Helicobacter pylori Infection and Complications of Cirrhosis
Shefali Amin, Biraj Shrestha, Ameya Deshmukh, Manish Shrestha, Parth Desai, John Altomare

TL;DR
This study explores the link between Helicobacter pylori infection and complications in patients with cirrhosis, finding higher complication rates in those with H. pylori.
Contribution
The study provides new insights into the association between H. pylori and cirrhosis-related complications using a large inpatient database.
Findings
H. pylori-infected cirrhotic patients had higher rates of complications like gastrointestinal bleeding and hepatorenal syndrome.
Despite lower in-hospital mortality, H. pylori-infected patients had longer hospital stays.
The study highlights the need for further research to determine if H. pylori causes or merely correlates with cirrhosis complications.
Abstract
Introduction: Helicobacter pylori is a significant contributor to conditions such as peptic ulcer disease, gastric cancer, gastric mucosa-associated lymphoid tissue lymphoma, and colorectal cancer. Recent studies have suggested a potential link between H. pylori and cirrhosis. However, the impact of H. pylori on cirrhosis-related mortality, inpatient outcomes, and decompensating events remains unclear. Considering the widespread availability of H. pylori testing and effective treatment options, there is a potential rationale for eradicating H. pylori in cirrhotic patients to mitigate the morbidity and mortality associated with cirrhosis. This study aims to investigate the association between H. pylori and inpatient outcomes and complications related to cirrhosis. Methods: The National Inpatient Sample (NIS) database, a part of the Healthcare Cost & Utilization Project, was utilized for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
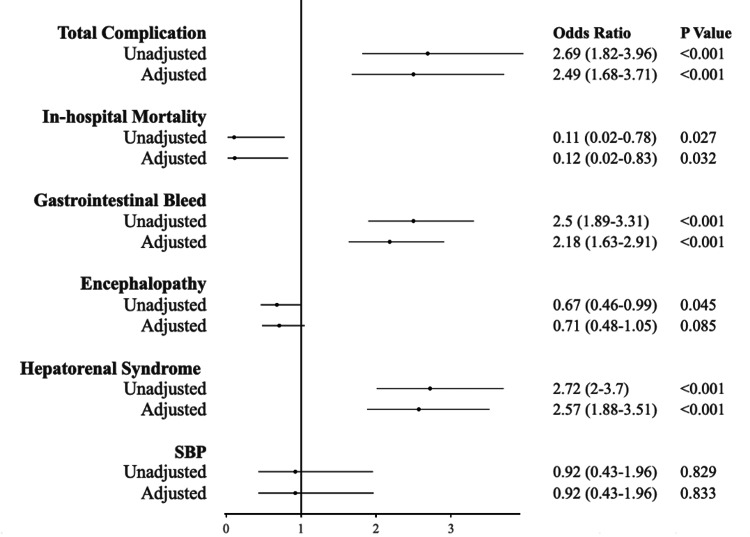 Figure 1
Figure 1| Baseline Characteristics | Overall (%) (N = 416,410) |
|
| P-value |
| Cirrhosis | ||||
| Mean Age, (Mean ± Standard error) (Years) | 57.17 (57.07 - 57.27) | 57.18 (57.08 - 57.28) | 54.25 (52.55 - 55.95) | 0.001 |
| Age (years) | 0.01 | |||
| • 18-49 | 24.73 | 24.71 | 33.84 | 0.01 |
| • 50-64 | 49.61 | 49.61 | 47.47 | 0.01 |
| • 65-74 | 17.83 | 17.84 | 12.12 | 0.01 |
| •>= 75 | 7.84 | 7.84 | 6.57 | 0.01 |
| Gender | 0.028 | |||
| • Male | 63.13 | 63.11 | 70.71 | 0.028 |
| • Female | 36.87 | 36.89 | 29.29 | 0.028 |
| Race | <0.001 | |||
| • White | 64.01 | 64.10 | 26.26 | <0.001 |
| • Black | 8.13 | 8.10 | 20.20 | <0.001 |
| • Hispanic | 18.62 | 18.58 | 36.36 | <0.001 |
| • Asian or Pacific Islander | 1.72 | 1.71 | 5.56 | <0.001 |
| • Native American | 1.50 | 1.50 | 2.53 | <0.001 |
| • Other | 6.02 | 6.02 | 9.09 | <0.001 |
| Comorbiditya | ||||
| • Obesity | 14.29 | 14.30 | 11.62 | 0.275 |
| • Body mass index (BMI) < 20 | 2.71 | 2.71 | 3.54 | 0.578 |
| • Hypertension | 49.70 | 49.71 | 42.42 | 0.042 |
| • Diabetes | 30.10 | 30.12 | 24.75 | 0.108 |
| • Hypercholesterolemia | 16.33 | 16.35 | 8.08 | 0.002 |
| • Heart failure | 11.95 | 11.96 | 7.58 | 0.059 |
| • Valvular disease | 0.74 | 0.74 | 0.51 | 0.701 |
| • Chronic kidney disease (CKD) stage 3 or more | 12.92 | 12.94 | 6.06 | 0.004 |
| • Alcohol use disorder | 48.56 | 48.53 | 61.11 | <0.001 |
| • Peripheral vascular disease | 3.72 | 3.73 | 1.52 | 0.101 |
| • Chronic obstructive pulmonary disease (COPD) | 12.94 | 12.94 | 10.61 | 0.327 |
| • Stroke | 0.58 | 0.59 | 0.00 | 0.295 |
| • Coronary artery disease (CAD) | 12.19 | 12.21 | 7.07 | 0.028 |
| • Cardiomyopathy | 2.28 | 2.28 | 2.53 | 0.818 |
| • Coagulopathy | 0.86 | 0.86 | 0.00 | 0.219 |
| • Bleeding disorder | 42.48 | 42.48 | 41.92 | 0.873 |
| • Smoking | 22.28 | 22.27 | 25.25 | 0.325 |
| • Cancer | 7.70 | 7.70 | 6.06 | 0.389 |
| • Autoimmune disease | 2.06 | 2.06 | 1.01 | 0.298 |
| Median Household Income Category for Patient's Zip Codeb | 0.0002 | |||
| • 0-25 percentile | 34.69 | 34.66 | 48.17 | 0.0002 |
| • 26-50 percentile | 26.73 | 26.73 | 24.61 | 0.0002 |
| • 51-75 percentile | 22.64 | 22.64 | 19.90 | 0.0002 |
| • 76-100 Percentile | 15.94 | 15.96 | 7.33 | 0.0002 |
| Primary Payerc | 0.002 | |||
| • Federal insurance | 65.68 | 65.68 | 65.68 | 0.002 |
| • Private insurance | 21.86 | 21.88 | 12.12 | 0.002 |
| • Other | 3.22 | 3.22 | 5.56 | 0.002 |
| • Uninsured | 9.06 | 9.05 | 15.66 | 0.002 |
| • Missing | 0.17 | 0.17 | 0.00 | 0.002 |
| Hospital Characteristics | ||||
| Hospital Region | 0.013 | |||
| • Northeast | 16.76 | 16.76 | 17.17 | 0.013 |
| • Midwest | 19.27 | 19.27 | 19.19 | 0.013 |
| • South | 43.00 | 43.02 | 33.84 | 0.013 |
| • West | 20.97 | 20.95 | 29.80 | 0.013 |
| Hospital Bed Sized | 0.025 | |||
| • Small | 17.11 | 17.11 | 13.64 | 0.025 |
| • Medium | 28.33 | 28.35 | 22.22 | 0.025 |
| • Large | 54.56 | 54.54 | 64.14 | 0.025 |
| Hospital Teaching Statuse | <0.001 | |||
| • Non-teaching | 26.42 | 26.45 | 15.15 | <0.001 |
| • Teaching | 73.58 | 73.55 | 84.85 | <0.001 |
| Hospital Location | 0.066 | |||
| • Rural | 5.51 | 5.52 | 2.53 | 0.066 |
| • Urban | 94.49 | 94.48 | 97.47 | 0.066 |
| Disposition | <0.001 | |||
| • Home | 63.25 | 63.21 | 80.30 | <0.001 |
| • Facility/others | 4.43 | 4.44 | 0.51 | <0.001 |
| • Died | 32.32 | 32.35 | 19.19 | <0.001 |
| Admission Type | 0.446 | |||
| • Non-Elective | 94.70 | 94.70 | 97.47 | 0.446 |
| • Elective | 5.14 | 5.14 | 2.53 | 0.446 |
| • Missing | 0.16 | 0.16 | 0.00 | 0.446 |
| Elixhauser Comorbidity Index for Mortality (Mean ± 95% Conf. Interval)f | -1.86 (-1.91 to -1.81) | -1.86 (-1.91 to -1.81) | -1.77 (-2.51 to -1.03) | 0.809 |
| Outcome | Overall (%) (N= 416,410) | Helicobacter pylori Absent (%) (N= 415,420) | Helicobacter pylori Present (%) (N= 990) | P-value |
| Cirrhosis | ||||
| In-hospital mortality | 4.43 | 4.44 | 0.51 | 0.007 |
| Length of stay (Mean ± Standard error) (Days) | 5.76 (5.68 - 5.83) | 5.75 (5.68 - 5.83) | 6.97 (6.21 - 7.72) | 0.002 |
| Cost of care (Mean ± Standard error) (USD) | 16547.22 (16031.09 - 17063.36) | 16543.49 (16026.53 - 17060.45) | 18106.18 (15947.94 - 20264.41) | 0.160 |
| Complicationsa | Overall (%) (N= 416,410) | Helicobacter pylori Absent (%) (N= 415,420) | Helicobacter pylori Present (%) (N= 990) | P-value |
| Cirrhosis | ||||
| Gastrointestinal bleed | 27.39 | 27.34 | 48.48 | <0.001 |
| Hepatic encephalopathy | 21.56 | 21.57 | 15.66 | 0.040 |
| Hepatorenal syndrome | 47.04 | 46.99 | 70.71 | <0.001 |
| Spontaneous bacterial peritonitis | 3.83 | 3.83 | 3.54 | 0.826 |
| Death | 4.43 | 4.44 | 0.51 | 0.007 |
| Overall complication | 67.63 | 67.59 | 84.85 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Gastric Cancer Management and Outcomes · Eosinophilic Esophagitis
Introduction
Helicobacter pylori is the most common chronic infection worldwide, affecting over 50% of the global population [1]. It is a major cause of peptic ulcer disease, gastric cancer, gastric mucosa-associated lymphoid tissue lymphoma, and colorectal cancer [2-3]. In addition, as H. pylori may induce a chronic inflammatory state, it has been linked to extraintestinal manifestations such as immune thrombocytopenic purpura, coronary artery disease, iron deficiency anemia, and migraines [4].
In recent years, clinicians have been investigating a potential link between H. pylori and cirrhosis. In one meta-analysis, patients with cirrhosis were significantly more likely to be infected with H. pylori when compared to controls [5]. However, the contribution of H. pylori to cirrhosis mortality, inpatient outcomes, and decompensating events remains unclear. Given the widespread availability of H. pylori testing and effective treatment strategies, eradicating H. pylori in cirrhotic patients may be warranted to reduce morbidity and mortality associated with cirrhosis if a link exists. The present research focuses on exploring the association between H. pylori and cirrhosis-related inpatient consequences and complications.
This article was previously presented as a meeting abstract at the 2022 American College of Gastroenterology (ACG) Annual Scientific Meeting on October 24, 2022.
Materials and methods
We used the National Inpatient Sample (NIS) database, which is part of the Healthcare Cost & Utilization Project. The national cohort database comprises data on over seven million hospital stays within the United States and reflects approximately 20% of discharges in the United States.
We extracted inpatient data for the years 2016 through 2019 (the latest year available in the database at the time of data extraction) from patients with a primary discharge diagnosis of cirrhosis as defined by ICD code B9681. Patients with concomitant diagnosis of H. pylori infection were extracted as defined by ICD code K70. Baseline characteristics were compared between H. pylori-infected and non-H. pylori-infected patients, including demographic factors (age, gender, race), comorbid conditions, Elixhauser Comorbidity Index, median household income, primary payer, hospital characteristics, disposition, and admission type. Primary outcomes were inpatient mortality, length of stay, and cost of care.
The secondary endpoints comprised complications related to cirrhosis during hospitalization, such as gastrointestinal bleeding, hepatic encephalopathy, hepatorenal syndrome, and spontaneous bacterial peritonitis, defined using appropriate ICD codes. Adjustment for potential confounding variables, including age, race, female gender, hypertension, diabetes, hyperlipidemia, heart failure, chronic kidney disease (CKD) stage 3 or greater, alcohol use disorder, and coronary artery disease, was conducted through multivariable logistic regression analysis.
Patients were categorized into two mutually exclusive groups: one with H. pylori and the other without. Demographic characteristics and in-hospital outcomes were analyzed for both groups. Mean values with 95% confidence intervals were used for continuous variables, while categorical variables were expressed as percentages of the total population. We utilized Healthcare Cost and Utilization Project (HCUP) weights and STATA's svy functions to estimate the national hospitalized US population from the observed hospitalization-level data. Differences between groups were assessed using t-tests and Chi-square tests for continuous and categorical variables, respectively, with a significance threshold of p<0.05.
The Elixhauser Comorbidity Index was computed using SAS version 9.4. Univariate logistic analysis was employed to examine the association between H. pylori and various outcomes, such as overall complication rates, in-hospital mortality, encephalopathy, gastrointestinal bleeding, spontaneous bacterial peritonitis, and hepatorenal syndrome, in comparison to patients without H. pylori. Subsequently, a multivariate logistic regression analysis was conducted for the same outcomes, adjusting for baseline factors that were significantly different (p<0.1) in baseline characteristics according to univariate analysis. The results of regression analyses were presented as odds ratios (OR) with corresponding confidence intervals (CI) and p-values. All statistical calculations were performed using STATA Version 14.2.
Results
Baseline characteristics
From the years 2016 to 2019, 416,410 patients had a primary discharge diagnosis of cirrhosis (Table 1). Of those patients, 990 (0.2%) had a secondary diagnosis of H. pylori infection. Cirrhosis patients with H. pylori were younger on average (mean age 54.25 vs. 57.18 years, p=0.01) and more likely to be within ages 18-49 (33.84% vs 24.71%, P=0.01). H. pylori-infected patients were also more likely to identify as male (70.71% vs 63.11%, P<0.028), Hispanic race (36.4% vs. 18.6%, p< 0.1), and of Black race (20.2% vs. 8.1%, p< 0.1). H. pylori patients were additionally more likely in the bottom quartile of median household income (48.17% vs. 34.66%, p< 0.01). The Elixhauser Comorbidity Index for mortality was similar in H. pylori and non-H. pylori patients (-1.77 vs -1.86, P=0.809).
Primary outcomes
H. pylori-exposed patients had lower in-hospital mortality (0.51% vs 4.44%, p=0.007) (Table 2). The mean length of stay, however, was higher in the H. pylori group (6.97 days vs 5.75, p=0.002). The overall cost of care was similar between the H. pylori exposed and non-exposed groups (mean USD18,106.18 vs $16,543.49, P=0.160).
Complications of cirrhosis
Patients exposed to H. pylori exhibited a higher overall incidence of complications related to cirrhosis (84.8% vs. 67.5%, p < 0.001), gastrointestinal bleeding (48.4% vs. 27.3%, p < 0.001), and hepatorenal syndrome (70.7% vs. 46.9%, p < 0.001), and these differences persisted even after adjusting for multiple variables in the analysis (refer to Table 3). Initially, rates of hepatic encephalopathy were higher in patients not exposed to H. pylori (21.5% vs. 15.6%, p <0.04), but this was rectified after accounting for potential confounding factors in the multivariate analysis, including age, race, sex, hypertension, diabetes mellitus, hyperlipidemia, heart failure, chronic kidney disease stage 3 or greater, alcohol use disorder, and coronary artery disease (Figure 1).
Adjusted outcomes for potential confounders using multivariable logistic regression analysisOdds of complication in cirrhosis patients with H. pylori infection compared to those without infectionSBP: spontaneous bacterial peritonitis
Discussion
H. pylori is a significant cause of morbidity and mortality, given its high prevalence worldwide. It was first discovered and identified as a cause of peptic ulcer disease in 1982 by Dr. Warren and Professor Marshall [6]. Its ability to colonize the stomach and cause gastrointestinal pathology is derived through four key steps: urease production, which confers acid neutralization within the stomach, flagella-mediated motility, cellular attachment through adhesins, and toxin production (e.g., CagA, VacA) causing tissue damage. CagA is also considered a major oncogenic factor in the development of gastric cancer. H. pylori has been classified as a group I carcinogen by the WHO since 1994 and is the etiologic factor in approximately 75% of worldwide gastric cancers and 5.5% of total malignancies [6-7].
H. pylori may be an independent contributor to liver damage through oxidative stress and hepatocyte injury [8]. This may fuel the development of decompensating events in cirrhosis. In particular, the association between hepatic encephalopathy and H. pylori has been of interest, given its ability to form ammonia. However, H. pylori eradication has not been consistently found to decrease ammonia levels and improve hepatic encephalopathy [9]. Other studies have shown an increased incidence of esophageal varices, gastric variceal bleeding, portal vein thrombosis, portal hypertensive gastropathy, and the development of hepatocellular carcinoma [10-13]. The findings of our multivariable analysis were significant for higher overall rates of gastrointestinal bleeding and hepatorenal syndrome in H. pylori-exposed patients.
There are multiple mechanisms by which H. pylori disturbs normal tissue. For example, it can release toxins directly into the cytoplasm or increase IL-8 and hydrogen peroxide in epithelial cells. It has been hypothesized that H. pylori can cause an overall state of severe endothelial dysfunction, including the portal venous system. This would lead to increased stiffness of the portal vein, increased portal pressure, and contribute to the formation of portal hypertension [14]. Portal hypertensive gastropathy results from intramucosal hemorrhage caused by portal hypertension and is characterized endoscopically by a mosaic-like pattern that may clinically manifest as acute or chronic gastrointestinal bleeding. This chronic inflammatory state formed by H. pylori can directly and indirectly further impair hepatocytes, exacerbating portal hypertensive gastropathy and increasing the risk of inflammatory lesions within the stomach in cirrhotic patients [10]. In addition, the overproduction of these pro-inflammatory cytokines can worsen portal hypertension and negatively affect varices. The current literature supports a significant association between H. pylori infection and gastrointestinal bleeding in both non-variceal and variceal bleeding forms [11]. A study by Devrajani et al., focusing on H. pylori infection in cirrhotic patients with upper gastrointestinal bleeding, demonstrated a 56% infection rate in these patients [15]. Another prospective study conducted by Elsebaey et al. demonstrated a significantly higher prevalence of H. pylori infection in cirrhotic patients with variceal bleeding than those without. It has been proposed that hypergastrinemia induces a hyperacidic state that is detrimental to the gastric mucosa causing erosions, ulcerations, and eventual variceal rupture and bleeding in cirrhotic patients [11]. The results of the current study showed higher rates of complications from gastrointestinal bleeding in H. pylori-infected patients compared with those without infection, which is consistent with the current literature.
In the present study, the rate of hepatic encephalopathy was initially higher in non-infected patients; however, this was corrected after multivariable analysis. Hepatic encephalopathy is a frequent complication of cirrhosis, with its pathogenesis thought to be driven by hyperammonemia. Therefore, many therapeutic approaches aim to target ammonia, such as targeting glutamine metabolism in the small bowel or bacterial ammonia production in the large bowel. However, the stomach can be another source of ammonia if H. pylori is present. As noted previously, H. pylori has the ability to form ammonia due to its urease activity, causing serum ammonia levels to increase at an even higher rate in cirrhotic patients and potentially accelerate hepatic encephalopathy [16]. Chen et al. conducted a prospective study that found hepatic encephalopathy was more frequently observed in cirrhotic patients infected with H. pylori. It also noted reduced levels of blood ammonia as well as significantly lower rates of hepatic encephalopathy after H. pylori eradication. On the other hand, other published literature on this association suggests that the ammonia levels produced by H. pylori are likely clinically insignificant in most cirrhotic patients. Despite multiple observational and interventional studies, it is still unclear whether clinicians should look for and treat H. pylori infection in all cirrhotic patients with hepatic encephalopathy [16-17].
Through multivariable analysis, this study found higher rates of hepatorenal syndrome in cirrhotic patients with H. pylori. H. pylori infection induces the release of multiple inflammatory cytokines and vascular active substances, such as C-reactive protein (CRP), tumor necrosis factor-alpha (TNF-α), interleukin 1 (IL-1), interleukin 6 (IL-6), interleukin 8 (IL-8), heat shock protein (HSP) causing local and systemic reactions [18]. Through risk factors of renal endovascular damage, proteinuria, and mesangial proliferation, H. pylori-exposed patients have accelerated loss of kidney function [18]. The development of renal failure in cirrhotic patients is known as hepatorenal syndrome, characterized by marked renal vasoconstriction with peripheral arterial vasodilation. A precipitating event, such as gastrointestinal bleeding, can place cirrhotic patients at a higher risk of developing hepatorenal syndrome [19]. As presented earlier, H. pylori-infected cirrhotic patients have been shown to have higher rates of gastrointestinal bleeding versus those without infection. In addition, a single-center observational study researching H. pylori infection as an initiating factor of complications in cirrhotic patients found an increased incidence of hepatorenal syndrome in H. pylori-positive versus negative patients [13]. The literature on the association between H. pylori and hepatorenal syndrome is limited. More studies will need to be conducted to understand the pathophysiology and determine whether this truly represents the general population.
Conclusions
This retrospective analysis has inherent limitations, and it is essential to acknowledge them. While the patients identified in the study were diagnosed with both H. pylori and cirrhosis upon discharge, it cannot be definitively concluded that H. pylori directly caused the complications associated with cirrhosis. Recognizing this uncertainty, further research is needed to better understand the connections between cirrhosis and complications related to H. pylori. Investigating the origins of cirrhosis and its relationship with H. pylori could offer valuable insights into whether the presence of H. pylori is a causative factor or merely a correlated aspect in patients with cirrhosis. Additionally, a prospective study focusing on eradicative therapy for H. pylori might prove beneficial in specific cases of cirrhosis, helping to determine whether such treatment can reduce the incidence of complications associated with cirrhosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The prevalence of Helicobacter pylori infection in different countries Aliment Pharmacol Ther Pounder RE Ng D 333921995 https://europepmc.org/article/med/85475268547526 · pubmed ↗
- 2ACG clinical guideline: Treatment of Helicobacter pylori infection Am J Gastroenterol Chey WD Leontiadis GI Howden CW Moss SF 21223911220172807165910.1038/ajg.2016.563 · doi ↗ · pubmed ↗
- 3Helicobacter pylori promotes colorectal carcinogenesis by deregulating intestinal immunity and inducing a mucus-degrading microbiota signature Gut Ralser A Dietl A Jarosch S 125812707220233701575410.1136/gutjnl-2022-328075 · doi ↗ · pubmed ↗
- 4Extraintestinal manifestations of Helicobacter pylori: A concise review World J Gastroenterol Wong F Rayner-Hartley E Byrne MF 11950119612020142523223010.3748/wjg.v 20.i 34.11950 PMC 4161781 · doi ↗ · pubmed ↗
- 5Association between cirrhosis and Helicobacter pylori infection: A meta-analysis Eur J Gastroenterol Hepatol Feng H Zhou X Zhang G 130913192620142530425110.1097/MEG.0000000000000220 · doi ↗ · pubmed ↗
- 6Clinical relevance of Helicobacter pylori infection J Clin Med Mladenova I 34731020213444176910.3390/jcm 10163473 PMC 8396975 · doi ↗ · pubmed ↗
- 7Helicobacter pylori infection: An overview of bacterial virulence factors and pathogenesis Biomed J Kao CY Sheu BS Wu JJ 14233920162710559510.1016/j.bj.2015.06.002PMC 6138426 · doi ↗ · pubmed ↗
- 8From the stomach to other organs: Helicobacter pylori and the liver World J Hepatol Waluga M Kukla M Żorniak M Bacik A Kotulski R 21362146720152632802510.4254/wjh.v 7.i 18.2136 PMC 4550868 · doi ↗ · pubmed ↗