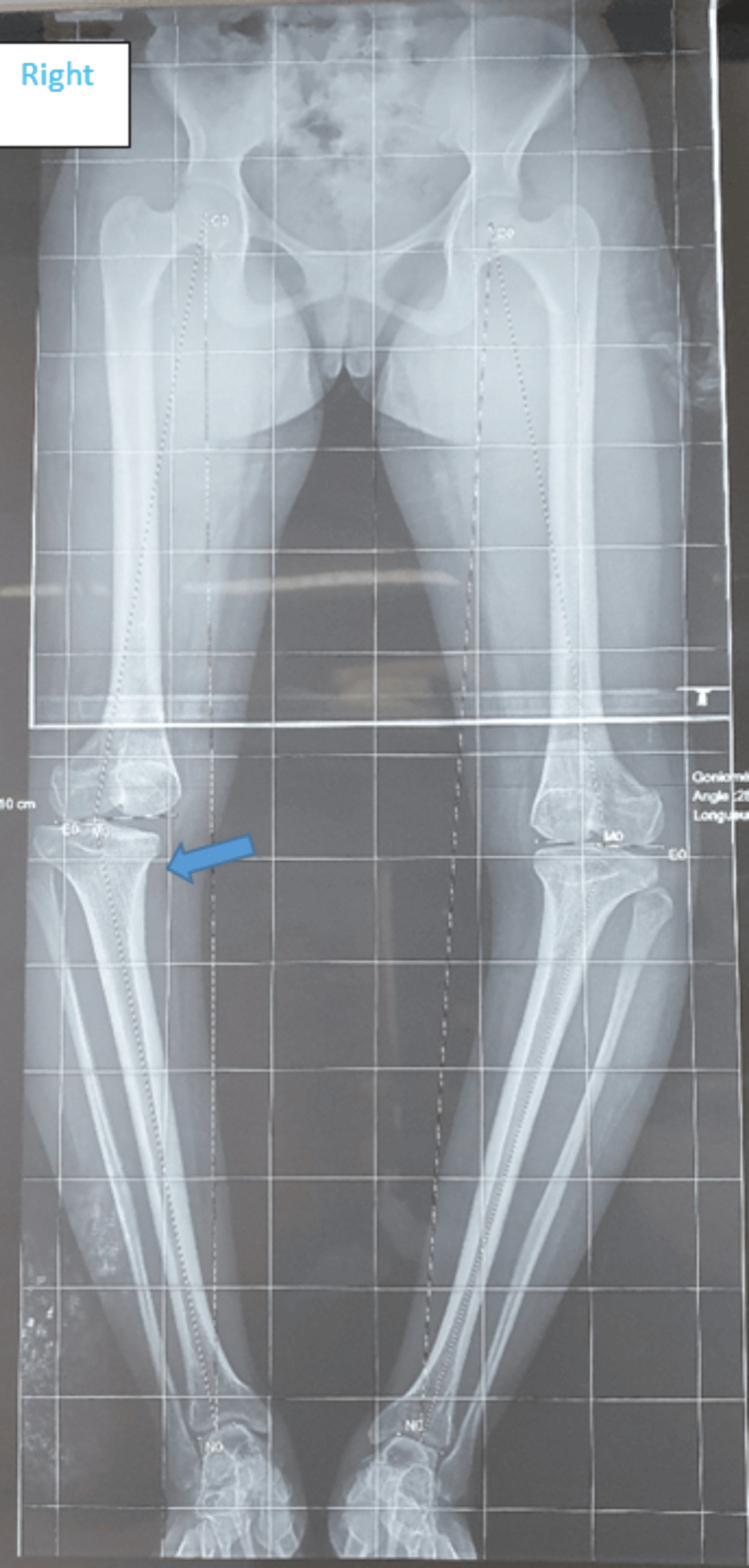 Figure 2
Figure 2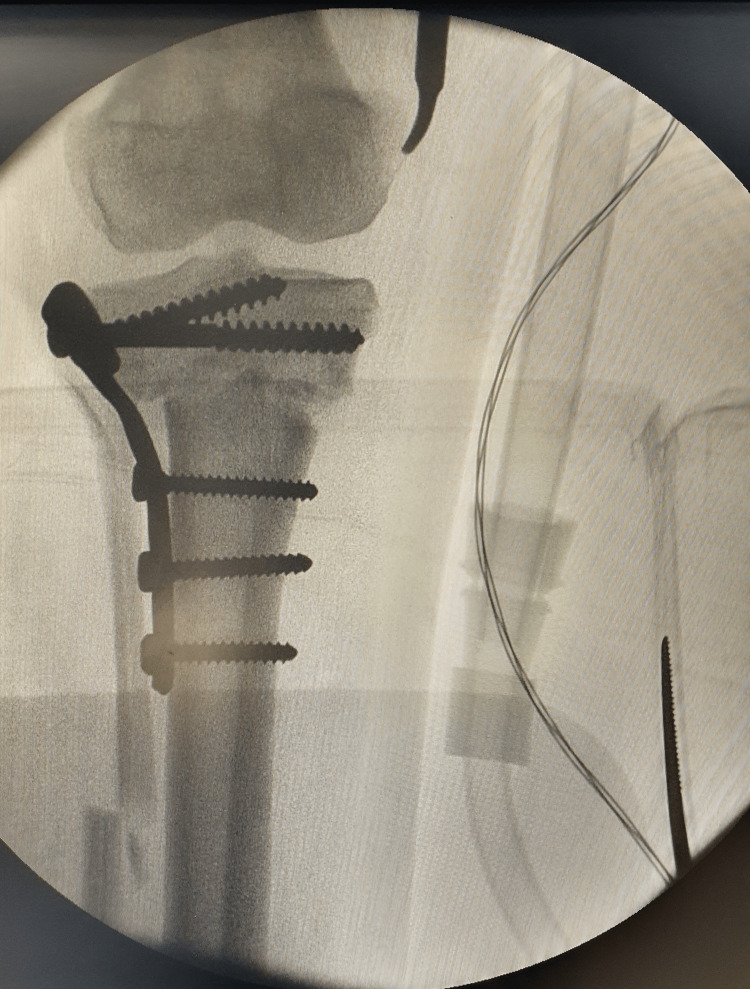 Figure 3
Figure 3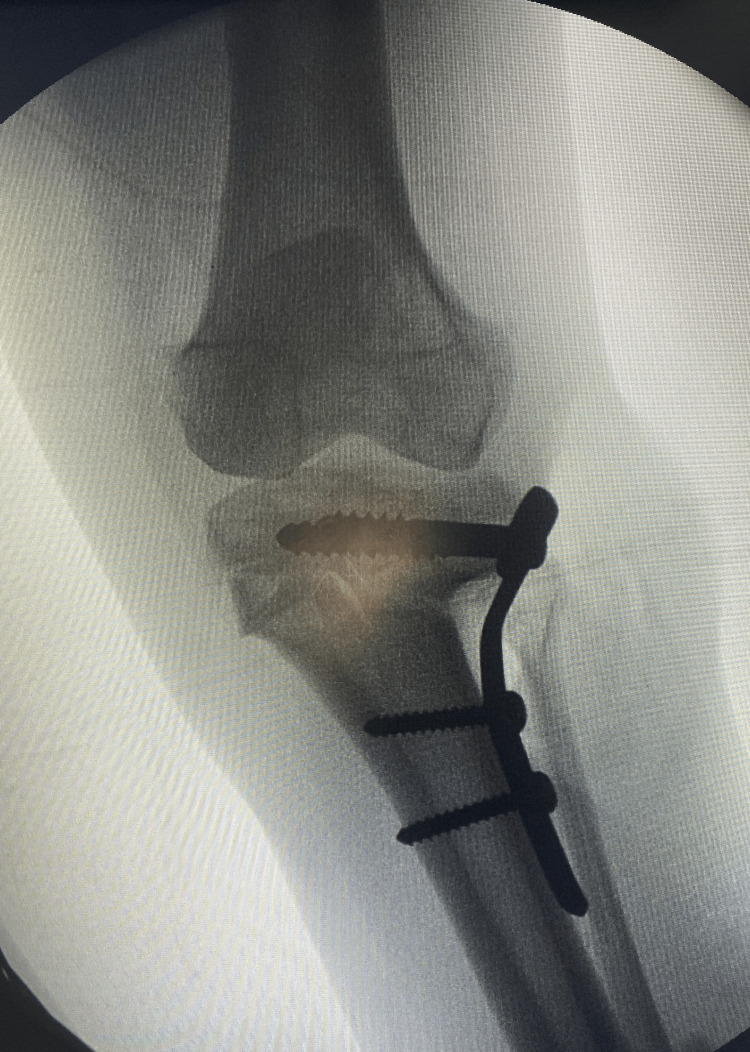 Figure 4
Figure 4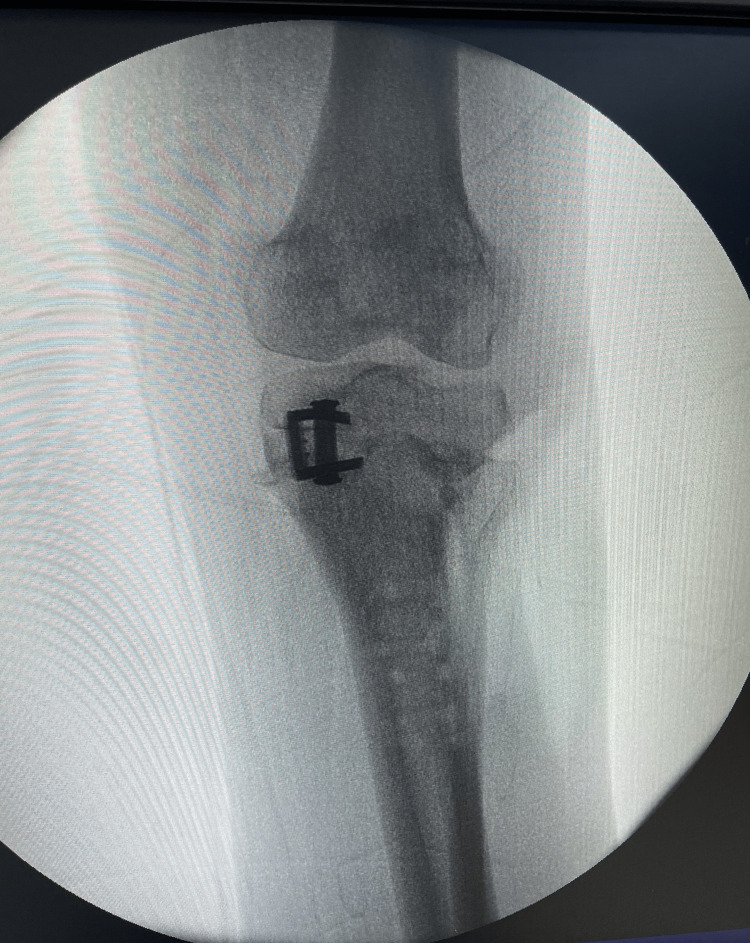 Figure 5
Figure 5 Figure 6
Figure 6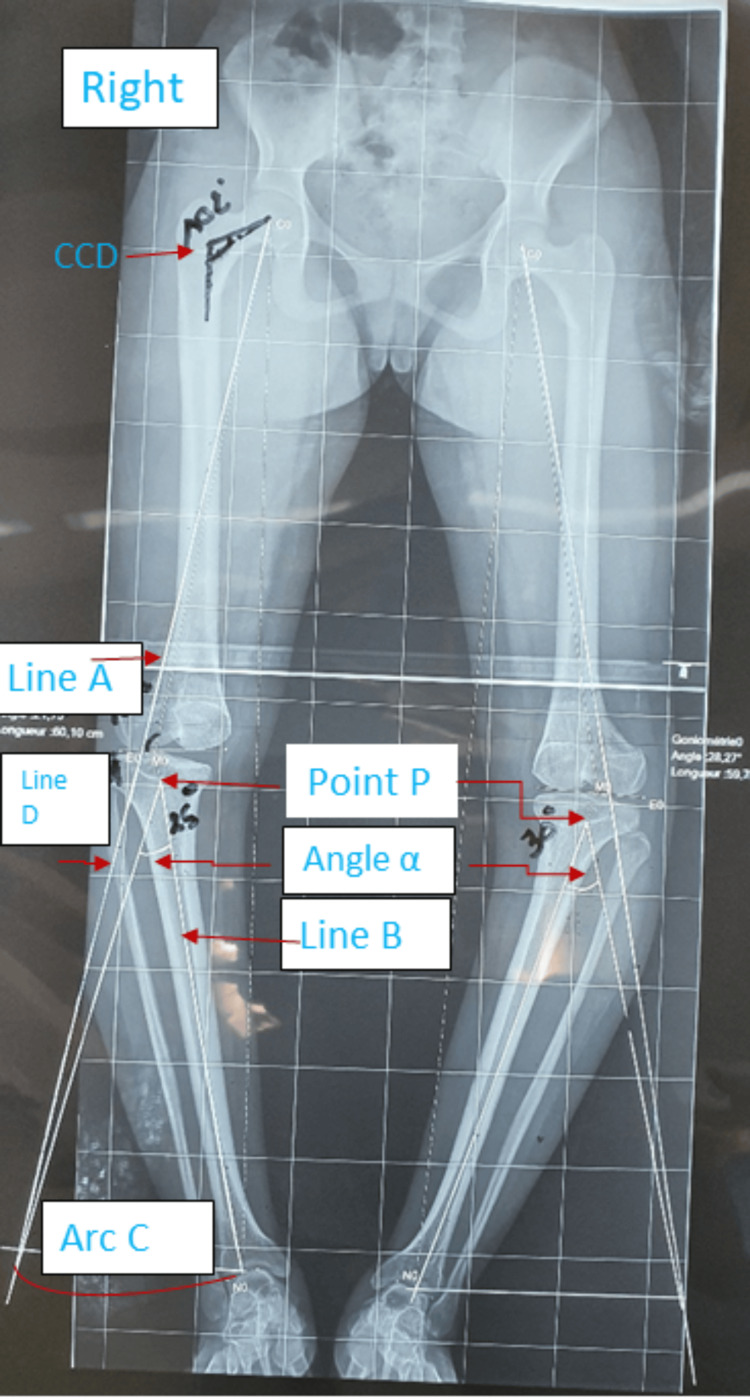 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Knee injuries and reconstruction techniques · Orthopaedic implants and arthroplasty
Introduction
The knee joint is subject to significant loads, bearing multiple times the body weight during daily life activities. It is a highly complex joint, and its stability primarily relies on the interaction of ligamentous, meniscal, muscular, and tendinous structures, cartilage, and bone [1]. The absence of automatic progression to osteoarthritis in this joint is attributed to the perfect distribution of loads achieved through the interaction of these elements and proper alignment. Osteotomies play a crucial role in balancing the mechanical load between the two tibiofemoral compartments by correcting abnormal joint alignment [1,2].
We present the case of a young patient who underwent bilateral high tibial osteotomy (HTO) within our department.
Case presentation
We report the case of a 21-one-year-old female student, apparently without significant medical history, presenting with mechanical pain in both knees and a progressively developing bilateral varus deformity, increasingly restricting the walking perimeter. The patient reported that the deformity had slowly manifested since the age of twelve. At that time, she had received realignment orthoses, but without clinical improvement.
Upon general examination, the patient was in good overall health without apparent dysmorphic features. Walking was possible but accompanied by a noticeable limp. Standing revealed a bilateral genu varum morphotype with a width of 10 fingerbreadths (19.5 cm), persisting even in the supine position (Figure 1). Joint ranges of motion in both knees were preserved. Palpation of the joint space did not elicit pain. Both hips were free and painless, and the spinal examination revealed no particularities. The patient underwent a long-leg standing X-ray (Figure 2).
Clinical appearance revealing a pronounced bilateral genu varum deformity.
Preoperative pangonogram revealing the location of the deformity.The blue arrow indicates the tibial location of the deformation.
The therapeutic decision was to perform a two-stage osteotomy on both knees with a six-month interval between each procedure. We conducted a "V-shaped" osteotomy on the right knee, followed by the left knee (Figures 3, 4). The postoperative course was uneventful for the right knee, while for the left knee, complications arose, including purulent drainage on day 19 accompanied by a fever reaching 39°C, suggestive of a postoperative infection. Management involved surgical debridement, plate replacement, and cytobacteriological sampling. Analysis revealed Staphylococcus aureus sensitive to ciprofloxacin and ceftriaxone.
Intraoperative fluoroscopic view of the right knee demonstrating correction and stabilization with a plate.
Intraoperative fluoroscopic view of the left knee demonstrating correction and stabilization with a plate.
Two months later, arthroscopic lavage was performed, followed by another procedure a month later, involving further debridement and replacement of the plate with two staples (Figure 5). These interventions led to drying of the operative site and bone consolidation in less than two months.
Fluoroscopic view showing post-plate removal and staples placement.
Currently, the patient walks without pain or mechanical aid, and she is satisfied, resuming her daily activities seven months after the osteotomy on the second side (Figure 6).
Clinical appearance of correction at 12 months from the first surgery.
Preoperative planning is a crucial step in the management process. It is conducted based on a pangonogram, allowing for the determination of the required correction. We identified a correction angle of 25° for the right knee and 30° for the left knee (Figure 7). The decision to start with the right side was influenced by the intensity of pain reported by the patient. This personalized approach aims to maximize the benefits of the osteotomy while taking into consideration the specific symptoms experienced by the patient.
Preoperative planning detailing correction angles, 25° on the right and 30° on the left.Line A, line B, line D, and arc C are drawn to calculate angle α. Determination of the point P at 3 centimeters from the joint surface.CCD: Hip cervico-diaphyseal angle.
Discussion
The operative technique is as follows. The initial step involves performing a fibular osteotomy at the junction of the upper and lower two-thirds through a small lateral incision. Following this, a reverse V-shaped tibial osteotomy is carried out using an antero-external approach, guided by preoperative data (Figure 7). The entire right lower limb radiograph is employed to outline the lines for the inverted V-shaped osteotomy. The apex point (Point P) is positioned at the center of the tibial condyle, approximately 3 cm from the joint surface line, with an apex angle of around 110°. To ascertain the angle for lateral hemi-wedge resection, a long line (Line A) is drawn from the center of the femoral head through the 65% or 62.5% point on the lateral tibial plateau. Subsequently, another line (Line B) is drawn from the apex point (Point P) to the center of the talar dome, and the length of Line B is measured. An arc (Arc C), with the apex point (Point P) as its center and Line B as its radius, is drawn intersecting Line A. Another line (Line D) is drawn from the apex point (Point P) to the intersection point of Line A and Arc C. The angle (α) formed between Lines B and D represents the lateral hemi-wedge resection angle, which is identical to the correction angle of the lower limb alignment. Using the angle (α), a dashed line is drawn to represent the lateral hemi-wedge resection line [3].
As with any knee deformity, it is crucial to first determine the origin of the malalignment: femoral, tibial, or mixed [3]. In varus knee deformities, only 28% of patients exhibit an exclusive tibial localization and are potential candidates for HTO [4]. This involves a meticulous analysis, using a pangonogram, of certain angles such as medial proximal tibial angle (MPTA), mechanical lateral distal femoral angle (mLDFA), the mechanical axis of the femur, joint-line convergence angle (JLCA) [2,5,6].
Once the tibial origin is confirmed, the next step is to calculate the correction angle. A first line is drawn from the center of the femoral head to the center of the talus. The second line passes through the femoral head and the Fujizawa point, located between 65 and 70% (from internal to external) of the proximal tibial articular surface for Kellgren-Lawrence stages 2 and 3, or at 62.5% if stages 1 or 2 [3].
Aoki et al. argue that there is a lower risk of delayed consolidation and loss of radiological correction with the reverse V-shaped osteotomy [7]. This technique is considered reliable, with functionally satisfactory results (according to the Japanese Orthopaedic Association functional score) at 83%, compared to 63% with a closing wedge osteotomy. It should be noted that, in this comparative study, the preoperative status of both groups was similar [7]. Maintaining correction, even after the removal of the osteosynthesis material, is considered by several authors as a guarantee of a good long-term result with a correction angle [8,9].
Various complications have been reported in the literature. In order of frequency, these include fractures of the cortical hinge, implant pain, loss of correction, fibular nerve injuries, surgical site infections, and pseudarthrosis or delayed consolidation [10,11]. Infection was the only complication observed in our patient. The reverse V-shaped HTO is a reliable method to delay or even halt joint destruction in often young patients with significant tibial varus deformity. This allows postponing the radical solution of arthroplastic replacement without excluding it altogether [12,13].
Conclusions
High tibial osteotomy (HTO) serves as a solution to improve knee function and delay or even avoid the potential need for arthroplasty. The practitioner should always consider the possibility of subsequent total knee replacement because joint deterioration, though significantly slowed, may eventually progress to the ultimate stage of osteoarthritis. In conclusion, multicenter case series studies and long-term evaluations are imperative to refine this surgical procedure and achieve even better functional outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1High tibial osteotomy: review of techniques and biomechanics J Healthc Eng Liu X Chen Z Gao Y Zhang J Jin Z 836312820192019 https://doi.org/10.1155/2019/83631283119185310.1155/2019/8363128 PMC 6525872 · doi ↗ · pubmed ↗
- 2Preoperative planning and preservation of the knee with complex osteotomies Mo Med Kfuri M Crist BD Stannard JP 1441511192022 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 9339400/36036038 PMC 9339400 · pubmed ↗
- 3Inverted v-shaped high tibial osteotomy for medial osteoarthritic knees with severe varus deformity Arthrosc Tech Kondo E Yasuda K Yabuuchi K Aoki Y Inoue M Iwasaki N Yagi T 072018 https://doi.org/10.1016/j.eats.2018.06.00510.1016/j.eats.2018.06.005PMC 620323230377579 · doi ↗ · pubmed ↗
- 4High tibial osteotomy for varus deformity of the knee J Am Acad Orthop Surg Glob Res Rev Murray R Winkler PW Shaikh HS Musahl V 5202110.5435/JAAOS Global-D-21-00141 PMC 827479334242204 · doi ↗ · pubmed ↗
- 5Deformity planning for frontal and sagittal plane corrective osteotomies Orthop Clin North Am Paley D Herzenberg JE Tetsworth K Mc Kie J Bhave A 425465251994 https://pubmed.ncbi.nlm.nih.gov/8028886/8028886 · pubmed ↗
- 6Isolated high tibial osteotomy is appropriate in less than two-thirds of varus knees if excessive overcorrection of the medial proximal tibial angle should be avoided Knee Surg Sports Traumatol Arthrosc Feucht MJ Winkler PW Mehl J Bode G Forkel P Imhoff AB Lutz PM 32993309292021 https://doi.org/10.1007/s 00167-020-06166-3.3269109310.1007/s 00167-020-06166-3PMC 8458209 · doi ↗ · pubmed ↗
- 7Inverted V-shaped high tibial osteotomy compared with closing-wedge high tibial osteotomy for osteoarthritis of the knee. Ten-year follow-up result J Bone Joint Surg Br Aoki Y Yasuda K Mikami S Ohmoto H Majima T Minami A 133613408820061701242410.1302/0301-620X.88B 10.17532 · doi ↗ · pubmed ↗
- 8High tibial valgus osteotomy for medial gonarthrosis: a 10- to 21-year study J Knee Surg Aglietti P Buzzi R Vena LM Baldini A Mondaini A 2126162003 https://pubmed.ncbi.nlm.nih.gov/12568262/12568262 · pubmed ↗