Right Femoral Fragility Fracture in an Adolescent with Vitamin D Deficiency from COVID-19 Pandemic-Related Confinement
Suhasheni Rajendran, Ze Chen Lee, Chu Ee Seow, Chong Hui Khaw

TL;DR
A 14-year-old boy suffered a femoral fracture due to vitamin D deficiency and a sedentary lifestyle during the pandemic.
Contribution
This case highlights the link between pandemic-related confinement, vitamin D deficiency, and fragility fractures in adolescents.
Findings
The patient had a low BMI and significant muscle loss due to prolonged inactivity.
DXA scans revealed low bone density with Z-scores of -2.2 (spine) and -3.9 (hip).
Vitamin D supplementation and rehabilitation led to improved physical fitness and normalized vitamin D levels.
Abstract
The COVID-19 pandemic has caused major impacts in various aspects of our life. In Malaysia, a Movement Control Order was imposed in March 2020. For almost two years, school going children and adolescents were not able to attend school physically, and their physical activity was confined within their room or house on most days. Case Description. We describe a case of a 14-year-old boy who was previously active in sports and sustained a low trauma fracture at the right neck of the femur following a prolonged period of extreme sedentary life along with poor dietary intake during the COVID-19 pandemic period. He underwent open reduction and screw fixation for the right neck femur fracture. He was thin with a low BMI (15.62 kg/m2) and a significant loss of muscle bulk in all limbs. Laboratory tests showed vitamin D deficiency (15.3 nmol/L) and the dual energy X-ray absorptiometry (DXA)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
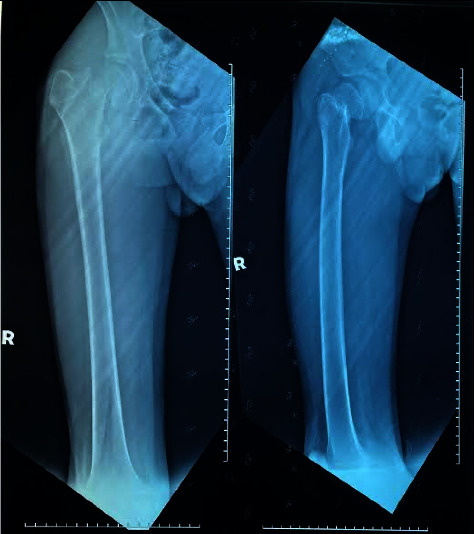 Figure 1
Figure 1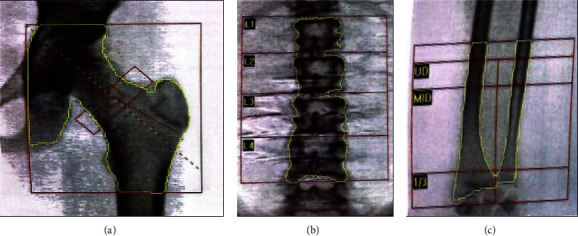 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin D Research Studies · Vitamin C and Antioxidants Research · Bone health and osteoporosis research
1. Introduction
Cutaneous synthesis from natural sun exposure is the primary source of vitamin D. Vitamin D deficiency reduces bone mass and increases the risk of osteoporotic fracture [1]. Movement Control Order (MCO) was commenced in Malaysia in March 2020 to combat the endemic spread of coronavirus disease 2019 (COVID-19). Lifestyle changes and dietary modifications during the COVID-19 lockdown were linked to overweight, nutritional deficiencies, reduced outdoor activity, and sun exposure.
2. Case Presentation
A 14-year-old boy with no prior medical history presented in October 2021 with a right femoral neck fracture (Figure 1) after slipping and falling from a standing position. He had no family history of bone or neuromuscular disease. He was active in outdoor cycling and soccer before the start of the Movement Control Order (MCO), but during the COVID-19 lockdown, he spent most of his time playing online games in a windowless room, limiting his sun exposure. His addiction to the mobile game led him to neglect his diet. Most of his meals during MCO comprised of fast food ordered via food delivery service, lacking of desirable nutrients including calcium and vitamin D. These lifestyle changes contributed to muscle loss and weight loss, without other constitutional or gastrointestinal symptoms.
He was assessed 6 weeks after the event at a visiting endocrinologist clinic. At the initial encounter, he was underweight, with a height of 158 cm, a weight of 38 kg, and a body mass index (BMI) of 15.62 kg/m^2^. His body weight was 42 kg with a BMI of 16.82 kg/m^2^ before MCO. He had marked muscle wasting, especially over his right thigh and both hands, but no obvious bony deformity over the spine or other long bones. He underwent an open reduction and internal fixation of his right femoral neck fracture. Investigations were performed to further evaluate the low-impact fracture (Table 1).
A full blood picture showed normal erythrocyte morphology without evidence of blasts or abnormal lymphoid cell. Protein and red cells were absent in the urinary analysis. Antibodies for celiac disease were not sent, as he did not experience any gastrointestinal symptoms. He had severe vitamin D deficiency and significantly reduced bone mineral density (BMD) on dual-energy X-ray absorptiometry (DXA) (Figure 2), with low Z-scores at the lumbar spine (−2.2) and left hip (−3.9) as shown in Table 2. He was started on activated vitamin D alpha calcidiol 0.25 mcg and cholecalciferol 5000 IU daily.
After surgery, he was followed up in endocrine and sports medicine clinics. He underwent physiotherapy and was advised to increase his intake of dietary vitamin D and get adequate daily sun exposure. Four months later, his total vitamin D level had increased from 15.3 nmol/L to 62.15 nmol/L, and his DXA scan showed a marked improvement in Z-score (Table 2). Additionally, he showed a marked improvement in physical fitness, being able to jog and cycle during his recent endocrine clinic review, in contrast to a few months prior, when he had required crutches and a wheelchair for ambulation.
3. Discussion
Despite living in an equatorial climate with year-round sunshine, 30–50% of children and adolescents in Malaysia have vitamin D deficiency or insufficiency [2]. We report an unusual case of a low-energy right femoral fracture due to vitamin D deficiency in a 14-year-old boy with a sedentary lifestyle and reduced outdoor activity and sunlight exposure during the COVID-19 lockdown. Notably, lower vitamin D concentrations were also observed among children in China and Poland during the COVID-19 confinement period [3]. Other diseases associated with low bone mineral density were excluded through a thorough history and physical examination, as well as blood tests for neuromuscular disorders (e.g., Duchenne muscular dystrophy, myopathies), hematological diseases (e.g., leukemia, thalassemia), systemic autoimmune diseases (e.g., juvenile systemic lupus erythematosus, dermatomyositis, systemic sclerosis), gastrointestinal diseases (e.g., inflammatory bowel disease, celiac disease), renal disease (e.g., nephrotic syndrome, chronic kidney disease), and endocrine diseases (e.g., hypogonadism, hyperthyroidism, hyperparathyroidism, adrenal insufficiency, growth hormone deficiency). Muscle wasting noticed over hands and right thigh is most probably related to disuse atrophy, as physical examination did not detect other signs suggestive of neuromuscular disorders.
Unlike most adolescent fracture cases, which involve the humerus and distal forearm, our patient sustained a low-impact right femoral fracture after a fall from a standing position. This triggered the orthopedic team to refer him to rule out other possible causes of fragility fracture. His serum 25-hydroxyvitamin D level was critically low at 15.3 nmol/L (less than 30 nmol/L). His DXA scan showed a low Z-score at the lumbar spine and left hip. Ideally, bone mineral content should be measured over the lumbar spine and total body less head (TBLH) in adolescents to diagnose osteoporosis [4]. Clinical presentation in this case did not meet the criteria to define osteoporosis in adolescents, which require a BMD Z-score of ≤ −2.0 coupled with a clinically significant fracture history, including two or more long bone fractures by the age of 10 years, three or more long bone fractures at any age up to 19 years, or vertebral compression fractures [4]. Osteoporosis diagnosis criteria that require both a Z-score and a recurrent fracture may underdiagnose the condition, as patients may need to be monitored for a second or third fracture before diagnosis. Therefore, current recommendations advise considering clinical context in the diagnosis of osteoporosis, specifically the severity and prognosis of the underlying disease or treatment [5]. Lack of compensatory raise parathyroid hormone (PTH) level in this case is probable explained by hypomagnesemia and a decreased inhibitory threshold of PTH [6]. Alkaline phosphatase levels did not increase, as in most of the severe vitamin D deficiency cases. To date, studies on the relationships of alkaline phosphatase with serum vitamin D levels have shown variable results [6]. Hypophosphatasia carrier state could be an alternative explanation for his normal alkaline phosphatase, but urine phosphate levels and genetic testing were not performed [7].
The patient was started on activated vitamin D alpha calcidiol 0.25 mcg and cholecalciferol 5000 IU daily for 6 months duration, as per guidelines [6]. Multimodal management with the involvement of an orthopedic surgeon, endocrinologist, sports physician, and physiotherapist is crucial for subsequent management and rehabilitation. The patient showed marked gains in muscle bulks, improvements in physical fitness, serum vitamin D levels, and bone mineral density at succeeding follow-up sessions. The repeated calcium and phosphorus level subsequently were 2.42 mmol/L and 1.58 mmol/L, respectively. DXA will be repeated after one year and then every 1 to 2 years thereafter, depending on the patient's progression. The patient was also given dietary advice on a balanced diet that meets calcium and vitamin D requirements and was recommended to get adequate exposure to sunlight (at least six minutes per day) for optimal cutaneous synthesis of vitamin D [4, 8].
4. Conclusion
A high degree of suspicion is needed to rule out secondary causes in adolescents who present with unusual fragility fractures. Inadequate vitamin D bioavailability and physical activity reduce bone acquisition and peak bone mass, increasing the risk of low-impact fractures in teenagers. Early detection and intervention with sufficient calcium and vitamin D intake, adequate sunlight exposure, and maximized physical activity are paramount for maintaining bone health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dominguez L. J. Farruggia M. Veronese N. Barbagallo M. Vitamin D sources, metabolism, and deficiency: available compounds and guidelines for its treatment Metabolites 2021114 p. 25510.3390/metabo 11040255 PMC 807458733924215 · doi ↗ · pubmed ↗
- 2Chee W. S. S. Chang C. Y. Arasu K. Vitamin D status is associated with modifiable lifestyle factors in pre-adolescent children living in urban kuala lumpur, Malaysia Nutrients 2021137 p. 217510.3390/nu 13072175 PMC 830830134202743 · doi ↗ · pubmed ↗
- 3Tomaszewska A. Rustecka A. Lipińska-Opałka A. The role of vitamin D in COVID-19 and the impact of pandemic restrictions on vitamin D blood content Frontiers in Pharmacology 20221310.3389/fphar.2022.836738 PMC 889972235264968 · doi ↗ · pubmed ↗
- 4Galindo-Zavala R. Bou-Torrent R. Magallares-López B. Expert panel consensus recommendations for diagnosis and treatment of secondary osteoporosis in children Pediatric Rheumatology 2020181 p. 2010.1186/s 12969-020-0411-9PMC 704111832093703 · doi ↗ · pubmed ↗
- 5Ciancia S.. van Rijn R. R. Högler W.. Osteoporosis in children and adolescents: when to suspect and how to diagnose it European Journal of Pediatrics 202218172549256110.1007/s 00431-022-04455-235384509 PMC 9192469 · doi ↗ · pubmed ↗
- 6Hashemipour S. Larijani B. Adibi H. The status of biochemical parameters in varying degrees of vitamin D deficiency Journal of Bone and Mineral Metabolism 200624321321810.1007/s 00774-005-0674-82-s 2.0-3364587769116622734 · doi ↗ · pubmed ↗
- 7Matsuo K. Mukai T. Furuya A. Suzuki S. Tanahashi Y. Azuma H. A case of vitamin D deficiency without elevation of serum alkaline phosphatase in a carrier of hypophosphatasia Clinical Pediatric Endocrinology 2013224737610.1297/cpe.22.732-s 2.0-8488664574724170964 PMC 3809733 · doi ↗ · pubmed ↗
- 8Munns C. F. Shaw N. Kiely M. Global consensus recommendations on prevention and management of nutritional rickets Journal of Clinical Endocrinology and Metabolism 2016101239441510.1210/jc.2015-21752-s 2.0-8495935719626745253 PMC 4880117 · doi ↗ · pubmed ↗