Randomized controlled double-blind trial of methylprednisolone versus placebo in patients with post-COVID-19 syndrome and cognitive deficits: study protocol of the post-corona-virus immune treatment (PoCoVIT) trial
Christiana Franke, Vanessa Raeder, Fabian Boesl, Benno Bremer, Lucas C. Adam, Ameli Gerhard, Irina Eckert, Anneke Quitschau, Anne Pohrt, Susen Burock, Lisa Bruckert, Carmen Scheibenbogen, Harald Prüß, Heinrich J. Audebert

TL;DR
This study tests if methylprednisolone helps improve cognitive issues in people with long-term effects after COVID-19.
Contribution
The trial introduces a novel approach to treating post-COVID cognitive deficits using methylprednisolone based on autoimmunological hypotheses.
Findings
The trial will assess cognitive improvement using the Multifactorial Memory Questionnaire.
It will explore biomarker and MRI changes linked to cognition in post-COVID patients.
Long-term effects on memory and quality of life will be evaluated over 52 weeks.
Abstract
Post-COVID-19 Syndrome (PCS) includes neurological manifestations, especially fatigue and cognitive deficits. Immune dysregulation, autoimmunity, endothelial dysfunction, viral persistence, and viral reactivation are discussed as potential pathophysiological mechanisms. The post-corona-virus immune treatment (PoCoVIT) trial is a phase 2a randomized, controlled, double-blind trial designed to evaluate the effect of methylprednisolone versus placebo on cognitive impairment in PCS. This trial is designed based on the hypothesised autoimmunological pathogenesis and positive aberrations, employing a series of off-label applications. Recruitment criteria include a diagnosis of PCS, a minimum age of 18 years and self-reported cognitive deficits at screening. A total of 418 participants will be randomly assigned to either verum or placebo intervention in the first phase of the trial. The trial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
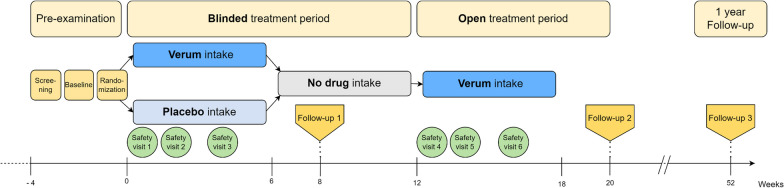 Figure 1
Figure 1- —http://dx.doi.org/10.13039/501100010571Bundesministerium für Bildung, Wissenschaft, Forschung und Technologie
- —Charité - Universitätsmedizin Berlin (3093)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Sclerosis Research Studies · Peripheral Neuropathies and Disorders · Healthcare and Venom Research
Introduction
In late 2019, a new strain of the coronavirus-family, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged. It spread rapidly around the world and precipitated the Coronavirus Disease 2019 (COVID-19) pandemic, thereby significantly impacting global public health [13]. Consequently, many patients continue to experience protracted symptoms, commonly referred to as ‘long-COVID’ or post-COVID-19 syndrome (PCS), a condition that poses a substantial burden to society. PCS exhibits an overall estimated prevalence ranged from 7.5 to 41% in non-hospitalized adults and 37.6% in hospitalized adults [18]. The manifestation of PCS is more common among younger and female patients [3, 6]. PCS is defined by the WHO as a persistent condition, lasting at least three months after infection with broad spectrum of symptoms which may affect all organ systems and impairing daily activity [22]. Cardinal neurological symptoms include fatigue and cognitive deficits [5], which impose a significant impact on quality of life [22]. Patients report a range of cognitive deficits such as concentration difficulties, word-finding difficulties, memory lapses, attention problems and “brain fog”. Systematic neuropsychological assessments reveal deficits in processing speed, executive function, phonemic fluency, category fluency, and memory encoding [2].
Pathophysiological mechanisms underlying the development of PCS and persistent neurological manifestations following SARS-CoV-2 infection revolve around ongoing viral persistence and direct viral invasion, reactivation of latent herpesviridae, endothelial/microcirculatory dysfunction, neuroinflammation, and autoimmunological processes [9, 15, 16, 21]. These potential pathomechanisms involve the overactivation of the immune system, characterized by hyperinflammation and cytokine release. A notable contributor is the post-viral induction of autoimmunity, a well-established mechanism observed in other diseases [16, 21], alongside molecular mimicry, where anti-pathogen antibodies cross-react with host proteins [19].
Based on previous findings, we propose that SARS-CoV-2 triggers an immune response resulting in a dysregulated autoimmune system involving both cellular and humoral components. Preliminary studies of our research group have shown an association of neuronal antibodies present in both serum and cerebrospinal fluid (CSF) and pathological montreal cognitive assessment (MoCA) results in patients with cognitive deficits [9, 16, 21]. Reactive autoantibodies in the central nervous system (CNS), detected in both serum and CSF during SARS-CoV-2 infection, have been consistently observed in a significant proportion of patients [7, 10, 12, 17]. While the role of biomarkers as indicators for CNS damage or involvement in pathophysiological processes remains challenging, they represent potential targets for immunosuppressive treatment. The rationale behind an autoimmune genesis hypothesis suggests that methylprednisolone could be a viable treatment approach. This well-established anti-inflammatory glucocorticoid has proven efficacy in treating various diseases suspected to have an autoimmune aetiology, characterized by inflammatory changes or immune overactivity. Examples include multiple sclerosis, chronic inflammatory demyelinating polyradiculoneuropathy, and steroid-responsive autoantibody related encephalitis [14]. While some of these diseases can be cured completely with corticosteroids, others require repeated pulse therapy. There are several controlled trials that employ corticosteroids, particularly methylprednisolone, at similar doses for autoimmune neurological diseases [8, 24]. The use of glucocorticoids has been explored in acute SARS-CoV-2 infections associated with an excessive inflammatory response [1, 11]. Methylprednisolone holds promise in disrupting various immunological triggers, presenting a well-known, generally well-tolerated, cost-effective, and widely available therapeutic option [14]. Our data indicates that off-label administration of methylprednisolone resulted in subjective improvements and enhanced performance on neuropsychological tests in a high proportion of PCS patients with CSF autoantibodies (data in preparation). This underscores the potential efficacy of the chosen treatment approach within this specific patient cohort. To date, no randomized, placebo-controlled trials have examined the effects of methylprednisolone in patients with PCS primarily characterized by cognitive deficits.
Methods
Objective of the trial
The post-corona-virus immune treatment (PoCoVIT) trial aims to examine the effect of methylprednisolone versus placebo in patients with cognitive deficits in PCS syndrome in a randomized controlled double-blind trial. Additionally, the trial includes exploratory research to identify potential biomarkers, given the frequent occurrence of CNS reactive autoantibodies in the serum and CSF of patients with PCS, particularly those with neurological symptoms such as cognitive deficits. The PoCoVIT trial may enhance our understanding of treatment strategies, thereby improving patient care. Simultaneously, it contributes to biomarker research advancing our understanding of the disease’s pathomechanisms. The objective is not only to demonstrate improvements in clinically relevant and qualitative patient-oriented measures from baseline to week 8 but also to establish correlations between these measures and objective antibody-related mechanistic indicators derived from baseline CSF, neuroimaging, and biomarkers. The second treatment phase, wherein all patients receive methylprednisolone will provide further insights into whether repetitive corticosteroid pulse therapy proves beneficial in symptom control among patients with PCS.
Trial description and design
The PoCoVIT trial is a prospective, single centre trial (OECD category 2) employing a randomized, double blind, placebo-controlled, 2-arm parallel-group design. Patients with predominantly cognitive deficits are enrolled. Figure 1 provides an overview of the main trial procedures. Methylprednisolone serves as the active treatment (verum), and our hypothesis centres on achieving clinically significant improvement following its administration. The primary endpoint is the intra-patient change in Multifactorial Memory Questionnaire (MMQ) subdomain memory satisfaction by ≥ 15 points from baseline to week 8 [25].Fig. 1. Flowchart of the post-corona-virus immune treatment (PoCoVIT) trial
Eleven trial visits, detailed in Table 1, including screening, are planned for each patient. The total trial duration for each participant is one year, including two treatment phases, each consisting of 4 weeks of treatment followed by 2 weeks of tapering.Table 1. Visit schedule with assessmentsPeriod/Visit nameScreeningBaseline 1Baseline 2 &RandomizationTreatment period: Placebo vs Verum^1^Follow-UpTreatment period: Verum^2^Follow-UpS (V1)B1B2 (V2)SV (V3)SV (V4)SV (V5)FU1 (V6)SV (V7)SV (V8)SV (V9)FU2 (V10)FU3 (V11)Trial days− 28 to 0− 14 to 021428568698112140365Time windows ± 3 days ± 30 daysOutpatient visit••••••••••Informed consent•Inclusion and exclusion criteria•Randomization•Discharge from trial•HistoryDemographic data••Medical history•Diagnostic assessmentsStructural cMRI•Diagnostic blood sample^3^•••Lumbar puncture^4^•Safety assessmentsNeurological and general physical examination•••Pregnancy test in female patients•••••Blood sample A^5^••••••Blood sample B^6^•••Clinical and sonographic exclusion of thrombosis••AE questioning•••••••••Concomitant medication••••••••••Outcome assessmentsPatient reported symptoms••••Multifactorial Memory Questionnaire••••Short form 36 Health survey••••Fatigue severity scale••••Chalder fatigue scale••••Beck depression inventory-II•••Montreal cognitive assessment•••PROMIS 29•••PROMIS Cognitive Function Short form 4a•••Verbal learning and memory test•••Brief Visuospatial memory test—revised•••WAIS-IV•••Test battery for attention performance•••Trail-making-test A and B•••Regensburger Wortflüssigkeits-test•••Symbol digit modalities test••Wortschatztest•LPS•Assessment of self-experienced exposure to IMP•Enrolment in diagnostic and biomarker platform study in a subgroup••AE, Adverse Event; cMRI, cranial magnetic resonance imaging; LPS, Performance testing system (Leistungsprüfungssystem: Subtest 3: Logical Thinking); PROMIS, Patient reported outcomes measurement information system; WAIS-IV, Digit span (forward/backward) from the Wechsler Adult Intelligence Scale-Fourth Edition^1^Treatment period: Placebo vs Verum begin at day 1 ± 3^2^Treatment period: Verum begin at day 85 ± 3^3^Blood sample: autoantibodies, complement system and inflammatory markers^4^Lumbar puncture: autoantibody testing and inflammatory markers^5^Blood sample A: Glucose, Na, K, GFR, creatinine^6^Blood sample B: Differential blood count, glucose, Na, K, HbA1c, GFR, creatinine, TSH, AST, ALT
Patients receive trial information and undergo screening before enrolment. At baseline 1 (B1), participants are scanned using cerebral MRI. At baseline 2 and prior to randomization (B2/R), patients complete a neurological and neuropsychological assessment. Blood and optional CSF samples are collected and assessed potential occurrence of autoantibodies. Selected patients, with or without autoantibodies, may be enrolled, following informed consent, in the biomarker and diagnostic platform receiving additional blood analyses and imaging. The biomarker and diagnostic platforms within our centre serve as databases for the identification of diagnostic and prognostic markers associated with PCS, using both imaging data and blood/CSF samples. After randomization, treatment phase 1 unfolds over six weeks, during which patients are randomly assigned to either verum (methylprednisolone) or placebo treatment. Follow-up 1 occurs two weeks post the cessation of trial medication of treatment phase 1. After a four-week treatment break, the second treatment phase begins with all patients receiving methylprednisolone for an additional six weeks. Follow-up 2 occurs two weeks post the cessation of treatment phase 2. Follow-up 3, scheduled 52 weeks after randomization, comprises a telephone interview and patient-completed questionnaires.
During both treatment phases, each participant undergoes safety and monitoring assessments involving blood tests and ultrasound examination for exclusion of deep vein thrombosis of the lower extremity. Detailed documentation of demographic data, medical history, and clinical assessments is conducted during the trial visits (for details refer to Table 1).
Eligibility criteria
Patients with PCS and cognitive deficits will be recruited from the specialised outpatient clinic of the Department of Neurology at Charité. Inclusion and exclusion criteria for the trial population are comprehensively outlined in Table 2. Informed consent from all participants is mandatory and will be documented after the screening visit, ensuring at least a 24-h period before baseline 1.Table 2. Inclusion and exclusion criteria for trial populationInclusion criteria1. History of confirmed (PCR or serology) SARS-CoV-2 infection according to WHO criteria2. Ongoing symptoms of PCS for ≥ 3 months3. Self-reported predominant cognitive deficits at screening4. Male or female adult who is 18 years or older at the time of informed consent5. Subject is willing, understanding, and able to provide informed consent6. Signed informed consent prior to initiation of any trial related measure7. For female subject or diverse subjects: (a) Confirmed post-menopausal state, defined as amenorrhea for at least 12 months, or (b) If being of childbearing potential:1. Negative highly sensitive urine or serum pregnancy test before inclusion, and2. Practicing a highly effective birth control method (failure rate of less than 1%): (a) combined (oestrogen and progestogen containing) hormonal (b) contraception associated with inhibition of ovulation (oral/intravaginal/ transdermal), or (c) progestogen-only hormonal contraception associated with inhibition of ovulation (oral/injectable/implantable), or (d) Intrauterine device, or (e) Intrauterine hormone-releasing system, or (f) Bilateral tubal occlusion, or (g) Vasectomised partner, or (h) Heterosexual abstinenceExclusion criteria1. Any ongoing central nervous system disease2. Any major psychiatric disease within the last 10 years3. Previous medical history of gastric ulcer, osteoporosis and/or previous vertebral fractures, rheumatological disease or metabolic disease including diabetes mellitus4. Ongoing immunosuppressive therapy5. Patient is pregnant or breastfeeding at screening6. MMQ memory satisfaction subdomain > 50 points at Screening7. Current malignant disease (including space-occupying brain tumours)8. Body weight < 45 kg9. Severe lactose intolerance10. Participation in another clinical interventional trial within the last 3 months or five half-lives of the other trial’s IMP, if longer than 6 months previous to informed consent11. Patient is institutionalized by order of court or public authority12. Patient who might be dependent on the sponsor, the investigator or the trial site13. Place of living does not allow the subject to attend the planned study visits14. Other conditions that are likely to affect the safety of the study treatment (e.g., severely impaired immune status)Additional exclusion criteria for MRI assessments1. Pacemaker2. Metal implants and other objects that are not proven MRI safe (e.g., drug pumps, heart valves, shards, joint prosthesis, hearing aids, stents)IMP, Investigational medicinal product; MMQ, Multifactorial Memory Questionnaire; MRI, magnetic resonance imaging; PCR, Polymerase chain reaction; PCS, Post-COVID-19 syndrome; SARS-CoV-2, Severe acute respiratory syndrome coronavirus 2; WHO, World Health Organization
Arms and intervention
Participants will be stratified based on age (> 50 years or ≤ 50 years), sex and cognitive screening assessment results, as determined by the MoCA at baseline 2 (> 26/30 or ≤ 26/30 points). Randomization will occur in a 1:1 ratio, assigning participants to either the verum or placebo group. The total intervention duration per participant is 20 weeks. The initial six weeks constitute a double-blind intervention with a starting dose of body weight-adjusted methylprednisolone or matching placebo. In the verum group, participants receive oral methylprednisolone at a dose of approximately 1 mg/kg body weight, taken once daily for four weeks followed by a two-week tapering phase. Conversely, in the control group participants receive a matching placebo orally once daily for six weeks, adhering to a comparable titration schedule to maintain blinding. Following the initial six-week blinded intervention, a drug-free period of six weeks ensues. This is followed by a second, unblinded treatment phase lasting the same duration with an equivalent tapering scheme. During this phase, all participants receive methylprednisolone Three follow-up visits (week 8, week 20, and week 52) are scheduled in addition to the six safety visits.
Outcome measures
The primary outcome measure is the intra-patient change in the MMQ sub-domain memory satisfaction, demonstrating an increase of ≥ 15 points from baseline to week 8 [25]. Key secondary and safety outcome measures include: (a) Intra-patient change in MMQ sub-domain memory satisfaction from baseline to week 20 and week 52, along with changes from week 8 to week 20, and from week 20 to week 52 (b). Mean difference in MMQ sub-domain memory performance and memory strategy from baseline to week 8, (c) Intra-patient change in neuropsychological and cognitive scores and quality of life measures from baseline to week 8 and week 20, and from week 8 to week 20 (d). Exploratory biomarker-related outcomes encompass the occurrence and change in molecular biomarkers in serum and CSF as well as structural or functional alterations in imaging of cortical and subcortical regions and fibre tracts implicated in neurocognitive processes.
The assessment of investigational medicinal product side effects is conducted through adverse event, serious adverse event, and suspected or unexpected serious adverse reaction reports. Detailed objective measures and outcomes are shown in Table 3.Table 3. Objectives and OutcomesObjectiveOutcomePrimaryImprovement in memory satisfaction from baseline to week 8 when comparing methylprednisolone with placebo in PCS patientsIntra-patient change in MMQ subdomain memory satisfaction by ≥ 15 points from baseline to week 8SecondaryLong-term improvement in memory satisfaction from baseline to week 20 and to week 52Intra-patient change in MMQ subdomain “memory satisfaction” from baseline to week 20, from week 8 to week 20 and from week 20 to week 52Improvement in memory ability, and memory strategyMean difference in MMQ subdomain “memory ability” from baseline to week 8 and to week 20 and from week 8 to week 20Mean difference in MMQ subdomain “memory strategy” to week 8 and to week 20 and from week 8 to week 20Improvement in neurocognitive symptoms quantified using neuropsychological and cognitive scoresIntra-patient change in neuro-psychological and cognitive scores (MoCA, neuropsychological test battery, SDMT) from baseline to week 8 and to week 20 and from week 8 to week 20Improvement in quality of lifeIntra-patient change in quantified PROMIS questionnaire and SF-36 from baseline to week 8 and to week 20 and to week 52 and from week 8 to week 20Improvement in fatigue and moodIntra-patient change in fatigue scores (FSS, CFQ) and mood (BDI) from baseline to week 8 and to week 20 and to week 52 and from week 8 to week 20Key safetyInfections meeting SAE criteriaOccurrence of IMP side and adverse effects, assessed with AE, SAE and SUSAR reportsPsychiatric complications (depression, euphoria, severe sleep disorders)Endocrinologic disorders meeting SAE criteriaExploratoryBiomarker-related: Autoimmune activity, immune status, inflammatory biomarkers, complement systemOccurrence and changes in molecular biomarkersBiomarker-related: Structural changes in the brain and in brain functionsStructural and functional alterations in MRI imaging in cortical and subcortical regions and fibre tracts with relevance to neurocognitive processesAE, adverse event; BDI, beck depression inventory II; CFQ, chandler fatigue scale; FSS, fatigue severity scale; IMP, investigational medicinal product; MMQ, Multifactorial Memory Questionnaire; MoCA, Montreal Cognitive Assessment; MRI, magnetic resonance imaging; PROMIS, patient reported outcomes measurement information system; SAE, serious adverse event; SDMT, symbol digit modalities test; SF-36, Short form 36 health survey; SUSAR, Suspected unexpected serious adverse reaction
Sample size calculation and statistical analysis
For the PoCoVIT trial, we aim to detect an improvement in the MMQ sub-domain memory satisfaction. We consider a change of additional 15 points a clinically relevant improvement. Based on our previous data, we anticipate this improvement in 15% of the verum group and 5% of the placebo group. To achieve 90% power at a significance level of α = 0.05, we require 188 patients in each group. This calculation uses a two-sample test for proportions (z-test with arcsine transformation) in the stats package of the R statistical computing environment (version 4.0.2). Assuming a dropout rate of 10%, our recruitment target is 209 patients per group, ensuring that 188 participants remain after dropout. We, therefore, plan to screen 700 patients to enrol the necessary 418, stratified by sex, age, and MoCA score.
Since a single primary outcome is selected, no multiplicity adjustment is required. Analyses of secondary outcomes will be exploratory. For the primary outcome, a binary logistic regression model will be used, focusing on improvement in outcome variables and treatment group as main effects, adjusting for stratification variables. Odds ratios will be reported with 95% confidence intervals, and an alpha of 0.05 has been set for significance. Complete case analysis will be conducted. Where missing values exceed 5%, sensitivity analysis will be performed using multiple imputation chain equations [4].
Secondary outcomes will be initially analysed descriptively and modelled using appropriate techniques such as ANCOVA and logistic models, depending on the outcome distributions. The treatment variable will be included as the main factor adjusting for stratification variables similar to the primary analysis model. Treatment effects will be calculated with two-sided 95% confidence intervals, and outcomes will be analysed in complete cases analyses. Safety, subgroup and interim analyses will be conducted. Statistical analyses will be performed using SAS release 9.2 or higher (SAS Institute Inc., Cary, North Carolina, USA) and R (www.r-project.org) version 4.1.2 or higher.
Contacts
The PoCoVIT trial is conducted within the Nationale Klinische Studiengruppe (NKSG), a clinical trial and translational research platform for the development of treatment in PCS and ME/CFS, funded by the German Ministry of Education and Research (BMBF) [20].
Perspective
This trial is based on the hypothesis that an immune system overactivation triggers sustained hyperinflammation and autoantibody production in PCS. Autoantibodies, including those against neurotransmitter receptors, have been identified in several cohorts of patients with PCS [9, 10]. The identification and specification of relative frequencies are still limited due to the broad spectrum of antibodies. Notably, autoantibodies against G protein-coupled receptors (GPCRs), particularly ß2- and a1-adrenoreceptors, angiotensin II-, muscarinic M2-, MAS-, nociception–, and ETA-receptors, have been found in sera from PCS patients with neurological and/or cardiac symptoms [26]. These autoantibodies correlated with symptom severity (e.g., fatigue, vasomotor and cognitive symptoms) in patients with post-acute sequelae of COVID-19 with chronic fatigue syndrome (PACS-CFS) [23]. Our findings indicate that autoantibodies targeting brain epitopes are common in patients with PCS and strongly associated with pathological cognitive screening test, especially when detected in CSF [9, 10]. However, due to the recent nature of this research, the epitopes and nature of these autoantibodies have not yet been fully characterized.
Evidence regarding the effect of immunosuppressive therapeutics is urgently needed. To date there are no proven therapeutic options to treat patients with PCS, which imposes a significant burden on individuals, society, and the economy. Methylprednisolone, chosen as the active treatment in this trial, is a cost-effective pharmaceutical with demonstrated clinical effectiveness in various immune-mediated diseases. Adverse effects are well described, and safety visits are scheduled accordingly in the PoCoVIT trial. An additional major aim of PoCoVIT is to enhance our understanding of the pathophysiological mechanisms underlying the disease paving the way for potential therapeutic approaches. In PCS, the imperative for adequately powered randomized placebo-controlled trials is evident, seeking to replace controversial experimental therapeutic approaches with evidence-based decision making in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Angus DC Derde L Al-Beidh F Annane D Arabi Y Beane Avan Bentum-Puijk W Berry L Bhimani Z Bonten M Bradbury C Brunkhorst F Buxton M Buzgau A Cheng A Cde Jong M Detry M Estcourt L Fitzgerald M Summers C Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: The REMAP-CAP COVID-19 corticosteroid domain randomized clinical trial JAMA 2020324131317132910.1001/jama.2020.1702232876697 PMC 7489418 · doi ↗ · pubmed ↗
- 2Becker JH Lin JJ Doernberg M Stone K Navis A Festa JR Wisnivesky JP Assessment of cognitive function in patients after COVID-19 infection JAMA Network Open 2021410 e 213064510.1001/jamanetworkopen.2021.3064534677597 PMC 8536953 · doi ↗ · pubmed ↗
- 3Boesl F Audebert H Endres M Pruss H Franke CA neurological outpatient clinic for patients with post-COVID-19 syndrome - A report on the clinical presentations of the first 100 patients Frontiers in Neurology 20211273840510.3389/fneur.2021.73840534603189 PMC 8481602 · doi ↗ · pubmed ↗
- 4Buuren S Groothuis-Oudshoorn CMICE: multivariate imputation by chained equations in R Journal of Statistical Software 201110.18637/jss.v 045.i 03 · doi ↗
- 5Ceban F Ling S Lui LMW Lee Y Gill H Teopiz KM Rodrigues NB Subramaniapillai M Di Vincenzo JD Cao B Lin K Mansur RB Ho RC Rosenblat JD Miskowiak KW Vinberg M Maletic V Mc Intyre RS Fatigue and cognitive impairment in post-COVID-19 syndrome: A systematic review and meta-analysis Brain, Behavior, and Immunity 20221019313510.1016/j.bbi.2021.12.02034973396 PMC 8715665 · doi ↗ · pubmed ↗
- 6Chen C Haupert SR Zimmermann L Shi X Fritsche LG Mukherjee B Global prevalence of post-coronavirus disease 2019 (COVID-19) condition or long COVID: A meta-analysis and systematic review Journal of Infectious Diseases 202222691593160710.1093/infdis/jiac 13635429399 PMC 9047189 · doi ↗ · pubmed ↗
- 7Delamarre L Gollion C Grouteau G Rousset D Jimena G Roustan J Gaussiat F Aldige E Gaffard C Duplantier J Martin C Fourcade O Bost C Fortenfant F Delobel P Martin-Blondel G Pariente J Bonneville F Geeraerts T Neuro ICURGCOVID-19-associated acute necrotising encephalopathy successfully treated with steroids and polyvalent immunoglobulin with unusual Ig G targeting the cerebral fibre network Journal of Neurology, Neurosurgery and Psychiatry 20209191004100610.1136/jnnp-2020-32367832651243 PMC 7476305 · doi ↗ · pubmed ↗
- 8Flanagan EP Mc Keon A Lennon VA Boeve BF Trenerry MR Tan KM Drubach DA Josephs KA Britton JW Mandrekar JN Lowe V Parisi JE Pittock SJ Autoimmune dementia: Clinical course and predictors of immunotherapy response Mayo Clinic Proceedings 2010851088189710.4065/mcp.2010.032620884824 PMC 2947960 · doi ↗ · pubmed ↗