The Impact of Constraint-Induced Movement Therapy on Motor Recovery in Middle Cerebral Artery Infarction Having Cardiomegaly in an Intensive Care Unit
Shweta A Nainani, Raghumahanti Raghuveer, Harsh R Nathani, Arasha F Khan

TL;DR
This case report explores how constraint-induced movement therapy helps a stroke patient recover motor function in an ICU setting.
Contribution
The study demonstrates the application of CIMT for motor recovery in stroke patients with cardiomegaly in an ICU.
Findings
CIMT was applied alongside conventional physiotherapy for a 65-year-old stroke patient.
The patient showed motor recovery improvements in the ICU setting.
CIMT is suggested as a beneficial rehabilitation approach for stroke patients.
Abstract
Stroke can be characterized by rapidly emerging neurological manifestations of global or focal impairment of neurological functionality, with consequences lasting a day or more or giving rise to mortality, with no significant etiology other than vascular origin. A middle cerebral artery (MCA) infarct is a form of stroke that develops when the MCA, one of the primary arteries providing blood to the brain, becomes blocked or obstructed. Constraint-induced movement therapy (CIMT) is an emerging method that has mainly been utilized to rehabilitate stroke patients, especially upper extremities. According to recent advances, CIMT can also be applied to the lower limbs to increase insufficient limb balance, thereby facilitating gait. This case report is based on a 65-year-old female who had weakness in the left side of the body and slurring of speech and was diagnosed with an MCA infarct. She…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
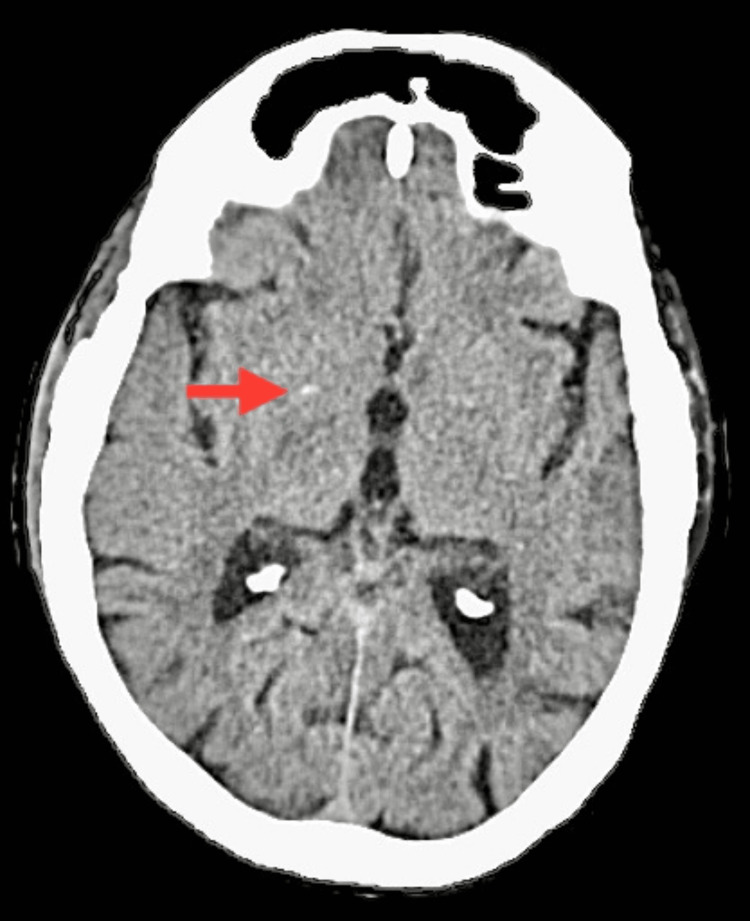 Figure 1
Figure 1 Figure 2
Figure 2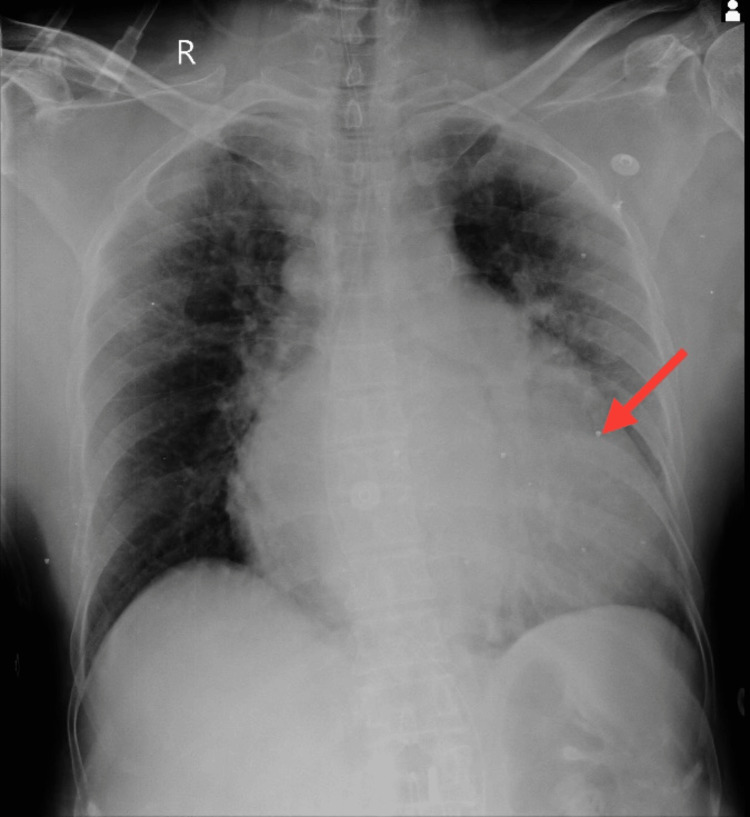 Figure 3
Figure 3 Figure 4
Figure 4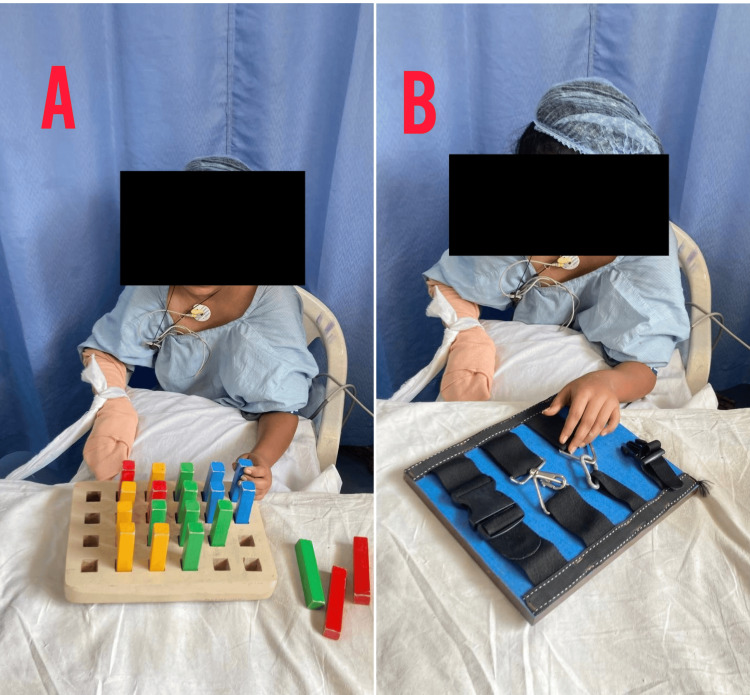 Figure 5
Figure 5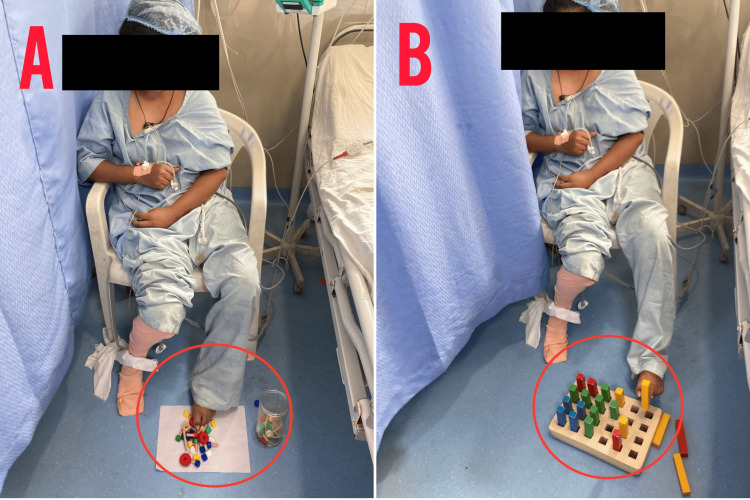 Figure 6
Figure 6| Phase | Goals | Interventions |
| Acute phase | Reduce edema and pain and prevent complications | Positioning to prevent contractures |
| PROM exercises | ||
| Bed mobility exercises | ||
| Breathing exercises | ||
| Limb elevation and effleurage | ||
| Subacute phase | Improve mobility and strength | AROM exercises |
| Bed-to-chair transfer practice | ||
| Gait training with assistance | ||
| Strengthening exercises for the left side | ||
| Recovery phase | Enhance functional independence | Progressive resistance exercises |
| Balance and coordination training | ||
| ADL training with adaptive techniques | ||
| Community reintegration activities |
| Week 1 | Week 2 | Week 3 |
| Grasping beads | Practice putting beads into a box | Putting beads into a rope |
| Holding a squeeze ball for five minutes | Holding a bottle for five minutes | Holding a chair |
| Turning the pages of a notebook in a forward direction | Turning the pages of a newspaper in a forward direction | Turning the pages forward and backward alternatively |
| Transferring cotton balls from one bowl to another | Transferring cotton balls with the help of a tweezer | Transferring water directly from one glass to another |
| Grasping a needle | Making holes in a putty with a needle | Putting a needle into a piece of cloth |
| Opening and closing a drawer | Opening and closing a sliding door | Opening and closing a cupboard |
| Pegboard exercises | Continue pegboard exercises | Continue pegboard exercises |
| Putting a ball in a jar | Putting a key in a jar | Putting a button in a jar |
| Taking out clothes from a hanger | Hanging and taking out clothes from a hanger | Hanging, taking out, and wrapping clothes |
| Opening and closing zips in a horizontal or vertical direction | Opening and closing zips in a zigzag manner | Opening and closing zips in a straight and zigzag pattern, alternatively |
| Spreading butter on bread | Spreading cream on a cake | Painting a wall |
| Opening the cap of a jar | Opening the cap of a bottle | Sharpening a pencil |
| Week 1 | Week 2 | Week 3 |
| Carrying beads with toes | Carrying a glass with toes | Pushing the wall |
| Spot marching with the affected leg | Walking with the affected leg and crossing obstacles | Walking backward with the affected leg and crossing obstacles |
| Walking straight | Walking in a zigzag pattern | Walking in a forward and zigzag pattern alternatively |
| Folding a handkerchief | Folding a T-shirt | Folding a saree |
| Putting a ball in a jar | Putting a key in a jar | Putting a button in a jar |
| Drawing a line with great toe | Drawing a semicircle | Drawing a circle |
| Pegboard exercises | Pegboard exercises | Pegboard exercises |
| Outcome measures | Pre-rehabilitation | Post-rehabilitation |
| STREAM | 17/70 | 30/70 |
| DGI | Jul-24 | Dec-24 |
| FIM | 131/210 | 180/210 |
| BBS | May-56 | 21/56 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Botulinum Toxin and Related Neurological Disorders · Cerebral Palsy and Movement Disorders
Introduction
Strokes are the world’s second-ranked significant factor for death and the third-ranked significant form of disability [1]. A stroke is described by the WHO as a suddenly evolving cerebral presentation of a worldwide or local impairment of function in the brain, with repercussions lasting longer than 24 hours or leading to mortality, with no significant etiology beyond its vascular origin [2]. Strokes are divided into two types: ischemic (80-87%) and hemorrhagic (13-20%). Ischemic strokes are the result of thrombus, embolism, or widespread hypoperfusion [3]. Cerebrovascular accident is an epidemic issue that is the leading parameter of disability in people [4]. According to the most recent data, 16.9 million individuals experience a cerebrovascular accident each year, with a worldwide incidence of 258 per 100,000 people per year, considerable discrepancies between high- and low-income countries, and an age-adjusted epidemiology 1.5 times higher in men than in women [5]. The epidemiology of cerebrovascular accidents in low- and middle-income nations has more than quadrupled during the last four decades [6].
Ischemic strokes are categorized into three types: anterior cerebral artery, middle cerebral artery (MCA), and posterior cerebral artery. MCA infarcts are the most common and impact motor activity due to their involvement in the corticospinal tract [7]. When blood flow from the MCA, one of the major arteries in the brain, is unexpectedly halted (ischemia) or completely stopped (infarction), a stroke ensues [8]. MCA infarctions can induce symptoms such as rapid-onset paralysis or numbness on one side of the body; typically, the face, arm, or leg are impacted [9]. These symptoms can also cause linguistic difficulties, including difficulty speaking. Patients may also experience visual problems, such as hemianopia. Cognitive skills may be affected, resulting in disorientation or confusion [10]. Aging, ethnicity, racial or ethnic background, and ancestry are all irreversible predisposing parameters for stroke [11]. Among other infectious agents, bacterial pathogens are the most prevalent cause of stroke [12]. Flexible stroke risk factors include elevated blood pressure, atrial fibrillation, various cardiac problems, hyperlipidemia, diabetes, smoking, lack of exercise, carotid stenosis, and transient ischemic attack [13].
Constraint-induced movement therapy (CIMT) was invented to address upper extremity limitations following a cerebrovascular accident and is a widely researched strategy for patient physiotherapy. However, recent advances suggest that CIMT also applies to the lower limbs for balance and gait. The original CIMT comprises non-paralyzed arm constraints and task-specific training. Modified types also use non-paralyzed arm restricting, although not as intensely as the primary CIMT. Both original and adapted CIMT positively affected motor activity, arm-hand functions, and self-experienced arm-hand activities in daily life [14]. It is anticipated that individuals who can benefit significantly from CIMT account for at least 50% of the overall stroke population [15]. Although meant to improve upper arm function, numerous authors have found that it improves balance [16]. CIMT, a stroke rehabilitation strategy, necessitates rigorous training of the damaged arm while restricting the mobility of the unaffected arm for six hours daily, five days a week, for two weeks [17]. The technique uses behavioral psychology, motor learning, and skill development concepts [18].
Case presentation
Patient information
The patient was a 65-year-old female who was brought to the neuro-outpatient department for complaints of weakness in the left side of the body and slurring of speech. She experienced these complaints for one day. She reported similar complaints six months ago and thereby visited the local hospital, where she was treated with medications. After a month, she experienced weakness on the left side of her body and was again treated with medications. She was admitted to the neurology ward, where specific investigations were done, such as an ECG, a two-dimensional echocardiogram, a color Doppler, an MRI, a complete blood count, a CT scan, and a chest X-ray. The patient had a known case of rheumatic heart disease, mild mitral stenosis, and mitral regurgitation; had a history of bronchial asthma and hypertension for three years; and was on medication for the same. The patient had no history of giddiness or falls. Moreover, there is no record of a head injury, fever, seizures, loss of consciousness, or headache in her medical history. She was then shifted to the medicine intensive care unit (MICU) for four days, then moved to the ward and treated with medications given, including a tablet of Clopitab-A 150 mg, a tablet of Rosuvas 40 mg, and an injection of Optineuron intravenous.
Clinical findings
The patient was endomorphic and had normal vital signs. Notably, both the upper and lower limbs exhibited dry and scaly skin. Notable clinical findings suggested an altered mental state, as the patient was conscious but not oriented to her surroundings. Additionally, the presence of slurred speech raised concerns about potential neurological involvement. The Glasgow Coma Scale score was 13 (E4V4M5), indicating a moderate level of consciousness. Furthermore, the assessment of cardiac function revealed a low ejection fraction, emphasizing the need for a thorough investigation into the neurological and cardiovascular aspects of the patient’s condition. Color Doppler imaging indicated atherosclerotic changes in the bilateral common carotid and internal and external carotid arteries. MRI findings showed altered signal intensity in the right corona radiata, lentiform nucleus, and temporal region, along with age-related atrophy and small vessel ischemic disease on the left side. A CT scan of the brain revealed a lesion in the right corona radiata, as shown in Figure 1, and chronic lacunar infarcts in the left gangliocapsular regions, as shown in Figure 2. Chest X-ray supine revealed cardiomegaly, as shown in Figure 3. Neurological assessments showed exaggerated biceps jerk, absent knee jerk, and extensor plantar response on the left side, while reflexes were normal on the right. The tone was 2+ on the right side and 3+ on the left. The patient also exhibited Wernicke’s aphasia, adding to the complex clinical picture.
CT scan of the brainThe red arrow shows an infarct in the right corona radiata.
CT scan of the brainThe red circle indicates chronic lacunar infarcts in the left gangliocapsular regions.
Chest X-ray eliciting cardiomegalyThe red arrow shows cardiomegaly.
Therapeutic intervention
Along with conventional therapy, CIMT was planned for the patient, which encompasses restricting the non-paralyzed arm and using the paralyzed arm for task-oriented activities. Table 1 represents the conventional therapy given to the patient; Table 2 describes the CIMT given for the left upper limb; and Table 3 describes the CIMT given for the left lower limb. Figures 4, 5, 6 show the patient being rehabilitated.
CIMT for the left upper limb(A) Bead exercises. (B) The red circle indicates squeezing a ball.CIMT, constraint-induced movement therapy
CIMT progressive exercises for the left upper limb(A) Pegboard exercises. (B) Opening and closing of zips in a zigzag pattern.CIMT, constraint-induced movement therapy
CIMT for the left lower limb(A) The red circle indicates bead exercises. (B) The red circle indicates pegboard exercises.CIMT, constraint-induced movement therapy
Outcome measures
The outcomes of the intervention are shown in Table 4.
Discussion
In 1999, Miltner et al. conducted a clinical trial on CIMT in which the participants were 15 individuals. Nine people had a right-side stroke, and six had a left-side stroke; all were right-arm predominant prior to the stroke. The treatment consisted of two primary parameters using a resting hand splint for 90% duration. At the same time, the patient is awake for the whole span of 12 days for constriction of the movement of the non-impacted upper arm and training of the arm that was impacted through an action known as “shaping” for about seven hours per day on the eight weekdays during that time. Patients improved considerably from before to after therapy on a clinical motor examination and a test evaluating the extent of use of the diagnosed limb in day-to-day activities, with no regression in performance at the six-month follow-up [19]. In 2006, Wolf et al. conducted a randomized controlled trial in which respondents were allocated at random to CIMT, which involved using a hindering mitt on the less affected grasp while practicing and shaping behavior with the hemiplegic hand or conventional therapy, which included no post-rehabilitation treatment to pharmaceutical or physiotherapeutic interventions. Sex and pre-stroke dominance were used to stratify patients. Their findings showed that CIMT resulted in a statistically considerable and medically relevant increase in the quality of arm movements for people who had cerebrovascular accidents during the preceding three to nine months and had it for at least a year [17].
Choi et al. arranged a randomized controlled experiment in 2017 to evaluate if game-based CIMT improves equilibrium skills in people with cerebrovascular accidents. Thirty-six chronic stroke victims were randomly assigned to one of the following three categories: game-based CIMT (n = 12), general game-based training (n = 12), and traditional (n = 12). For four weeks, all techniques were carried out three times a week. The static balance control and weight-bearing symmetry were examined, as well as the Functional Reach Test (FRT), modified FRT, and Timed Up and Go Tests, to assess balancing abilities. According to the findings, while conventional game-based retraining and game-based CIMT enhanced static and dynamic equilibrium skills, game-based CIMT improved static equilibrium control, weight-bearing symmetry, and side-to-side weight shift to a greater extent [16]. Duarte Pereira et al. conducted a multiple case study in 2022, including a convenience sample of 12 participants (eight males) with an average age of 55 years old. The lower extremity CIMT (LE-CIMT) intervention process, combining task-oriented training, motor learning techniques, and a transfer package, was conducted in a clinical environment. CIMT increased gait metrics, reduced test execution time, and enhanced functional mobility in stroke patients, according to the findings. The study indicated that LE-CIMT is a valuable management strategy for increasing perceptions of improvements and encouraging paralyzed lower extremities in daily mobility tasks [20].
Conclusions
According to studies, CIMT is the use of the paretic limbs by restricting non-paretic limbs and is mainly used for the upper limbs. Still, recent advances have proved that the therapy can be applicable for lower limbs to maintain balance and facilitate gait. Patients with stroke usually have difficulty performing activities of daily living due to weakness in their paretic limbs; hence, the therapy, which encompasses the use of paretic limbs, was found to be effective. Moreover, the subjective satisfactory experience with the CIMT provides valuable insights into the efficiency of this therapy in patients undergoing cerebrovascular accidents. The promising outcome measures have proved that CIMT in the ICU is a precise and versatile therapy for patients with stroke. Hence, we conclude that CIMT, in addition to primary rehabilitation, has been proven to be a promising approach for the rehabilitation of patients with stroke.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stroke: a global response is needed Bull World Health Organ Johnson W Onuma O Owolabi M Sachdev S 6349420162770846410.2471/BLT.16.181636 PMC 5034645 · doi ↗ · pubmed ↗
- 2The neuropsychiatry of stroke Psychosoma Chemerinski E Robinson RG 51441200010.1016/S 0033-3182(00)71168-610665263 · doi ↗ · pubmed ↗
- 3Stroke: current concepts S D Med Albertson M Sharma J 455465455, 457-61, 463-5672014 https://pubmed.ncbi.nlm.nih.gov/25490795/25490795 · pubmed ↗
- 4The global stroke initiative Lancet Neurol Bonita R Mendis S Truelsen T Bogousslavsky J Toole J Yatsu F 391393320041520779110.1016/S 1474-4422(04)00800-2 · doi ↗ · pubmed ↗
- 5Epidemiology of stroke and transient ischemic attacks: current knowledge and perspectives Rev Neurol (Paris) Béjot Y Daubail B Giroud M 596817220162671859210.1016/j.neurol.2015.07.013 · doi ↗ · pubmed ↗
- 6Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010 Lancet Feigin VL Forouzanfar MH Krishnamurthi R 24525438320142444994410.1016/s 0140-6736(13)61953-4PMC 4181600 · doi ↗ · pubmed ↗
- 7Motor recovery mechanisms in patients with middle cerebral artery infarct: a mini-review Eur Neurol Jang SH 2342396820122300657810.1159/000342026 · doi ↗ · pubmed ↗
- 8Malignant MCA infarction: pathophysiology and imaging for early diagnosis and management decisions Cerebrovasc Dis Heiss WD 1741201610.1159/00044162726581023 · doi ↗ · pubmed ↗