Investigating efficacy of colchicine plus phenolic monoterpenes fraction as a potential treatment for patients diagnosed with COVID-19: A randomized controlled parallel clinical trial
Siavash Vaziri, Alireza Janbakhsh, Mohammad Hossein Zamanian, Yadollah Shakiba, Shayan Mostafaei, Amir Hossein Norooznezhad, Kamran Mansouri, Ahmad Bagheri, Farhad Abdali, Kavyan Fatahpour, Ali Mostafaie

TL;DR
This study found that adding colchicine and phenolic monoterpenes to standard care reduced mortality and hospitalization time in COVID-19 patients.
Contribution
The study introduces a novel combination therapy of colchicine and phenolic monoterpenes for treating COVID-19.
Findings
The intervention group had significantly lower mortality rates during hospitalization and follow-up.
ICU admission rates were significantly lower in the intervention group.
Hospitalization duration was shorter in the intervention group with no significant side effects.
Abstract
COVID-19 now is a serious concern for the world healthcare system. This study aimed to investigate possible therapeutic effect of colchicine and phenolic monoterpenes accompanied by standard care of treatment (SCT) in patients diagnosed with COVID-19. In this randomized controlled parallel clinical trial, a total number of 179 (of 200) patients with confirmed COVID-19 were enrolled according to the inclusion and exclusion criteria. The patients were allocated by simple randomization method into two groups control (receiving SCT with 71 patients) and intervention (receiving SCT plus colchicine and phenolic monoterpenes with 107 patients). The mortality ratio during hospitalization as well as a 2-week follow-up, ICU admission rate, and hospitalization duration were assessed as main outcomes. The mortality ratio was 0.9% (1/108) and 8.45% (6/71) in the intervention and the control groups…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
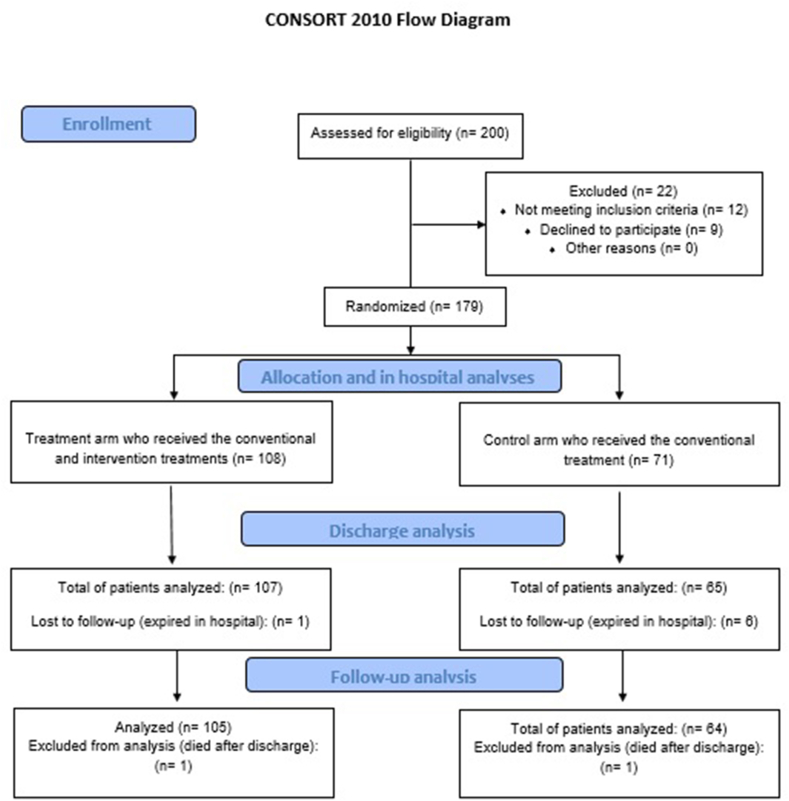 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · SARS-CoV-2 and COVID-19 Research · Phytochemicals and Medicinal Plants
Introduction
1
Coronavirus disease 2019 (COVID-19) which started in China in late 2019, led to a pandemic emergency according to the declaration of the World Health Organization (WHO). This disease has infected millions of people and caused many morbidities and even mortality. COVID-19 which is caused by a virus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may cause different signs and symptoms in different age groups [1]. The main clinical manifestation of COVID-19 has been known to be pneumonia [2], however, this disease could cause different morbidities such as acute respiratory distress syndrome (ARDS), septic shock, acute kidney injury, acute cardiac injury, heart failure, and hepatic failure [3]. Despite the clinical manifestation, different findings such as changes in leukocyte count, lymphopenia, decrease in absolute neutrophil count, and elevated levels of C reactive protein (CRP) have been seen in the primary laboratory investigation of patients diagnosed with COVID-19 [4]. Other than clinical trials performed on available medications, different trials have been performed on natural-derived products on patients with COVID-19 [5]
This randomized controlled parallel clinical trial aimed to investigate possible efficacy of colchicine plus phenolic monoterpenes fractions as a potential side treatment for patients diagnosed with COVID-19.
Methods and patients
2
Study design
2.1
This randomized controlled parallel clinical trial was performed in two COVID-19 special hospitals in Kermanshah, Iran from April 2020 to December 2020. Inpatients individuals older than 10 years old with a confirmed diagnosis of COVID-19 according to the SARS-CoV-2 real-time polymerase chain reaction (RT-PCR) and/or lung computed tomography (CT) scan were evaluated for further assessments. The exclusion criteria were defined as pregnancy and severe chronic liver disease. Patients who met both inclusion and exclusion criteria enrolled in the study and allocated in a ratio of 1.5 to 1 (intervention to control) through simple randomization method (Fig. 1).Fig. 1. Study design and protocol.Fig. 1
Ethics
2.2
The aims and methods of this study were clearly explained to patients or their legal guardians (in case of being less than 18 years old) according to their level of knowledge and education and they were asked to sign a consent form freely following the explanations. This study was approved by the Medical Ethics Committee of Kermanshah University of Medical Sciences. Also, it has been recorded in the Iranian Registry of Clinical Trial (IRCT20150623022884N3) and clinicaltrials.gov (NCT04392141). All the authors adhered to the Helsinki 1964 Declaration and its further revisions.
Definitions
2.3
Fever was defined according to the guidelines by the Centers for Disease Control and Prevention (CDC) [6] and the Iranian Ministry of Health and Medical Education [7] as body temperature of >38 °C and >37.8 °C respectively. The severe COVID-19 was defined according to the National Institute of Health (NIH) definition [8].
Intervention materials
2.4
The control group received standard care of treatment (SCT) according to the university guideline which was lopinavir/ritonavir (Kaletra®). The intervention groups received a combination of colchicine plus phenolic monoterpenes. The phenolic monoterpenes were extracted from Nigella sativa and Trachyspermum ammi based on a total phenolic standard. Also, colchicine was extracted from Colchicum autumnale. The intervention group received a total of 0.8 mg/day of colchicine as well as 45 mg of the mentioned extracted phenolic monoterpenes plus Kaletra®. The duration of the treatment of colchicine plus phenolic monoterpenes was 12 days. The intervention treatments were provided by Zist Tolid Razi Co (Kermanshah, Iran).
Data collection
2.5
The demo-biographic data (sex and age), as well as any underlying condition, were collected from the patients’ files. Patients in each group were evaluated for COVID-19-related signs and symptoms on the admission day. Also, complete blood count (CBC) variables, C reactive protein (qualitative), and lactate dehydrogenase (LDH) were investigated among the routine laboratory evaluations. Hospitalization duration, intensive care unit (ICU) admission, and mortality ratio were considered as the main outcomes. Moreover, changes in the signs including body temperature and SpO_2_ evaluated in both groups on the third day of receiving treatment and discharge/death day (compared to their admission time as the baseline).
Statistical analysis
2.6
All the data were collected in Microsoft Excel (Microsoft®) and controlled by two investigators separately. The continuous and categorical variables were presented as mean ± standard deviation (SD) and N (%) respectively. After checking the normality assumption, independent-sample T-test and paired T-test were used for comparing the continuous variables between groups and before and after analyses, respectively. Also, Chi-square/Fisher exact test was applied to assess the associations of the categorical variables and both groups. Data analyses were performed by SPSS version 25 (SPSS Inc, Chicago, IL, USA). The significance level was set at the level of 0.05.
Results
3
Baseline characteristic
3.1
According to both inclusion and exclusion criteria from a total number of 200 patients, 179 individuals were included in the trial. For the SCT and intervention groups, 71 and 108 patients were allocated, respectively. The control group's mean age was 54.21 ± 15.39 which had no significant difference (p-values = 0.527) compared to the intervention group (52.71 ± 15.52). Also, the ratio of females in the control and intervention groups were 37 (52.1%) and 55 (50.9%) respectively which showed no statistical differences for gender (p-values = 0.876) among the two arms. In control and intervention groups, 36 (50.7%) and 62 (57.4%) (respectively) of patients had underlying diseases such as hypertension, diabetic mellitus, asthma, and malignancy which revealed no statistically significant difference (p-value = 0.378) between the groups. The details of underlying diseases/disorders have been provided in Table 1. Also, primary evaluations at admission of the patients showed no statistically significant difference in variables including leukocyte and lymphocyte number, platelet count, hemoglobin (Hb) and LDH levels, and body temperature (all p-values> 0.05) between the groups. However, regarding the SpO_2_, the control group (87.39 ± 6.32) has a significantly lower mean (p-values< 0.001) compared to the intervention group (90.94 ± 3.27) at the admission phase. Considering this finding, the severity of the disease was investigated between the groups according to the NIH guideline [8], which showed that 62 (88.57%) and 90 (83.33%) individuals in the control and the intervention groups had a severe illness which revealed no significant difference (p-values = 0.510) between the groups.Table 1. Demographic and underlying diseases in the control and SCT intervention groups.Table 1. VariableControl (n = 71)Intervention (n = 108)P-valueAge (years)54.21 ± 15.3952.71 ± 15.520.527Female37 (52.1%)55 (50.9%)0.876Male34 (47.9%)53 (49.1%)Underlying disease (overall)36 (50.7%)62 (57.4%)0.378Hypertension12 (16.9%)26 (24.0%)0.251Other cardiovascular diseases5 (7.0%)11 (10.2%)0.596Diabetic mellitus5 (7.0%)11 (10.2%)0.596Asthma1 (1.4%)2 (1.8%)>0.999Malignancy2 (2.8%)7 (6.4%)0.322End stage renal disease/CKD3 (4.2%)9 (8.3%)0.368Immunosuppressive diseases01 (0.9%)>0.999Autoimmune diseases4 (5.6%)10 (9.2%)0.571Chronic liver diseases1 (1.4%)5 (4.6%)0.405Hypothyroidism01 (0.9%)>0.999Hyperthyroidism1 (1.4%)00.397Anemia02 (1.8%)0.519Recent pneumonia4 (5.6%)8 (7.4%)0.766Smoking/Substance abuse2 (2.8%)12 (11.1%)0.049Sever to critically ill COVID-1962/71 (87.3%)90/107 (84.1%)0.510
Clinical outcomes
3.2
As mentioned, different clinical variables in both groups were studied during the hospitalization period. The mortality ratio in this duration in the intervention group (1/108 [0.9%]) represented a significantly lower ratio (p-values = 0.035) compared to the control group (6/71 [8.45%]). Moreover, the accumulative mortality ratio after 14 days follow-up following discharge was significantly lower (p-values = 0.031) in the intervention group (2/108 [1.85%]) compared to the control arm (7/71 [9.85%]). Also, in the intervention group, a significant decrease in ICU admission was observed compared to the control group (2/108 [1.85%] vs. 10/71 [14.08%] respectively, p-values = 0.006). Furthermore, the intervention group (4.17 ± 1.34 days) showed to has a significantly (p-value< 0.001) lower hospitalization duration than the control arm (6.93 ± 2.59 days). Regarding the other clinical variables, statistical analyses showed a narrow p-value of 0.051 for the difference in SpO_2_ levels in the intervention (93.49 ± 2.12%) and the control groups (92.98 ± 1.76%) at the discharge moment. The details of clinical outcomes have been provided in Table 2. According to Supplementary Tab. 1, there was no serious side effect in the intervention group compared to the control arm (p values > 0.05).Table 2. Clinical outcomes of the studied groups.Table 2. ParameterIntervention (n = 108)Control (n = 71)Odds ratio (95% CI)P-valueMortality rate (during hospitalization)1 (0.9%)6 (8.45%)9.87 (1.16–83.89)0.035Mortality rate (After 14 days follow-up)2 (1.85%)7 (9.85%)5.79 (1.16–28.76)0.031ICU admission rate2 (1.85%)10 (14.08%)8.68 (1.84–40.95)0.006Hospitalization Duration (Days)4.17 ± 1.346.39 ± 2.59Not applicable**<0.001SpO_2_ (%)Admission90.94 ± 3.2787.39 ± 6.32Not applicable<0.001Discharge93.49 ± 2.1292.89 ± 1.76Not applicable0.051Body temperature (°C)Admission37.74 ± 0.4337.67 ± 0.40Not applicable0.695Discharge37.37 ± 0.3837.0 ± 0.41Not applicable0.004**95% CI: 95% confidence interval. ***: P-value<0.001 for before and after evaluation of each variable.
Paraclinical outcomes
3.3
As mentioned, different laboratory variables were evaluated in the studied groups. Discharge absolute lymphocyte count in the intervention group (1.74 ± 0.83 cells × 10^3^/mm^3^) was significantly (p value < 0.001) higher than the control group (1.17 ± 0.49 cells × 10^3^/mm^3^). Also, similar results were observed for the discharge lymphocyte to leukocytes ratio (27.0 ± 9.38 vs 18.66 ± 8.55, p value < 0.001). Moreover, LDH levels at discharge were significantly lower (p-value = 0.004) in the intervention group (542.94 ± 225.67 U/L) compared to the SCT group (691.04 ± 299.09 U/L). Furthermore, the statistically significant increase in the mean of absolute lymphocyte count (p value < 0.001) and lymphocyte to leukocytes ratio (p value < 0.001) as well as a decrease in the LDH levels (p value < 0.001) compared to their baseline levels were only observed in the intervention group (details have been provided in Table 3). The significance of differences between admission and discharge values of laboratory variables in each group have been shown in Table 3).Table 3. Comparisons of laboratory tests between the studied groups.Table 3. ParameterTimeIntervention (n = 108)Control (n = 71)P-valueLeukocyte × 10^3^/mm^3^Admission7.08 ± 3.657.11 ± 3.570.954Discharge6.87 ± 3.577.35 ± 3.700.415Lymphocytes/leukocyte (%)Admission20.91 ± 8.8219.55 ± 7.980.323Discharge27.0 ± 9.3818.66 ± 8.55<0.001Absolute lymphocytes × 10^3^/mm^3^Admission1.31 ± 0.641.19 ± 0.450.175Discharge1.74 ± 0.831.17 ± 0.49**<0.001Platelet × 10^3^/mm^3^Admission199.82 ± 115.62200.26 ± 104.340.980Discharge224.08 ± 112.42222.80 ± 86.150.939Hemoglobin (gr/dL)Admission12.0 ± 2.2112.55 ± 1.920.594Discharge11.43 ± 2.0511.59 ± 1.710.159LDH (U/L)Admission680.27 ± 471.44664.98 ± 295.840.836Discharge542.94 ± 225.67691.04 ± 299.090.004**P-value<0.05, **P-value<0.01, and ***P-value<0.001 represent p-values for difference changes between before/admission and after/discharge analysis for each variable of a group.
Discussion
4
This randomized controlled clinical trial showed that SCT plus colchicine and phenolic monoterpene-rich fractions seem to be more effective just than SCT. The intervention groups had a lower mortality ratio in both hospitalization duration and 2-week follow-up. Also, the admission to ICU was lower in the intervention group compared to the controls. Moreover, the intervention group showed important significant improvement in different assessed laboratory variables.
As mentioned, both groups had no statistically significant difference in age, sex, and underlying diseases (overall and one by one). The only difference observed was in the SpO_2_ levels which we have decided to evaluate the disease severity according to the NIH criteria [8] that showed no statistically significant difference among the groups regarding the frequency of patients with severe state of disease. As the results showed, the mortality ratio during hospitalization in the control group was 8.45% which was very similar to the obtained results of 431 hospitalized patients with COVID-19 (9%) reported in the same city and same condition [1]. Thus, it seems that despite the lower number of controls compared to the intervention group, the controls were the well-represented target population.
A randomized controlled trial on the efficacy of colchicine in patients diagnosed with COVID-19 in two groups of intervention (55 cases) vs. standard care of treatment (50 cases) showed significant improvement in time to clinical deterioration. They found event-free 10-day survival for control and intervention groups were 83% vs. 97% (p-value = 0.03) respectively [9]. Moreover, another randomized, double-blinded, placebo-controlled clinical trial has been performed on colchicine and COVID-19 in two 36 cases arms. It has been shown that colchicine was able to significantly reduce the need for supplemental oxygen and length of hospitalization in the intervention group compared to the controls [10]. Also, another randomized control clinical trial is now conducting on the potential of Nigella sativa supplementation to treat symptomatic mild COVID-19 but no result has been published for it. It has been stated that Nigella sativa oil (MARNYS® Cuminmar) softgel in dosage of 500 mg each 12-h (BID) for ten days [11].
Colchicine is a well-known anti-inflammatory agent that has been used in medicine for a long time. In the therapeutic dose, colchicine could decrease crucial steps of inflammation such as migration, degranulation, and cell-cell attachment in the inflammatory-related cells especially macrophages and neutrophils [12]. The phenolic monoterpenes such as thymoquinone have shown strong antioxidant and anti-inflammatory properties [13]. Using the phenolic monoterpenes along with colchicine not only synchronously increases the anti-inflammatory action of colchicine but also might decrease any possible cytotoxic effect. Also, the anti-oxidant role of phenolic monoterpenes should not be ignored [13] since oxidative stress is a key role player in the many aspects of COVID-19 pathogenesis [14] especially endothelial dysfunction that leads to thromboembolic events [15].
As same as any other study, this one has its limitations. The main limitation of this study was the low sample size of the studied patients. Also, the current study used colchicine plus phenolic monoterpenes fraction which the exact compounds of phenolic monoterpenes fraction are not well-known. Moreover, the current investigation was an open-label clinical trial which could be another limitation.
Although the results of the study were suggestive to using the mixture of colchicine accompanied by phenolic monoterpenes as a possible treatment for COVID-19, it seems further studies such as double-blinded randomized control trials on both inpatients and outpatients are necessary. One of the missing points of this study was the lack of some laboratory data such as interleukin 6 (IL-6), quantitative C-reactive protein, and cardiac troponin values which should be evaluated in further studies.
Conclusion
5
According to the results, the combination of colchicine and phenolic monoterpenes could be a possible side treatment for COVID-19. This treatment option showed decrease in mortality ratio, ICU admission rate, and hospitalization duration in the treated patients. The authors of this study suggest further investigations on this mixture as a potential co-treatment for COVID-19.
Funding
This study was funded by Zist Tolid Razi Co (Kermanshah, Iran).
CRediT authorship contribution statement
Siavash Vaziri: Writing – review & editing, Writing – original draft, Project administration, Investigation, Data curation. Alireza Janbakhsh: Writing – review & editing, Writing – original draft, Investigation. Mohammad Hossein Zamanian: Writing – review & editing, Writing – original draft, Investigation. Yadollah Shakiba: Writing – review & editing, Writing – original draft, Investigation. Shayan Mostafaei: Writing – review & editing, Writing – original draft, Visualization, Software, Methodology. Amir Hossein Norooznezhad: Writing – review & editing, Writing – original draft, Methodology, Investigation. Kamran Mansouri: Writing – review & editing, Writing – original draft, Investigation. Ahmad Bagheri: Writing – review & editing, Writing – original draft, Investigation. Farhad Abdali: Writing – review & editing, Writing – original draft, Investigation. Kavyan Fatahpour: Writing – review & editing, Writing – original draft, Investigation. Ali Mostafaie: Writing – review & editing, Writing – original draft, Project administration, Investigation, Funding acquisition, Data curation, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Norooznezhad A.H.Najafi F.Riahi P.Moradinazar M.Shakiba E.Mostafaei S.Primary symptoms, comorbidities, and outcomes of 431 hospitalized patients with confirmative RT-PCR results for COVID-19Am. J. Trop. Med. Hyg.10320208348373258880110.4269/ajtmh.20-0512 PMC 7410435 · doi ↗ · pubmed ↗
- 2Hantoushzadeh S.Norooznezhad A.H.Inappropriate antibiotic consumption as a possible cause of inflammatory storm and septic shock in patients diagnosed with coronavirus-19 disease (COVID-19)Arch. Med. Res.5120203473483234075910.1016/j.arcmed.2020.03.015PMC 7129207 · doi ↗ · pubmed ↗
- 3Zhou F.Yu T.Du R.Fan G.Liu Y.Liu Z.Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study Lancet 3952020105410623217107610.1016/S 0140-6736(20)30566-3PMC 7270627 · doi ↗ · pubmed ↗
- 4Norooznezhad A.H.Eskandarion S.Akbari R.Alimohammadi S.Nabavian S.M.Giti S.Changes of leukocytes, neutrophils, and lymphocytes count and dependent variables in pregnant women with coronavirus disease 2019 (COVID-19) before and after cesarean delivery J. Med. Virol.2202166466610.1002/jmv.2652532940910 · doi ↗ · pubmed ↗
- 5Ang L.Song E.Lee H.W.Lee M.S.Herbal medicine for the treatment of coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis of randomized controlled trials J. Clin. Med.9202015833245612310.3390/jcm 9051583 PMC 7290825 · doi ↗ · pubmed ↗
- 6Centers for Disease Control and Prevention (CDC)Definitions of Symptoms for Reportable Illnesses 2020 https://wwwcdcgov/quarantine/air/reporting-deaths-illness/definitions-symptoms-reportable-illnesseshtml
- 7Ministry of Health and Medical Education[Instructions for diagnosis and care tof COVID-19 in selected comprehensive health centers]http://treatmentsbmuacir/uploads/2-2-montakhab_salamatzip 2020
- 8National Institute of Health (NIH)Management of Persons with COVID-192020 https://wwwcovid 19treatmentguidelinesnihgov/overview/management-of-covid-19