Spanish version of Multidimensional Mentalizing Questionnaire (MMQ): Translation, adaptation and psychometric properties in a Chilean population
Nerea Aldunate, Pablo López-Silva, Cristian Brotfeld, Ernesto Guerra, Edmundo Kronmüller, Juan Luis Castillo-Navarrete, Juan Luis Castillo-Navarrete, Juan Luis Castillo-Navarrete, Juan Luis Castillo-Navarrete

TL;DR
This study translates and adapts the Multidimensional Mentalizing Questionnaire into Spanish for use in Chile, showing it works well for measuring mentalization in this population.
Contribution
The first Spanish version of the MMQ, adapted and validated for a Chilean population, with improved psychometric properties.
Findings
The translated MMQ shows strong psychometric properties after item modifications based on confirmatory factor analysis.
Positive mentalizing correlates with empathy, especially cognitive empathy, while negative mentalizing links to poor perspective-taking and aggression.
Gender differences in mentalizing are observed, and negative mentalization decreases with age.
Abstract
This paper presents the first translation and adaptation of the Multidimensional Mentalizing Questionnaire (MMQ) into Spanish for a native Spanish-speaking sample in Chile. The study examines the psychometric properties and internal consistency of the translated MMQ. The instrument undergoes modifications based on a confirmatory factor analysis of the original structure, resulting in the elimination of items with cross-loadings and improvement in model fit. The modified scale is then analyzed, demonstrating strong psychometric properties. Convergent evidence is assessed by correlating MMQ subscales with the Interpersonal Reactivity Index (IRI) and Empathy Quotient (EQ), while divergent evidence is assessed by correlating aggressive traits using the Buss-Perry Aggression Questionnaire (BPAQ). The study also explores gender differences and age. Results reveal positive correlations between…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
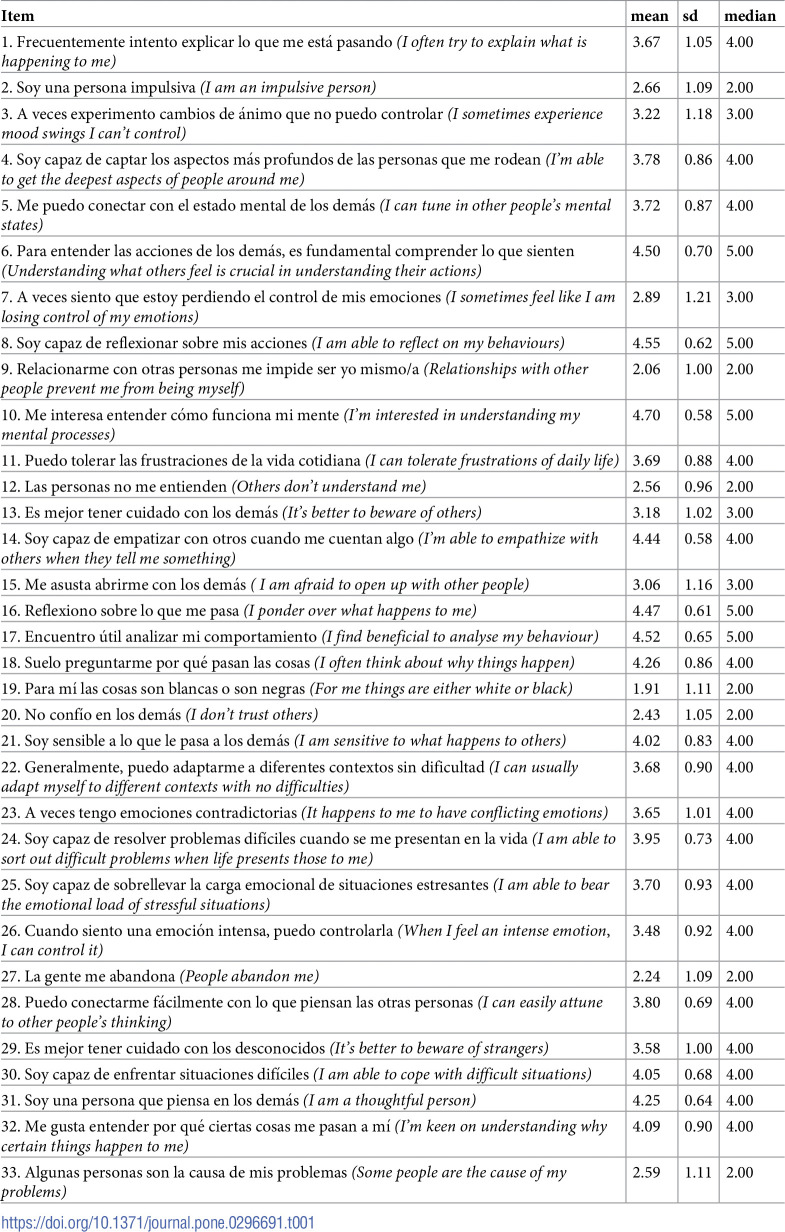 Figure 1
Figure 1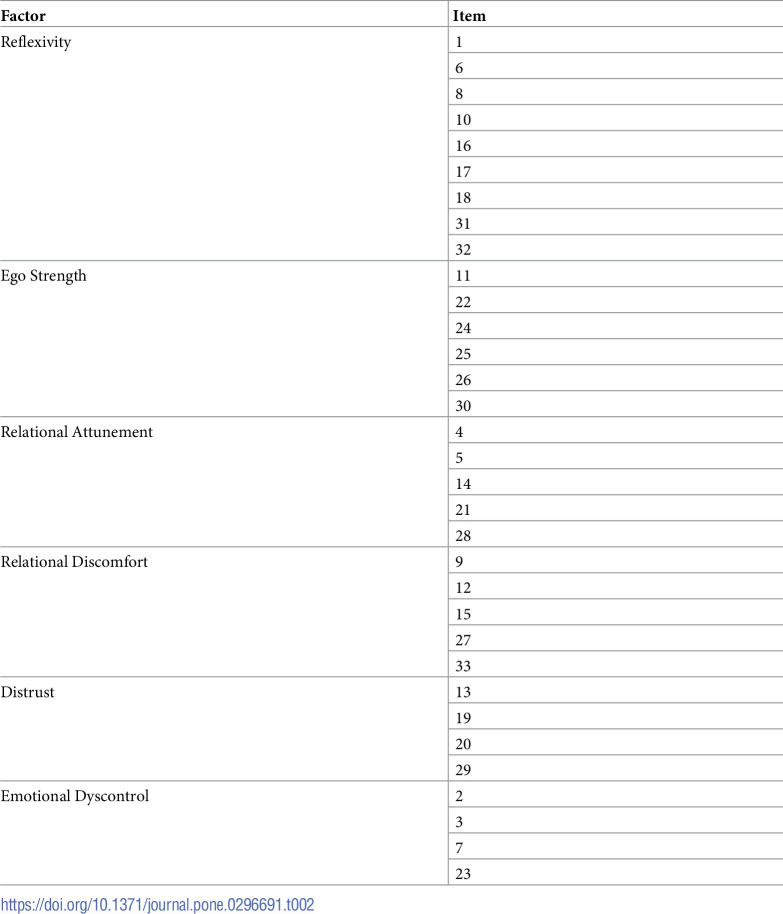 Figure 2
Figure 2 Figure 3
Figure 3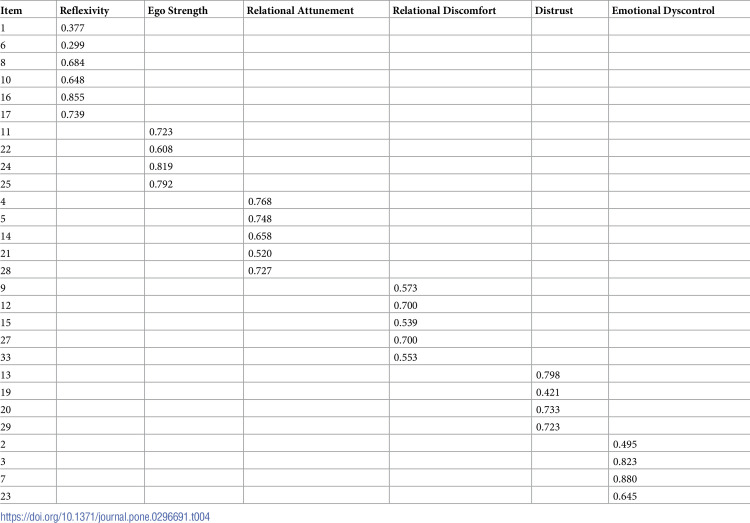 Figure 4
Figure 4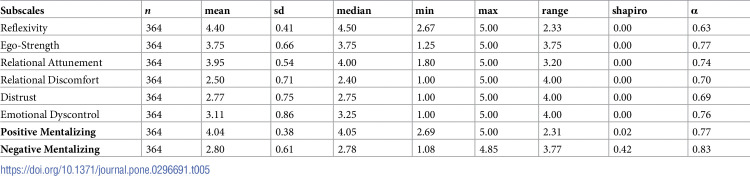 Figure 5
Figure 5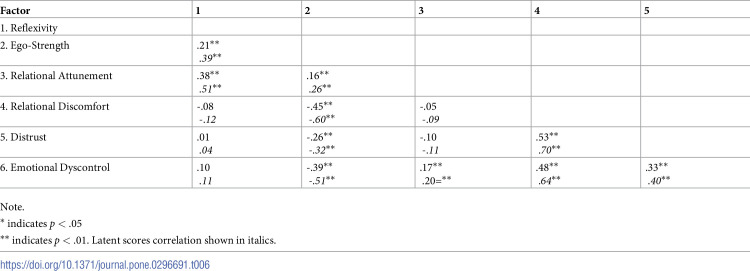 Figure 6
Figure 6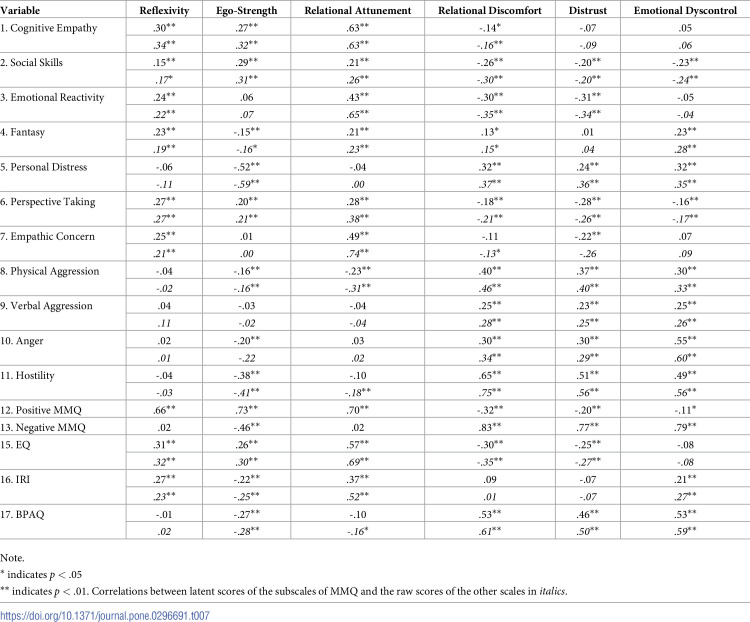 Figure 7
Figure 7 Figure 8
Figure 8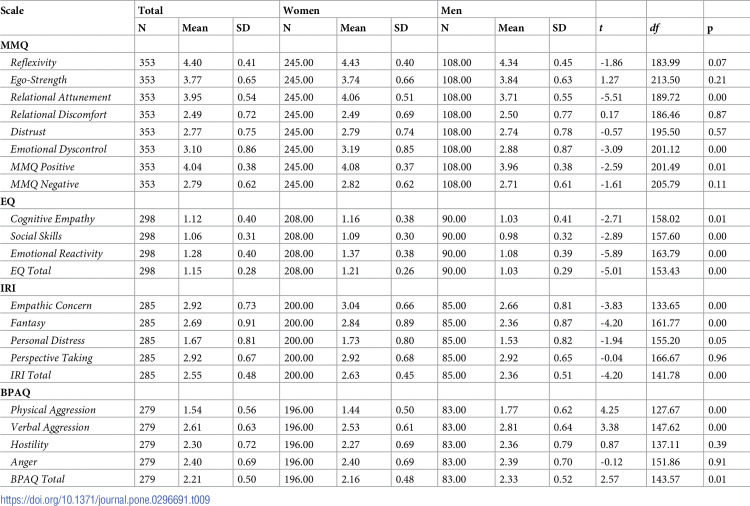 Figure 9
Figure 9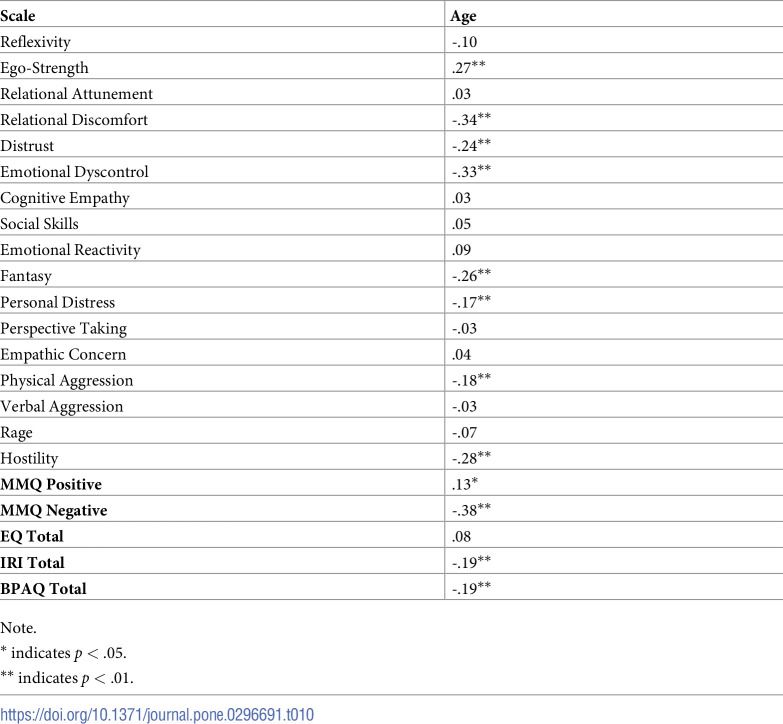 Figure 10
Figure 10- —http://dx.doi.org/10.13039/501100020884Agencia Nacional de Investigación y Desarrollo
- —http://dx.doi.org/10.13039/501100020884Agencia Nacional de Investigación y Desarrollo
- —http://dx.doi.org/10.13039/501100020884Agencia Nacional de Investigación y Desarrollo
- —http://dx.doi.org/10.13039/501100020884Agencia Nacional de Investigación y Desarrollo
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPersonality Disorders and Psychopathology · Personality Traits and Psychology · Attachment and Relationship Dynamics
Introduction
Mentalizing is the process of making sense of our own and others’ behavior in terms of subjective states and mental processes [1–3]. Mentalization belongs to a broader set of socio-cognitive abilities aiming at perceiving, interpreting, and processing social information in the environment, namely, social cognition. Through the generation and flexible use of mental representations about the relationship between oneself and others, mentalizing is crucial in guiding socially functional behavior [4–9]. Studied in the context of the attachment-based approach to trauma and resilience [10, among many others, 11], the capacity for mentalizing is thought to be internalized during the early stages of development through reciprocal behavioral patterns in the relationship between infants and their caregivers [12–14]. Consistently, it has been shown that different attachment patterns facilitate or hinder adult mentalization processes [3, 15, 16].
Mentalization has been linked to the development of several capacities that are relevant in everyday social interaction. Indeed, since it involves an active meaning-giving perspective-taking that allows the differentiation between one’s and the other’s behaviors, it plays an important role in the construction of a stable sense of self and the mutuality of the social relationships we build over time [14, 16]. Mentalization has been also positively linked to language skills, emotional control, and executive control over several cognitive abilities [17]. An important capacity that has been linked to mentalization is empathy. Mentalization involves the capacity to comprehend and infer others’ thoughts and emotions from different sources, including non-verbal signals such as gestures, facial expressions, and gaze, as well as knowledge about their perspectives and beliefs [18–20]. Evidence suggests that high-level mentalization skills that require the integration of knowledge about beliefs with knowledge about emotions are related to the ability to empathize with others [21]. Thus, mentalization is not only related to understanding the current individuals’ emotional states, but also to the prediction of their future emotional states as a consequence of their beliefs [22, 23].
Over the years, it has been shown that the capacity to mentalize plays an important role in mental health [2, 24, 25]. For example, it is thought to be a crucial factor in the relational difficulties and interpersonal stress characteristic of schizophrenia and antisocial and borderline personality disorders [26–28]. In this context, a distinction has been made between implicit mentalization, corresponding to automatic-not conscious-processing, and explicit mentalization, which requires conscious verbal effort [29, 30]. Research suggests that social stress in subjects with antisocial traits, personality disorders, and schizophrenia would predominantly activate implicit over explicit mentalizing [30, 31]. This abnormal pattern of activation in the mentalizing system would underlie difficulties in the general understanding of social situations prompting the type of impulsive and aggressive behaviors observed in some of these conditions [32, 33]. Consistent with these findings, previous research suggests that problems in mentalization underlie emotional dysregulation, commonly observed in the aforementioned conditions [34, 35].
The assessment of mentalization
Despite its clinical relevance as a promoter of mental health and its relation to several other cognitive and affective abilities, developing assessment methods for mentalization capacities (for others and oneself) has been elusive. Most of the methods currently available involve clinical interviews performed by trained professionals and direct observation of behaviors that could be labeled as instances of mentalizing [36]. This imposes several practical and methodological constraints on the assessment process, making it highly complex and time-consuming, especially, when applied to large samples [27]. To avoid some of these issues, researchers have started to use self-report-based methods focused on socio-affective abilities to assess mentalization in a reliable and straightforward way [2, 27, 37]. An example of this is the Empathy Quotient [EQ; 38], a 60-item questionnaire (with a 40-item shorter version) that focuses on assessing cognitive empathy, emotional reactivity, and social skills. However, besides cognitive empathy, this questionnaire does not offer valuable information about key non-affective elements of mentalization involving a higher representational component, such as, for example, beliefs about the other, expectations, and intentions.
Another example of self-report-based methods is the Interpersonal Reactivity Index [IRI; 39, 40], a 28-item survey focused on the assessment of empathy and answered on a 5-point Likert scale. The IRI has four subscales, each one with seven items. The first two subscales focus on the cognitive aspects of empathy. While perspective-taking refers to the tendency to adopt the psychological point of view of others spontaneously, fantasy captures subjects’ tendency to transport themselves imaginatively into the feelings and actions of fictitious characters in books, movies, and plays. The other two subscales focus on affective elements of empathy. While empathic concern assesses other-oriented feelings of sympathy and concern for unfortunate others, personal distress measures self-oriented feelings of personal anxiety and unease in tense interpersonal settings [40]. Problematically, the IRI’s focus on empathy does not allow for identification of the more fine-grained cognitive-representational components involved in the mentalization process. This becomes a practical problem when considering the fundamental role of these components in the currently dominant definitions of mentalization, as seen in the case of the EQ.
Recently, the Multidimensional Mentalizing Questionnaire [MMQ; 2] has been proposed to improve self-report-based methods by assessing mentalization in a less constrained way and, crucially, beyond its affective components. The MMQ assesses mentalization capacities in adults from an attachment theory framework [see 2, 41], and it is developed based on the Handbook of Mentalizing in Mental Health Practice [42]. The MMQ proposes an integrated and multilevel model of mentalizing. It consists of 33 items answered on a 5-point Likert scale, ranging from 1 ‘Not at all’ to 5 ‘A great deal’. It allows for the assessment of the levels of mentalization based on the construct conceptualization covering four axes: cognitive-affective, self-other, outside-inside, and implicit-explicit [see 41, Appendix A]. The factor model was tested through a confirmatory factor analysis (CFA) that indicated a 6-factors structure grouped in positive–or good mentalizing—(reflexivity, ego-strength, and relational attunement) and negative factors–or bad mentalizing—(relational discomfort, distrust, and emotional dyscontrol), with a satisfactory internal consistency (α = 0.75).
Regarding the positive factors that measure good mentalizing, reflexivity indicated a propensity towards self-mentalization through meta-cognition, introspection, and critical thinking (e.g., ‘I often try to explain what it is happening to me’, “Provo spresso a darmi delle spiegazioni su ciò che mi accade”, α = 0.89). Ego-strength concerns the perception of being able to face everyday problems with an emotional resistance to stress and frustrations (e.g., ‘I am able to cope with difficult situations’, “Sono in grado di affrontare situazioni difficili”, α = 0.81), and relational attunement indicated the ability to tune with the emotional and cognitive states of others to understand their experiences (e.g., ‘I can easily attune to other people’s thinking’, “Riesco a sintonizzarmi facilmente sul pensiero altrui”, α = 0.82). Regarding the negative factors, relational discomfort (opposite to relational attunement) captures a subject’s interpersonal difficulties and the perception of being misunderstood and damaged by others (e.g., ‘Others don’t understand me’, “Gli altri non mi capiscono”, α = 0.76). Distrust (opposite to ego-strength) refers to an attitude of closed-mindedness, distrust in relationships and a tendency to have a binary and rigid view of the world (e.g., ‘It’s better to beware of others’, “È meglio stare attenti agli altri”, α = 0.74). Finally, emotional dyscontrol (opposite to reflexivity) refers to the difficulty in managing own affective states and to a tendency to impulsiveness (e.g., ‘I am an impulsive person’, “Sono una persona impulsiva”, α = 0.72). Recently, the psychometric properties of the MMQ have been backed up by the use of network and factorial analysis supporting the usefulness of this self-report-based method and its application in both research and clinical practice [41].
The present study
There are more than 485 million native speakers of Spanish, making it the 3^rd^ most spoken language in the world [43]. However, no method for the specific assessment of mentalization capacities has been developed or adapted to the Spanish language, thus creating important epistemic and clinical asymmetries for developing research about psychological promoters of mental health in that community. Indeed, as mentioned above, mentalization is associated with mental health at the level of relational difficulties and interpersonal stress in schizophrenia and antisocial and borderline personality disorders. Moreover, suicidal behavior could also be linked to a low capacity for mentalization [44, 45]. Thus, early detection of low levels of mentalization could serve both prevention and management in therapeutic interventions such as Mentalization-Based Therapy [46–48]. In this regard, it has also been proposed that mentalization is one of the primary tools for establishing therapeutic settings that could lead to a good alliance between therapist and patient. Finally, the MMQ could also be applied to therapists in training, serving to identify shortcomings and recommend the development of mentalizing skills [47, 49, 50].
Although the EQ and IRI have Spanish versions, it is essential to recall that such scales focus on assessing empathy rather than mentalizing capacities. In addition, neither the EQ nor the IR provide clear identification of cognitive components involved in the mentalization process, such as beliefs about the other, expectations, and intentions, among many others. Considering this gap in the literature, the present study examines the psychometric properties and internal consistency of the first translation of the MMQ into the Spanish. The current data was obtained from a large sample of native Spanish speakers in Chile.
Additionally, the study will aim at testing the following two hypotheses: First, since both mentalizing and empathy involve understanding and interpreting the mental and emotional states of others to facilitate social cognition and mutual understanding, we expect them to be positively associated, especially in the scales measuring their cognitive component. Second, considering that difficulties in the general understanding of social situations can lead to misinterpretations of others’ intentions and behaviors, leading in turn to a higher propensity for aggression, we expect difficulties in mentalizing to be positively associated with engagement in aggressive behaviors. To tests these hypotheses, we correlated the MMQ with the Spanish versions of the EQ and IR, and the Chilean version of the Buss and Perry Aggression Questionnaire [BPAQ; 51], an instrument designed for the assessment of different aggressive behaviors. Thus, the study provides convergent and discriminant evidence of the validity of the MMQ.
Methods
Participants
419 adults participated in the study. 364 completed all the MMQ (M_age_ = 29.32, SD = 11.73) participated in the study. Female participants represented 67.3% of the sample, 29.7% were males, and 3% other gender or prefer not to say. Half of the participants had completed High School (50.8%) and the other half had a college degree or equivalent (49,2%). They participated in exchange of the participation in a raffle for three gift cards of 50.000 CLP. All participants gave informed consent approved by the ethical committee of the Pontificia Universidad Católica de Chile by checking the box corresponding to “I accept to participate” (in Spanish: Acepto Participar) in the web form. Data was collected from April 29^th^ to June 16^th^ of 2022.
Measures
The Empathy Quotient Scale (EQ)
The EQ was originally developed by Baron-Cohen and Wheelwright [38] to measure empathy and showed a good internal consistency (α = 0.92). The scale is comprised of 60 items, 40 of which are statements related to empathy, either affective or cognitive (e.g., ‘Other people tell me I am good at understanding how they are feeling and what they are thinking’), while the other 20 items are fillers (e.g., ‘I prefer animals to humans’). Participants must answer on a 4-point Likert scale, ranging from strongly agree (1) to strongly disagree (4). According to Lawrence, Shaw [52], the EQ has a 3-factor composition. The first obtained factor is Cognitive Empathy (CE), with items related to the capacity to attribute mental states, representing affective states (e.g., ‘I can tell if someone is masking their true emotion’), epistemic states (e.g., ‘I find it easy to put myself in somebody else’s shoes’) and desires (e.g., ‘I can easily work out what another person might want to talk about’). The second factor is Emotional Reactivity (ER) which measures the tendency to react emotionally in response to others’ mental states (e.g., ‘seeing people cry doesn’t really upset me’). Finally, the third factor is Cognitive Skills (CS), which asses the spontaneous use of empathic skills (e.g., ‘I often find it difficult to judge whether something is rude or polite’). The overall Cronbach’s alpha for the Chilean version was 0.83 [53], and in this study was 0.78.
The Interpersonal Reactivity Index (IRI)
The IRI measures empathy in four dimensions: emphatic concern, perspective-taking, personal distress, and fantasy. The original English version [39, 40] shows good internal consistency with Cronbach’s alphas ranging from 0.71 to 0.77. As defined by Davis [40], emphatic concern (EC) evaluates the tendency to sympathize with others who suffer (e.g., ‘I often have tender, concerned feelings for people less fortunate than me’). Perspective-taking (PT) refers to the tendency to take the psychological point of view of others (e.g., ‘I try to look at everybody’s side of a disagreement before I make a decision’). Fantasy (FT) assesses the capacity to imaginatively feel and think like fictional characters in movies and books (e.g., ‘I really get involved with the feelings of the characters in a novel’). Finally, Personal distress (PD) measures the level of anxiety produced by adverse scenarios (e.g., ‘I sometimes feel helpless when I am in the middle of a very emotional situation’). The instrument presents statements on a 5 points Likert scale, ranging from 1 (does not describe me well) to 5 (describes me very well). Its psychometric structure was tested in a Chilean sample [54], showing a consistent pattern with the original (α = 0.76). For the current study, the observed Cronbach’s alpha was 0,79.
Buss and Perry Aggression Questionnaire (BPAQ)
The original BPAQ [55] measures four forms of aggression through self-report, with statements such as ‘Sometimes I can’t control the impulse to hit another person’. Participants must indicate on a 5-point Likert scale, ranging from 1 (extremely uncharacteristic of me) to 5 (extremely characteristic of me). Its psychometric structure was tested with a sample of Chilean students [51], showing Cronbach’s alphas ranging from 0.60 to 0.80. The questionnaire shows a composition with four factors. Physical aggression and verbal aggression asses the activation of aggressive behaviors. Whereas hostility reflects the cognitive and anger the affective aspects of aggressive traits. In this study, BPAQ showed a good internal consistency (α = 0.88).
Items translation and adaptation
The process of translating and adapting the items focused on reducing irrelevant features of the construct by adapting them to the cultural characteristics of the target population [American Psychological 56]. For this reason, all items were translated in two ways: a literal translation and an adapted translation, aiming for the latter to address the expressive modes specific to Chilean cultural and linguistic context. Both translations and the original English items were presented to an expert panel composed of two psycholinguists and two linguists. The panel members analyzed and evaluated the translations following a process adapted from Solano-Flores, Contreras-Niño [57]. This process examined ten dimensions in which adaptation errors can occur during translation: style, format, conventions, information, grammar, semantics, register, culture, and origin (error in the original item). Items in which errors were detected were discussed until a consensus was reached regarding an error-free final version.
Five cognitive interviews (3 women) with individuals without formal education in psychology were conducted. The procedure consisted of two stages. In the first stage, participants completed the instrument, and in the second stage, they were interviewed for each item, answering four questions: 1) What is the item asking you to respond to? 2) What did you answer? 3) Why did you choose this response? 4) Was there anything in the item that seemed unclear or confusing to you? A total of 21 items with errors were identified and agreed upon, of which 19 were in the register dimension, 7 in the semantic area, and 1 in the information area. In all these cases, the errors were corrected, and a suitable version from the panel’s perspective was reached.
Data analyses
With the structure proposed and tested by Gori, Arcioni [2], we conducted a confirmatory factor analysis (CFA) of the adapted MMQ, based on the common factors model. In addition, we tested 3 additional models: bifactor, one-factor, and hierarchical factor model, to determine the best factor structure. We then test their reliability by computing Cronbach’s alpha for each subscale. In order to contrast our initial hypotheses, we compute Pearson correlations with all scales and subscales of the different instruments for convergent and divergent evidence. Finally, following Gori, Arcioni [2], we conducted a t-test on the means for males and females on each subscale for all the MMQ scales. To test whether the constructs have the same meaning for those who identify themselves as men or women, we performed an analysis of invariance. Following the sequence proposed by Wu & Estabrook [58], we first compared the baseline configural model with a restricted threshold model, then the factor loadings are restricted, and the intercept is forced to be equal across groups. Finally, the error variance for both groups is set to be equal. Given the ordinal nature of the Likert scale used in the instrument, we used polychoric correlations to estimate the model’s fit. This methodological approach has been widely argued to be the most suitable for modeling ordinal data [59–61]. All analyses were conducted with R Lavaan [v0.6.15; 62].
Results
Descriptive analyses
Table 1 presents each item along with its respective mean, median, and standard deviation. The original factorial structure is shown in Table 2. Based on the item means, a tendency to respond positively (that applies to one’s life) can be observed when the content reflects a socially valued attitude. Thus, statements related to self-reflection on one’s behaviors and emotions and the importance of understanding and empathizing with others have a higher average than statements that indicate a negative attitude towards social relationships or a self-perception of low competence in self-control. A tendency toward positive response bias can affect the instrument’s sensitivity by reducing variance. However, based on the results in Table 1, it can be concluded that participants did utilize the full scale from one to five.
Table 1: Descriptive statistics.
Table 2: Original factor structure of the Multidimensional Mentalizing Questionnaire.
Confirmatory factor analysis
We carried out a confirmatory factor analysis for the factorial structure proposed by Gori, Arcioni [2], as presented in Table 2. As can be seen in Table 3, the fit indicators and explained variance are below current standards [63]. Aiming to improve the fit and, at the same time, safeguard the simplicity and the parsimony of the model, we look for items that correlated with one or more additional factors different than the one to which they were initially associated based on theoretical and empirical grounds. Specifically, we examined the modification indices provided by the Lavaan package v. 0.6.15 [62] to identify items to which adding an extra parameter, i.e., a factor weight, substantially improved the fit indicators of the model. Following this rationale, five items exhibited substantial cross-loadings (18, 26, 30, 31, and 32). Three of these items originally belonged to the Reflexivity subscale, which had the largest number of items, and the remaining two belonged to Ego Strength, the second largest subscale. As shown in Table 3, the model’s fit indicators improved substantially by removing those items, placing them within the accepted psychometric standards for the common factors model [63]. The modified model also performed better than three alternative models: one factor, bifactor and hierarchical.
Table 3: Fit indices of the original and modified models.
Regarding the factor loadings (see Table 4), only two items in the reflexivity scale show loadings below 0.4. When comparing these factor weights with those of the original scale reported by Gori, Arcioni [2], it can be observed that the range of these values is not significantly different from those obtained in the version reported here, falling within an appropriate range. Similarly, the reliability indices for each are within an acceptable range (see Table 5). While these values might be considered relatively low, the small number of items per scale can account for them, as Cronbach’s Alpha is sensitive to the number of items on the scale being tested.
Table 4: Factor loading (lambda).
Table 5: Descriptive statistics for each subscale.
Finally, as seen in Table 6, the structure of correlations between the subscales is consistent with the underlying constructs. This can be primarily seen in the pattern of positive and negative correlations between the subscales related to good mentalization (Reflexivity, Ego Strength, and Relational Attunement) and those related to poor mentalization (Relational Discomfort, Distrust, and Emotional Dyscontrol). For example, Relational Discomfort has a strong positive correlation with Distrust (r = .70), contrasting with the negative correlation with Ego Strength (r = -.60). While moderate and strong correlations can be observed between some of the subscales, in general, correlations among them are low or non-existent, indicating a low level of redundancy in the overall scale.
Table 6: Correlations between MMQ subscales.
Convergent and divergent evidence
According to our predictions, higher scores on the positive MMQ are strongly associated with higher scores on the EQ (r = 0.53; p < 0.01), especially in the case of the cognitive empathy subscale (r = 0.56; p < 0.01). Although a small correlation was found with the complete IRI (r = 0.14; p > 0.05), it was observed that the positive MMQ has a moderate positive correlation with the perspective-taking (r = 0.34; p < 0.01) and empathic concern (r = 0.32; p < 0.01) subscales.
The negative MMQ only shows a weak negative correlation with the EQ (r = -0.26; p < 0.01), especially with social skills (r = -0.29; p < 0.01) and emotional reactivity (r = -0.27; p < 0.01). Among the IRI subscales, the negative MMQ had a weak negative correlation with perspective taking (r = -0.25; p < 0.01), but moderate positive correlation with personal distress (r = 0.36; p < 0.01). Low negative correlations are observed regarding the relationship between the negative MMQ and empathy scales.
As can be seen in Table 7, regarding the subscales of the positive MMQ, it can be observed that the strongest positive correlations were found between relational attunement of the positive MMQ and cognitive empathy of the EQ (r = 0.63; p < 0.01), as well as with empathic concern of the IRI (r = 0.72; p < 0.01). Additionally, there is a strong negative correlation between ego-strength of the positive MMQ and personal distress of the IRI (r = -0.59; p < 0.01).
Table 7: Correlations between MMQ, EQ, and IRI.
The MMQ also showed correlations with the BPAQ. A weak negative relationship was observed between the positive MMQ and the BPAQ (r = -0.20; p < 0.01). As can be seen in Table 7, the highest correlation was obtained between ego-strength and hostility (r = -0.41; p < 0.01). Strong correlations were found between the negative MMQ and the BPAQ (r = 0.64; p < 0.01), particularly with hostility (r = 0.68; p < 0.01). Hostility showed moderate to strong correlations with the subscales of relational discomfort (r = 0.75; p < 0.01), distrust (r = 0.56; p < 0.01), and emotional dyscontrol (r = 0.56; p < 0.01). Additionally, anger also positively correlated with emotional dyscontrol (r = 0.60; p < 0.01).
Further analyses: Gender differences and correlation with age
As it can be seen in Table 8, invariance analysis shows no difference between male and female. Comparisons between both groups show that women scored higher in their self-perception of good mentalizing and empathy than men. Similarly, women exhibit a lower tendency towards aggression, as measured by the BPAQ (see Table 9). In addition, we found an inverse association between the negative aspects of mentalization subscales and age. In other words, negative aspects of mentalization tend to decrease over time. The same tendency was observed in aggressive traits (see Table 10).
Table 8: Invariance analysis.
Table 9: Gender differences.
Table 10: Correlation with age.
Discussion
This paper examines psychometric properties and internal consistency of the first translation and adaptation of the MMQ into the Spanish, using a native Spanish-speaking sample in Chile. We first conducted a confirmatory factor analysis based on psychometric structure of the original test [reported in 2]. We then modify the instrument by eliminating the items showing cross-loadings with two or more factors and where adding the corresponding parameters would improve the model’s fit. A second factor analysis on the modified scale provide evidence of a good psychometric performance of the shorter and more parsimonious scale. To provide convergent and divergent evidence, we correlated the different subscales of the MMQ with all the subscales of the IRI and EQ, since both asses, indirectly, some components of mentalization. Also, we include an instrument measuring the tendency for aggressive behaviors, looking for evidence of a relationship between the ability to mentalize and the engagement in these types of behaviors. Finally, we explore gender differences and the association of the MMQ with age.
Our results provide evidence of consistency between the MMQ and other scales that indirectly measure the capacity for mentalization. Supporting our first hypothesis, our results show that positive mentalizing correlates with cognitive components of empathy, such as cognitive empathy as measured in the EQ and perspective-taking in the IRI. This reaffirms that positive mentalization is a fundamental component of empathy, and training mentalization could positively impact the development of better empathetic skills. The subscale of relational attunement shows strong positive correlations with cognitive empathy in the EQ and empathic concern in the IRI. Cognitive empathy is a component of empathy that involves representing the cognitive aspects of someone else’s emotional states, such as recognizing their affective beliefs, thoughts, or intentions [64]. The observed correlation reflects shared aspects between mentalizing and cognitive empathy, which involve their capacity to understand the other’s mental states by inferring their thoughts, beliefs, and emotions [22, 65]. Empathic concern refers to emotional responses such as compassion, sympathy, or care for others experiencing suffering or distress. Here, mentalization implies inferring the emotional experiences of others. This inference induces a sense of concern and empathy for the individual’s well-being, promoting social behaviors such as prosociality [66–68]. Relational attunement plays a special role in cognitive empathy and empathic concern. This latter dimension refers to the capacity to connect or align with someone else’s emotions, needs, or beliefs. By attuning to others and understanding their emotions and experiences, individuals can improve a cognitive understanding of other’s mental states and establish emotional connections with others. Additionally, an inverse relation between ego-strength and personal distress (IRI) was found. Ego-strength refers to an individual’s capacity to face adversity and cope with stressors and problems through self-regulation [69–71]. Importantly, people with a decreased capacity to manage and regulate their emotions adaptively appears to suffer more personal distress [72, 73], which denotes the negative emotional experience in response to these stressors [74].
Regarding our second hypothesis, we observed that personal distress and emotional reactivity positively correlate with bad mentalizing (negative MMQ). Bad mentalizing is measured through relational discomfort, distrust, and emotional dyscontrol, and it is the opposite pole of positive mentalizing. Negative mentalizing refers to failures and distortions in mentalizing, and it is related to problems in connecting with others. This might be produced by an increased emotional reactivity and impulsiveness, attitudes of closed-mindedness, distrust in relationships, and relational insecurity caused by the perception of being misunderstood [2]. This study shows that poor mentalizing is closely related to problems with perspective-taking and social skills. Previous literature established a relationship between poor mentalizing and aggressive traits [32]. Notably, a strong relation between mentalizing and aggressive traits was found in this study, especially in the case of bad mentalizing and hostility. We observed hostility related to relational discomfort, distrust, and emotional dyscontrol. Furthermore, emotional dyscontrol was correlated with anger. These results are in line with the obtained by Gori, Arcioni [2] where bad mentalizing was related to impulsiveness. These authors and others suggest that a self-regulation deficiency would underlie impulsive and negative reactions [2, 75]. Low ego-strength with high relational discomfort and distrust in relationships could lead to misunderstandings of the intentions and motivations of others. These misunderstandings could conduct to impulsivity and hostility as a primal adaptive response. In this sense, people may respond defensively or more aggressively due to increased discomfort or lack of trust [51, 76]. Additionally, deficiencies in emotional control are related to hostility and anger, since people with difficulties regulating their emotions may be more prone to be aggressive and hostile [77–79].
Our analysis found gender differences in mentalizing capacities. Previous studies have shown gender differences where women score higher than men in empathy measures [52, 80]. However, those scales are not specifically designed to measure mentalization capacities. In our study, women exhibit higher levels of reflexivity and relational attunement than men, indicating positive aspects of mentalizing. However, women also report a higher self-perception of emotional dyscontrol than men, which could be related to gender differences in emotional regulation strategies [81–83]. Further research is needed to clarify the connections between these results and how cultural factors could impact the development of mentalization abilities in different genders.
Finally, we observed in an exploratory analysis that the negative aspects of mentalization measured in the MMQ tend to decrease with age. This interesting finding offers the opportunity to address mentalization from the perspective of the subjects’ life cycle and developmental stage. Arguably, the decrease in negative aspects of mentalization could be explained by the way in which life experiences shape relational discomfort, distrust, and emotional dyscontrol. Integrating meaningful life experiences into understanding others would improve emotional regulation and a greater ability to navigate relationships effectively [84, 85]. It is important to note that these results are exploratory and should be interpreted with caution considering that our sample has a mean age of 29.32 years old and the distribution is positively skewed. Moreover, future work should address the generalizability of our findings across life span through invariance analysis. In sum, further research is needed to gain a more comprehensive understanding of gender differences and age-related patterns in mentalization.
It is also important to note that measuring mentalization capacity through self-reporting poses a challenge shared with other self-report instruments that measure specific capacities without directly observing performance in a task that assesses that capacity. In fact, we can argue that the MMQ measures individuals’ self-perception of their mentalization abilities. It is a matter of debate and empirical investigation to determine how self-perception of competence is related to actual performance in tasks or activities that require that competence for execution. Concerning this, one possible avenue for research would be to correlate self-perception of mentalization with the judgments of others who interact with the individuals being evaluated on a daily basis. Crossed-examinations of mentalizing capacities from the 1^st^ and 3^rd^ person could enrich the use of self-report-based methods. Similarly, it could be valuable to associate the results of comprehensive psychological interviews and assessments with the scores obtained on the MMQ. By incorporating these approaches, researchers could gain a broader understanding of the relationship between self-perception of mentalization, external assessments, and objective performance in tasks that require mentalization abilities. This would contribute to the ongoing investigation and refinement of mentalization measurement tools.
The availability of an instrument that measures mentalization in various dimensions, acknowledging the complexity of this capacity, allows us to advance our understanding of it in clinical populations. Future research could compare MMQ’s results in different clinical populations with non-clinical control samples to understand how mentalizing works in those diagnoses. With this, more specific interventions focused on training mentalizing abilities could be developed. Additionally, an instrument of this kind enables us to study potential differences and invariances of the construct based on gender and stage of the life cycle. Furthermore, it allows us to conduct transcultural research on this fundamental human capacity for sociability, which may vary to different degrees among individuals from different cultural backgrounds and environments. In conclusion, an instrument that measures mentalization, accounting for the complexity of the construct, provides the opportunity for conducting research and clinical interventions. Moreover, making this type of instrument available in different languages allows us to explore the variations of mentalization capacity across different cultural backgrounds.
In conclusion, the Spanish adaptation of the MMQ presented in this work demonstrates robust psychometric properties in the Chilean population. The study provides evidence of how the different dimensions of mentalizing may be related to empathic abilities and aggressive behaviors. Considering that the original version was developed in Italian, it is crucial to address potential cultural differences, as they may influence the behavioral expression of mentalization and item functioning [86, 87]. Therefore, we advocate for cross-cultural studies that, among other questions, test cultural invariance. Additionally, exploring the relationship between age and mentalization and other pertinent demographic analyses in forthcoming investigations is crucial. Finally, the adaptation of the MMQ presented in this paper is the first tool that will serve for self-administered measurements of mentalization in Chile, providing a standardized and valid measure that can inform psychological treatment and research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bateman A, Fonagy P. Mentalization based treatment for borderline personality disorder. World psychiatry. 2010;9(1). doi: 10.1002/j.2051-5545.2010.tb 00255.x 20148147 PMC 2816926 · doi ↗ · pubmed ↗
- 2Gori A, Arcioni A, Topino E, Craparo G, Lauro Grotto R. Development of a new measure for assessing mentalizing: The multidimensional mentalizing questionnaire (MMQ). Journal of Personalized Medicine. 2021;11(4). doi: 10.3390/jpm 11040305 33921083 PMC 8071450 · doi ↗ · pubmed ↗
- 3Fonagy P, Campbell C, Luyten P. Attachment, Mentalizing and Trauma: Then (1992) and Now (2022). Brain Sciences. 2023;13(3). doi: 10.3390/brainsci 13030459 36979268 PMC 10046260 · doi ↗ · pubmed ↗
- 4Green MF, Penn DL, Bentall R, Carpenter WT, Gaebel W, Gur RC, et al. Social cognition in schizophrenia: an NIMH workshop on definitions, assessment, and research opportunities. Schizophrenia bulletin. 2008;34(6):1211–20. doi: 10.1093/schbul/sbm 145 18184635 PMC 2632490 · doi ↗ · pubmed ↗
- 5Javed A, Charles A. The importance of social cognition in improving functional outcomes in schizophrenia. Frontiers in Psychology. 2018;9:157.29740360 10.3389/fpsyt.2018.00157 PMC 5928350 · doi ↗ · pubmed ↗
- 6CavieresÁ, López-Silva P. Social perception deficit as a factor of vulnerability to psychosis: a brief proposal for a definition. Frontiers in Psychology. 2022;13. doi: 10.3389/fpsyg.2022.805795 35645890 PMC 9131014 · doi ↗ · pubmed ↗
- 7Savla GN, Vella L, Armstrong CC, Penn DL, Twamley EW. Deficits in domains of social cognition in schizophrenia: a meta-analysis of the empirical evidence. Schizophrenia bulletin. 2013;39(5):979–92. doi: 10.1093/schbul/sbs 080 22949733 PMC 3756768 · doi ↗ · pubmed ↗
- 8Montag C, Brandt L, Lehmann A, De Millas W, Falkai P, Gaebel W, et al. Cognitive and emotional empathy in individuals at clinical high risk of psychosis. Acta Psychiatrica Scandinavica. 2020;142(1):40–51. doi: 10.1111/acps.13178 32339254 · doi ↗ · pubmed ↗