Thrombotic ST-segment elevation myocardial infarction caused by a caseous mitral annular calcification
Baravan Al-Kassou, Marcel Weber, Georg Nickenig, Sebastian Zimmer

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
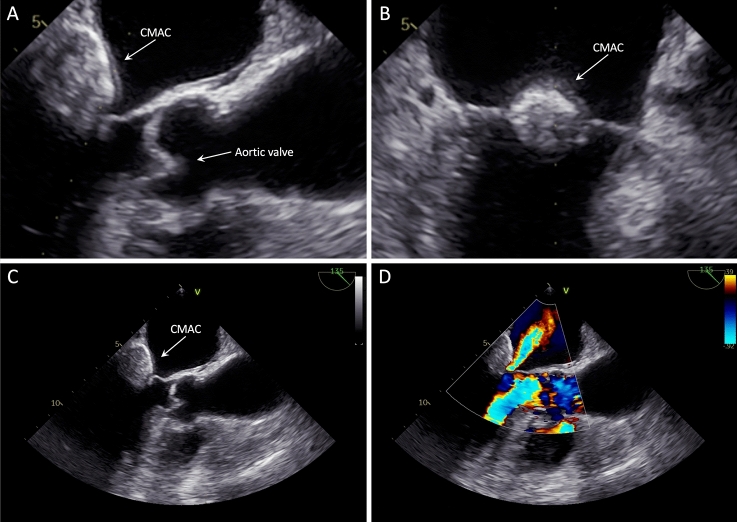 Figure 1
Figure 1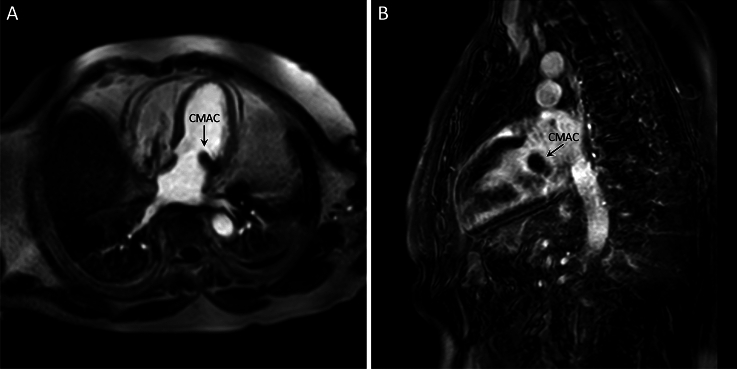 Figure 2
Figure 2- —Rheinische Friedrich-Wilhelms-Universität Bonn (1040)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Cardiac Structural Anomalies and Repair
Sirs:
A 73-year-old patient was admitted to the emergency department for an ST-segment elevation myocardial infarction. The patient reported sudden onset of persisting chest pain and dyspnea for three hours. The clinical history of the patient included diabetes, arterial hypertension, and prior stroke in the year 2002.
Initial 12-lead electrocardiogram (ECG) showed sinus rhythm with posterior and inferior ST-segment elevation. The transthoracic echocardiography revealed inferior and lateral hypokinesia of the left ventricle. Moreover, a large, echo-dense mass with central echolucency and well-defined calcified margins was detectable.
Emergency coronary angiography via transradial approach revealed a thrombus in the proximal left circumflex artery. Except for the proximal embolic occlusion, adequate blood flow was detectable in the distal artery. Furthermore, the coronary arteries were free of atheromatous lesions. After thrombus resolution with heparin and tirofiban, recovery of ST segment elevation and improvement in clinical symptoms were observed.
Diagnostic work-up for differentiation of the cardiac tumor included transesophageal echocardiography (TEE), that showed a well-circumscribed, smooth-bordered echo-dense mass (2.9 × 1.9 cm) at the posterior peri-annular region of the mitral valve, containing central echolucency and suspicious for a caseous mitral annular calcification (CMAC, Fig. 1A–C). The color flow Doppler detected a mild mitral regurgitation with a mean pressure gradient of 3.0 mmHg (Fig. 1D). The subsequent cardiac magnetic resonance revealed a calcified caseous formation of the mitral valve annulus adjacent to the posterior mitral valve leaflet, that was hypointense in both T1- and T2-weighted sequences without early or late contrast enhancement, confirming the suspected diagnosis of CMAC (Fig. 2A–B).Fig. 1. Transesophageal echocardiography showing a well-defined, smooth-bordered echo-dense mass with central echolucency at the posterior peri-annular region of the mitral valve causing a mild mitral regurgitation. CMAC caseous mitral annular calcificationFig. 2Cardiac magnetic resonance revealing a T1- and T2-weighted hypointense, calcified caseous formation of the mitral valve annulus, without early or late contrast enhancement. CMAC caseous mitral annular calcification
Other potential sources of coronary embolism, such as infective endocarditis and left atrial appendage thrombus have been excluded by TEE. Furthermore, no atrial fibrillation or flutter was detectable during prolonged ECG Holter monitoring.
CMAC is a rare variant of the mitral annular calcification, a chronic degenerative process of the fibrous mitral annulus that occurs at advanced age [1–3]. Histopathologically, CMAC is characterized by a liquefaction necrosis of the central region with amorphous eosinophilic acellular material, that is surrounded by macrophages and lymphocytes and bordered by multiple calcifications [4]. Although secondary consequences such as mitral valve regurgitation or stenosis caused by CMAC have been reported, a conservative approach is generally recommended due to the general benign prognosis [5–7]. However, patients with CMAC are at increased risk of arterial thromboembolism, especially embolic strokes, that are not related to atrial fibrillation [8]. The suspected pathomechanism of systemic embolism include embolization of calcium and cholesterol particles, surface ulceration with subsequent thrombus formation and embolization as well as fistulation of caseous necrotic material into the left atrium or ventricle (8, 9).
The reported case demonstrates the potentially life-threatening complication that may arise from CMAC. Thus, close clinical follow-up with multi-center research focusing on possible consequences of CMAC and a critical evaluation for oral anticoagulation is warranted. In the present case, the heart team recommended surgical resection of the tumor, which the patient declined. Therefore, oral anticoagulation with a non-vitamin K agent was initiated to prevent further thromboembolic events.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (MP4 5423 KB) Transesophageal echocardiography acquisition of caseous mitral annular calcification with mitral regurgitation Supplementary file2 (MP4 3710 KB) Transesophageal echocardiography acquisition of caseous mitral annular calcification with mitral regurgitationSupplementary file3 (MP4 2195 KB) Transesophageal echocardiography acquisition of caseous mitral annular calcification with mitral regurgitationSupplementary file4 (MP4 2584 KB) Transesophageal echocardiography acquisition of caseous mitral annular calcification with mitral regurgitationSupplementary file5 (MP4 2426 KB) Coronary angiography videos of the patient including follow-up angiogram after thrombus resolution.Supplementary file6 (MP4 2352 KB) Coronary angiography videos of the patient including follow-up angiogram after thrombus resolution.Supplementary file7 (MP4 2689 KB) Coronary angiography videos of the patient including follow-up angiogram after thrombus resolution.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Churchill TW Yucel E Deferm S Levine RA Hung J Bertrand PB Mitral valve dysfunction in patients with annular calcification: JACC review topic of the week J Am Coll Cardiol 20228073975110.1016/j.jacc.2022.05.03235953139 PMC 10290884 · doi ↗ · pubmed ↗
- 2Chehab O Roberts-Thomson R Bivona A Management of patients with severe mitral annular calcification: JACC state-of-the-art review J Am Coll Cardiol 20228072273810.1016/j.jacc.2022.06.00935953138 · doi ↗ · pubmed ↗
- 3Curl E Riemer E Caseous calcification of the mitral annulus: case report and brief review Eur Heart J Case Rep 2018212410.1093/ehjcr/yty 124PMC 642607231020200 · doi ↗ · pubmed ↗
- 4Harpaz D Auerbach I Vered Z Motro M Tobar A Rosenblatt S Caseous calcification of the mitral annulus: a neglected, unrecognized diagnosis J Am Soc Echocardiogr 20011482583110.1067/mje.2001.11187711490332 · doi ↗ · pubmed ↗
- 5Elgendy IY Conti CR Caseous calcification of the mitral annulus: a review Clin Cardiol 201336 E 273110.1002/clc.2219924038099 PMC 6649616 · doi ↗ · pubmed ↗
- 6Mayr A Muller S Feuchtner G The spectrum of caseous mitral annulus calcifications JACC Case Rep 2021310410810.1016/j.jaccas.2020.09.03934317479 PMC 8305068 · doi ↗ · pubmed ↗
- 7Movahed MR Saito Y Ahmadi-Kashani M Ebrahimi R Mitral annulus calcification is associated with valvular and cardiac structural abnormalities Cardiovasc Ultrasound 200751410.1186/1476-7120-5-1417359540 PMC 1838405 · doi ↗ · pubmed ↗
- 8Dietl CA Hawthorn CM Raizada V Risk of cerebral embolization with caseous calcification of the mitral annulus: review article Open Cardiovasc Med J 20161022123210.2174/187419240161001022127990181 PMC 5120388 · doi ↗ · pubmed ↗