Clinical-histopathological features and cancer gene analysis of cutaneous epithelioid angiosarcoma: A report of 4 cases
Keiko Tokuchi, Teruki Yanagi, Suguru Kurosawa, Shinya Kitamura, Takuya Maeda, Che Yuan Hsu, Kodai Miyamoto, Hiroshi Nishihara, Hideyuki Ujiie

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
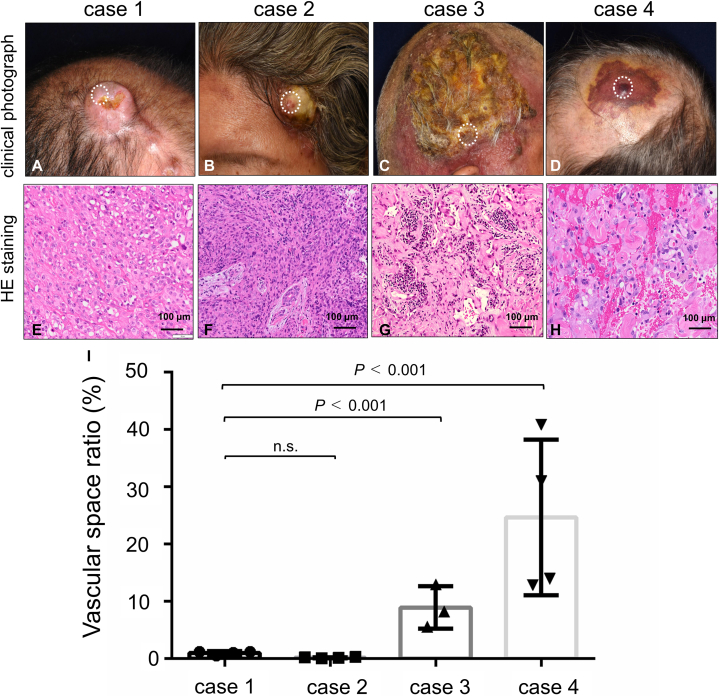 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Sarcoma Diagnosis and Treatment · Cardiac tumors and thrombi
Introduction
Angiosarcoma (AS) is a rare variant of malignant soft tissue sarcoma, representing less than 1% of all soft tissue sarcomas.1 Among the histopathological subtypes of AS, epithelioid angiosarcoma (EAS) is characterized by epithelioid morphology, with polygonal or spherical cells containing eosinophilic cytoplasm.2 Tumors where over 80% of the cells are epithelioid are typically classified as EAS.3 EAS usually manifests during adulthood, particularly around the seventh decade of life.2 Approximately 12% of cutaneous AS is cutaneous EAS, yet detailed studies on clinical presentations are lacking.2 In this study, we report 4 cases of EAS and analyze the vascular space in biopsy specimens to investigate correlations between clinical and histopathological findings. Additionally, we conducted cancer gene analyses using two EAS cases and three AS cases, and we detected no notable genetic differences between EAS and conventional AS tumors.
Case report
We report 4 individuals diagnosed with EAS (Supplementary Table I, available via Mendeley at https://doi.org/10.17632/rvs83cnfph.1; Fig 1, A-D). In all cases, skin biopsies revealed a solid sheet of polygonal or round tumor cells with eosinophilic cytoplasm and intracytoplasmic lumina formations (Fig 1, E-H). Immunohistochemically, the tumor cells in all cases were positive for CD31 but negative for smooth muscle actin, S-100, Melan-A, and HMB-45 (not shown). Consequently, all 4 cases were diagnosed as cutaneous EAS. Purpura was not observed in the lesions of 2 of the 4 cases (cases 1 and 2), whereas purpura was observed in the others (cases 3 and 4). To analyze the correlation between clinical manifestations and histopathological findings, we examined the histopathological vascular space in the skin biopsy specimens. The vascular space ratio, defined as the ratio of the vascularized channel area to the total high-power view area, was calculated using Image J software (https://imagej.nih.gov/ij/).4 The vascular space ratio was 1.10% for case 1, 0.19% for case 2, 8.95% for case 3, and 24.67% for case 4, indicating that tumors with a high amount of vascular space tend to display purpura (Fig 1, I). For the genomic analyses of the EAS tumors, we performed somatic gene mutation analysis of cancer-associated genes for 2 of the EAS cases (case 1 and case 3) and for 2 conventional AS cases (both 81-year-old males), as well as for 1 case of Stewart-Treves syndrome (lymphedema-associated AS, an 89-year-old female) (Table I, Supplementary Table II, available via Mendeley at xxx, Institutional Review Board approval #15-029). In both EAS cases, loss-of-function mutations in tumor protein 53 (TP53) were detected. Additionally, loss of heterozygosity of cyclin-dependent kinase inhibitor 2A (case #1) and amplification of guanine nucleotide-binding protein alpha subunit (case #3) were observed. One of the 2 conventional AS cases showed a v-myc avian myelocytomatosis viral related oncogene, neuroblastoma derived homolog mutation (ClinVar: likely pathogenic), and the other case showed loss of heterozygosity of cyclin-dependent kinase inhibitor 2A and TP53 with a high tumor mutation burden (11 mutants/Mbp). The case with Stewart-Treves syndrome exhibited amplification of the MYC oncogene, consistent with previous studies.5 The data suggests that gene mutations in EAS resemble those in AS, including loss-of-function mutations of tumor suppressor genes (TP53 and cyclin-dependent kinase inhibitor 2A).Fig 1. Clinical and histopathological findings of the present 4 cutaneous epithelioid angiosarcomas. A to D, Clinical photographs of the present cases. Dotted circles indicate biopsy sites. E to H, Histopathological findings. Scale bar = 100 μm. Hematoxylin and eosin staining. I, A bar graph indicates the vascular space ratio for each case. These ratios were calculated using Image J software. We photographed high-power view images randomly and colored vascular channels manually to calculate the vascular space ratio (n = 3 or 4, mean ± SD, t test).Table IActionable mutations of epithelioid angiosarcoma, conventional angiosarcoma, Stewart-Treves syndromeEpithelioid AS #1GeneAA ChangeSAFCNAeCNTP53p.Y220C0.31707317HD−0.3KEAP1Wild typeHD−0.2TP53Wild typeHD−0.3TSC1Wild typeHD−0.2PMS2Wild typeLOH0.2BRCA1Wild typeLOH0.5BRCA2Wild typeLOH0.7CHEK2Wild typeLOH0.5PALB2Wild typeLOH0.5CDKN2AWild typeLOH0.9SMARCB1Wild typeLOH0.8POLD1Wild typeLOH0.7STK11Wild typeLOH0.9VHLWild typeLOH0.3FANCAWild typeLOH0.5CDH1Wild typeLOH0.6EP300Wild typeLOH0.6SMARCA4Wild typeLOH0.4PIK3R2Wild typeLOH0.9EPCAMWild typeLOH0.2RAD51CWild typeLOH0.2Epithelioid AS #3GeneAA ChangeSAFCNAeCNGNASWild typeAmplification14.8EZH2Wild typeAmplification4.5BRAFWild typeAmplification4.5MYCWild typeAmplification4TP53c.376-1G > A0.55555556LOH1.1BRCA2Wild typeLOH1.3TP53Wild typeLOH1.1MAP3K1Wild typeLOH1.4RB1Wild typeLOH1.4APCWild typeLOH1.4FBXW7Wild typeLOH1.4BCL2L11Wild typeLOH1.4Conventional AS #1 (TMB-high, 11 Muts/Mbp)GeneAA ChangeSAFCNAeCNFGFR4AmplificationAmplification4.5CDKN2AWild typeLOH0.6TP53Wild typeLOH1.1VHLWild typeLOH1.1KEAP1Wild typeLOH0.9Conventional AS #2GeneAA ChangeSAFCNAeCNMYCNp.P44L0.206198Neutral0.8Stewert Treves syndromeGeneAA ChangeSAFCNAeCNMYCAmplificationAmplification101.3NF1p.V1182F0.340458LOH1.1PIK3CAp.Q546K0.080696neutral2.4PALB2Wild typeLOH1KEAP1Wild typeLOH0.6NF1Wild typeLOH1.1RAD51CWild typeLOH1.2AA, Amino acid; APC, adenomatous polyposis coli; AS, angiosarcoma; BCL2L11, B-cell/CLL lymphoma 2-like 11; BRAF, v-raf murine sarcoma viral oncogene homolog B1; BRCA1, Breast cancer susceptibility gene 1; BRCA2, Breast cancer susceptibility gene 2; CDH1, cadherin 1; CDKN2A, cyclin dependent kinase inhibitor 2A; CDKN2A, cyclin-dependent kinase inhibitor 2A; CHEK2, checkpoint kinase2; CNA, copy number alteration; eCN, estimated copy number in cancer cells; EP300, E1A binding protein P300; EPCAM, epithelial cell adhesion molecule; EZH2, enhancer Of zeste 2 polycomb repressive complex 2 subunit; FANCA, Fanconi anemia complementation group A; FBXW7, F-box and WD repeat domain containing 7; FGFR4, fibroblast growth factor receptor 4; GNAS, guanine nucleotide-binding protein alpha subunit; HD, homo deletion; KEAP1, kelch like ECH associated protein 1; KEAP1, Kelch-like ECH-associated protein1; LOH, loss of heterozygosity; MAP3K1, mitogen-activated protein kinase kinase kinase 1; MYC, myelocytomatosis viral related oncogene; NF1, neurofibromin 1; PALB2, partner and localiser of BRCA 2; PALB2, partner and localizer of BRCA2; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; PIK3R2, phosphoinositide-3-kinase regulatory subunit 2; PMS2, post-meiotic segregation 2; POLD1, DNA polymerase delta1 catalytic subunit; RAD51C, RAD51 paralog C; RB1, retinoblastoma gene1; SAF, somatic allele frequency; SMARCA4, SWI/SNF-related, matrix-associated, actin-dependent regulators of chromatin A4; SMARCB1, SWI/SNF related, matrix associated, actin dependent regulator of chromatin, subfamily b, member 1; STK11, serine/threonine kinase 11; TMB, tumor mutation burden; TP53, tumor protein 53; TSC1, Tuberous sclerosis complex1; VHL, Von Hippel-Lindau tumor suppressor.
Discussion
Rosai et al first described the epithelioid phenotype of AS in 1976, with Fletcher et al establishing the current definition in 1991.6 Due to the diversity of primary sites and the incredibly aggressive nature of the tumors, only around 50 reports of cutaneous EAS are publicly available. Nodules and plaques are the most common clinical manifestations of cutaneous EAS.2^,^7 In our study, half of the EAS cases presented with nonpurpuric lesions, and all had elevated nodules or plaques on the scalp. Consistent with earlier studies, our cases displayed large polygonal epithelioid cells with eosinophilic cytoplasm. EAS tumors exhibit higher cellularity of the epithelioid tumor cells, which contributes to their unique clinical presentations, such as nodule, plaque, or tumor formation. Our findings suggest that some EAS lesions exhibit purpura due to the presence of certain vascular formations.
Several mutation analysis studies on human AS have been reported.5^,^8 Gene alterations of TP53 have been frequently reported5^,^9; thus, our cancer gene analysis results align with these previous findings. No reports on EAS-specific gene mutations exist; however, our study suggests no notable differences in cancer-associated gene mutations between EAS and conventional AS tumors.
In conclusion, we reported 4 cases of cutaneous EAS and analyzed their clinical characteristics and histopathological findings. Our study suggests that the purpuric appearance of EAS may be dependent on the vascular space formations in the EAS tumor tissue. Furthermore, our analysis of cancer-associated gene mutations indicates that EAS tumors have gene mutation profiles similar to those of conventional AS, including loss-of-function mutations in TP53.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Young R.J.Brown N.J.Reed M.W.Hughes D.Woll P.J.Angiosarcoma Lancet Oncol 1120109839912053794910.1016/S 1470-2045(10)70023-1 · doi ↗ · pubmed ↗
- 2Hart J.Mandavilli S.Epithelioid angiosarcoma: a brief diagnostic review and differential diagnosis Arch Pathol Lab Med 13520112682722128444910.5858/135.2.268 · doi ↗ · pubmed ↗
- 3Suchak R.Thway K.Zelger B.Fisher C.Calonje E.Primary cutaneous epithelioid angiosarcoma: a clinicopathologic study of 13 cases of a rare neoplasm occurring outside the setting of conventional angiosarcomas and with predilection for the limbs Am J Surg Pathol 35201160692116428810.1097/PAS.0b 013e 3181 fee 872 · doi ↗ · pubmed ↗
- 4Ozerdem U.Wojcik E.M.Duan X.Ersahin C.Barken G.A.Prognostic utility of quantitative image analysis of microvascular density in prostate cancer Pathol Int 6320132772822371425610.1111/pin.12056 · doi ↗ · pubmed ↗
- 5Goerdt L.V.Schenider S.W.Booken N.Cutaneous angiosarcomas: molecular pathologenesis guides novel therapeutic approaches J Dtsch Dermatol Ges 20202242944310.1111/ddg.1469435218306 · doi ↗ · pubmed ↗
- 6Fletcher C.D.Beham A.Bekir S.Clarke A.M.Marley N.J.Epithelioid angiosarcoma of deep soft tissue: a distinctive tumor readily mistaken for an epithelial neoplasm Am J Surg Pathol 151991915924171817610.1097/00000478-199110000-00001 · doi ↗ · pubmed ↗
- 7Bacchi C.E.Silva T.R.Zambrano E.Epithelioid angiosarcoma of the skin: a study of 18 cases with emphasis on its clinicopathologic spectrum and unusual morphologic features Am J Surg Pathol 342010133413432069724910.1097/PAS.0b 013e 3181 ee 4eaf · doi ↗ · pubmed ↗
- 8Ishida Y.Otsuka A.Kabashima K.Cutaneous angiosarcoma: update on biology and latest treatment Curr Opin Oncol 3020181071122919407510.1097/CCO.0000000000000427 PMC 5815647 · doi ↗ · pubmed ↗