Cancer mortality in workers at risk of occupational exposure to ionizing radiation in a company in the nuclear sector headquarters in São Paulo
Glacy Sabra Vieira, Maria Carmen Martinez, Maria Regina Alves Cardoso

TL;DR
This study found lower cancer mortality in workers exposed to radiation compared to the general population and among monitored workers compared to unmonitored ones in São Paulo.
Contribution
The study provides new evidence on cancer mortality differences in radiation-exposed workers using a specific nuclear sector cohort.
Findings
Cancer mortality was significantly lower in exposed workers compared to the general population (SMR=0.224).
Monitored workers had lower cancer mortality than unmonitored workers (SMR=0.685).
The healthy worker effect was observed in the external analysis.
Abstract
To compare cancer mortality among workers exposed to gamma and X radiation and the general population of the city of São Paulo, as well as that of the subgroup monitored with those not monitored for gamma and X radiation in a work unit with ionizing radiation based in the city of São Paulo. Between 2016 and 2021, a retrospective open cohort study was carried out with workers who were employed from 08/31/1956 to 12/31/2016 based on data collected at the company and in official institutions. Standardized mortality ratios (SMR) were calculated by sex, age and calendar period of cancers grouped according to type, risk factor and organ system in two analyses: in the external analysis, the mortality of the study population was compared with that of the general population of the city of São Paulo; In the internal analysis, the mortality of the monitored subgroup was compared with that of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
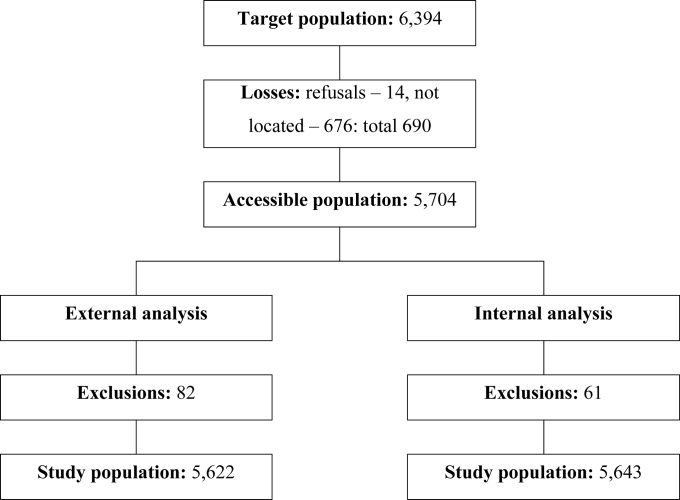 Figure 1
Figure 1| Characteristics | Males | Females | Total | ||||
|---|---|---|---|---|---|---|---|
| N° | % | N° | % | N° | % | ||
| Age range (in years) at the end of follow-up | |||||||
| 15 ├ 35 | 42 | 1.0 | 15 | 1.0 | 57 | 1.0 | |
| 35 ├ 50 | 256 | 6.1 | 133 | 9.1 | 389 | 6.9 | |
| 50 ├ 60 | 1,542 | 36.9 | 473 | 32.2 | 2,015 | 35.7 | |
| ≥60 | 2,334 | 55.9 | 848 | 57.7 | 3,182 | 56.4 | |
| Calendar period for employment | |||||||
| 1956 to 1959 | 45 | 1.1 | 9 | 0.6 | 54 | 1.0 | |
| 1960 to 1969 | 274 | 6.6 | 106 | 7.2 | 380 | 6.7 | |
| 1970 to 1979 | 1,810 | 43.4 | 727 | 49.5 | 2,537 | 45.0 | |
| 1980 to 1989 | 1,857 | 44.5 | 488 | 33.2 | 2,345 | 41.6 | |
| 1990 to 1999 | 98 | 2.3 | 84 | 5.7 | 182 | 3.2 | |
| 2000 to 2016 | 90 | 2.2 | 55 | 3.7 | 145 | 2.6 | |
| Length of employment (in years) | |||||||
| Less than 1.0 | 930 | 22.3 | 255 | 17.4 | 1,185 | 21.0 | |
| 1.0 to 4.9 | 1,621 | 38.8 | 457 | 31.1 | 2,078 | 36.8 | |
| 5.0 to 9.9 | 446 | 10.7 | 181 | 12.3 | 627 | 11.1 | |
| 10.0 to 19.9 | 342 | 8.2 | 163 | 11.1 | 505 | 8.9 | |
| 20.0 to 29.9 | 291 | 7.0 | 204 | 13.9 | 495 | 8.8 | |
| 30.0 to 39.9 | 473 | 11.3 | 177 | 12.0 | 650 | 11.5 | |
| 40.0 to 49.9 | 69 | 1.7 | 32 | 2.2 | 101 | 1.8 | |
| 50.0 or more | 2 | 0.0 | 0 | 0.0 | 2 | 0.0 | |
| Characteristics of the position held | |||||||
| High-level position | 273 | 6.5 | 183 | 12.5 | 456 | 8.1 | |
| Mid-level position | 2,046 | 49.0 | 774 | 52.7 | 2,820 | 50.0 | |
| Hybrid position (mid- and higher-level) | 1,789 | 42.9 | 443 | 30.2 | 2,232 | 39.6 | |
| Unknown | 66 | 1.6 | 69 | 4.7 | 135 | 2.4 | |
| Risk of exposure to gamma and X radiation | |||||||
| No | 1,664 | 39.9 | 691 | 47.0 | 2,355 | 41.7 | |
| Yes | 2,510 | 60.1 | 778 | 53.0 | 3,288 | 58.3 | |
| Vital status at the end of follow-up | |||||||
| Alive | 3,532 | 84.6 | 1,330 | 90.5 | 4,862 | 86.2 | |
| Died from cancer | 139 | 3.3 | 57 | 3.9 | 196 | 3.5 | |
| Died from other causes | 503 | 12.1 | 82 | 5.6 | 585 | 10.4 | |
| Total | 4,174 | 100.0 | 1,469 | 100.0 | 5,643 | 100.0 | |
| Characteristics | Males | Females | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N° | % | CMR | N° | % | CMR | N° | % | CMR | ||
| Causes | ||||||||||
| All causes | 642 | 100.0 | 698.6 | 139 | 100.0 | 431.2 | 781 | 100.0 | 629.2 | |
| All cancers | 139 | 21.7 | 151.3 | 57 | 41.0 | 176.8 | 196 | 25.1 | 157.9 | |
| All causes except cancer | 503 | 78.3 | 547.4 | 82 | 59.0 | 254.4 | 585 | 74.9 | 471.3 | |
| Organic system | ||||||||||
| Digestive | 64 | 46.0 | 69.6 | 16 | 28.1 | 49.6 | 80 | 40.8 | 64.4 | |
| Respiratory | 32 | 23.0 | 34.8 | 10 | 17.5 | 31.0 | 42 | 21.4 | 33.8 | |
| Genitourinary | 15 | 10.8 | 16.3 | 21 | 36.8 | 65.1 | 36 | 18.4 | 29.0 | |
| Hematogenous | 13 | 9.4 | 14.1 | 5 | 8.8 | 15.5 | 18 | 9.2 | 14.5 | |
| Musculoskeletal | 3 | 2.2 | 3.3 | 2 | 3.5 | 6.2 | 5 | 2.6 | 4.0 | |
| Eyes and Central Nervous System | 6 | 4.3 | 6.5 | 2 | 3.5 | 6.2 | 8 | 4.1 | 6.4 | |
| Skin | 1 | 0.7 | 1.1 | 1 | 1.8 | 3.1 | 2 | 1.0 | 1.6 | |
| Uncertain | 5 | 3.6 | 5.4 | 0 | 0.0 | 0.0 | 5 | 2.6 | 4.0 | |
| Total | 139 | 100.0 | 151.3 | 57 | 100.0 | 176.8 | 196 | 100.0 | 157.9 | |
| Males | Females | Total | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| O | E | SMR | 95%CI | O | E | SMR | 95%CI | O | E | SMR | 95%CI | |||
| Causes of death | ||||||||||||||
| All causes | 623 | 2,717.5 | 0.229 | 0.462–0.541 | 137 | 677.6 | 0.202 | 0.170–0.239 | 760 | 3,395.0 | 0.224 | 0.208–0.240 | ||
| All cancers | 137 | 352.0 | 0.389 | 0.327–0.460 | 56 | 88.0 | 0.636 | 0.481–0.826 | 193 | 440.0 | 0.439 | 0.379–0.505 | ||
| All causes except cancer | 486 | 2,365.4 | 0.205 | 0.188–0.225 | 81 | 589.6 | 0.137 | 0.109–0.171 | 567 | 2,955.0 | 0.192 | 0.176–0.208 | ||
| Cancer groups | ||||||||||||||
| Type | ||||||||||||||
| Solid | 119 | 308.3 | 0.386 | 0.320–0.462 | 51 | 75.8 | 0.673 | 0.501–0.884 | 170 | 384.1 | 0.443 | 0.379–0.514 | ||
| Unspecified | 5 | 18.5 | 0.270 | 0.087–0.629 | 0 | 5.2 | 0.000 | ---. 0.701 | 5 | 23.8 | 0.210 | 0.068–0.491 | ||
| Hematogenous | 13 | 24.9 | 0.523 | 0.278–0.894 | 5 | 6.9 | 0.720 | 0.232–1.679 | 18 | 31.8 | 0.566 | 0.335–0.895 | ||
| Risk factor | ||||||||||||||
| Related to alcoholism | 51 | 138.5 | 0.368 | 0.274–0.484 | 29 | 37.2 | 0.779 | 0.521–1.118 | 80 | 175.7 | 0.455 | 0.361–0.567 | ||
| Related to smoking | 96 | 234.6 | 0.409 | 0.331–0.500 | 26 | 43.0 | 0.605 | 0.395–0.886 | 122 | 277.6 | 0.439 | 0.365–0.525 | ||
| Related to work | 94 | 232.4 | 0.405 | 0.327–0.495 | 48 | 61.5 | 0.780 | 0.575–1.035 | 142 | 293.9 | 0.483 | 0.537–0.647 | ||
| Gamma and X radiation | 77 | 191.0 | 0.403 | 0.318–0.504 | 45 | 51.5 | 0.873 | 0.637–1.168 | 122 | 242.5 | 0.503 | 0.418–0.601 | ||
| Organic system | ||||||||||||||
| Digestive | 63 | 149.7 | 0.421 | 0.323–0.538 | 15 | 30.2 | 0.497 | 0.278–0.820 | 78 | 179.9 | 0.434 | 0.343–0.541 | ||
| Respiratory | 32 | 73.8 | 0.434 | 0.297–0.612 | 10 | 9.8 | 1.017 | 0.487–1.871 | 42 | 83.6 | 0.502 | 0.362–0.679 | ||
| Genitourinary | 15 | 62.1 | 0.242 | 0.135–0.399 | 21 | 29.5 | 0.712 | 0.440–1.088 | 36 | 91.6 | 0.393 | 0.275–0.544 | ||
| Musculoskeletal | 3 | 4.3 | 0.691 | 0.139–2.020 | 2 | 1.3 | 1.516 | 0.170–5.470 | 5 | 5.7 | 0.883 | 0.285–2.062 | ||
| Skin | 1 | 5.8 | 0.173 | 0.002–0.961 | 1 | 1.2 | 0.850 | 0.011–4.715 | 2 | 7.0 | 0.287 | 0.032–1.036 | ||
| Eyes and Central Nervous System | 5 | 11.6 | 0.432 | 0.139–1.008 | 2 | 3.3 | 0.608 | 0.068–2.195 | 7 | 14.9 | 0.471 | 0.189–0.971 | ||
| Endocrine | 0 | 1.5 | 0.000 | ---. 2.397 | 0 | 0.6 | 0.000 | ---. 5.731 | 0 | 2.2 | 0.000 | ---. 1.690 | ||
| Hematopoietic | 13 | 26.0 | 0.501 | 0.266–0.856 | 5 | 7.2 | 0.693 | 0.223–1.616 | 18 | 33.2 | 0.543 | 0.321–0.857 | ||
| Undetermined | 5 | 17.0 | 0.295 | 0.095–0.687 | 0 | 4.8 | 0.000 | ---. 0.761 | 5 | 21.8 | 0.229 | 0.074–0.535 | ||
| Males | Females | Total | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| O | E | SMR | 95%CI | O | E | SMR | 95%CI | O | E | SMR | 95%CI | |||
| Causes of death | ||||||||||||||
| All causes | 316 | 470.6 | 0.671 | 0.599–0.750 | 62 | 81.3 | 0.763 | 0.585–0.978 | 378 | 551.9 | 0.685 | 0.618–0.758 | ||
| All cancers | 72 | 95.3 | 0.756 | 0.591–0.952 | 23 | 36.1 | 0.637 | 0.404–0.956 | 95 | 131.4 | 0.723 | 0.585–0.884 | ||
| All causes except cancer | 244 | 375.4 | 0.650 | 0.571–0.737 | 39 | 45.2 | 0.863 | 0.613–1.179 | 283 | 420.6 | 0.673 | 0.597–0.756 | ||
| Cancer groups | ||||||||||||||
| Type | ||||||||||||||
| Solid | 62 | 83.7 | 0.741 | 0.568–0.949 | 20 | 34.2 | 0.586 | 0.357–0.904 | 82 | 117.9 | 0.696 | 0.553–0.864 | ||
| Unspecified | 3 | 0.0 | --- | ---. --- | 0 | 2.2 | 0.000 | ---. 1.645 | 3 | 2.2 | 1.344 | 0.270–3.931 | ||
| Hematogenous | 7 | 8.5 | 0.826 | 0.331–1.703 | 3 | 1.9 | 1.555 | 0.312–4.542 | 10 | 10.4 | 0.961 | 0.460–1.768 | ||
| Risk factor | ||||||||||||||
| Related to alcoholism | 29 | 32.8 | 0.885 | 0.592–1.271 | 13 | 18.3 | 0.709 | 0.377–1.213 | 42 | 51.1 | 0.822 | 0.592–1.111 | ||
| Related to smoking | 49 | 68.2 | 0.719 | 0.532–0.951 | 8 | 20.2 | 0.395 | 0.170–0.779 | 57 | 88.4 | 0.645 | 0.488–0.836 | ||
| Related to work | 53 | 61.8 | 0.858 | 0.642–1.122 | 20 | 31.1 | 0.643 | 0.393–0.993 | 73 | 92.9 | 0.786 | 0.616–0.988 | ||
| Gamma and X radiation | 44 | 50.5 | 0.871 | 0.633–1.169 | 19 | 29.2 | 0.651 | 0.392–1.017 | 63 | 79.7 | 0.790 | 0.607–1.011 | ||
| Organic system | ||||||||||||||
| Digestive | 36 | 39.4 | 0.913 | 0.639–1.264 | 6 | 10.6 | 0.564 | 0.206–1.227 | 42 | 50.1 | 0.839 | 0.604–1.134 | ||
| Respiratory | 12 | 28.7 | 0.418 | 0.216–.730 | 3 | 7.5 | 0.399 | 0.080–1.167 | 15 | 36.2 | 0.414 | 0.232–0.683 | ||
| Genitourinary | 8 | 9.9 | 0.804 | 0.346–1.584 | 8 | 13.8 | 0.581 | 0.250–1.145 | 16 | 23.7 | 0.674 | 0.385–1.095 | ||
| Musculoskeletal | 2 | 1.3 | 1.589 | 0.178–5.731 | 2 | 0.0 | --- | ---. --- | 4 | 1.3 | 3.177 | 0.854–8.128 | ||
| Skin | 0 | 1.3 | 0.000 | ---. 2.911 | 1 | 0.0 | --- | ---. --- | 1 | 1.3 | 0.794 | 0.010–4.416 | ||
| Eyes and Central Nervous System | 4 | 3.1 | 1.296 | 0.348–3.314 | 0 | 2.2 | 0.000 | ---. 1.645 | 4 | 5.3 | 0.752 | 0.202–1.925 | ||
| Endocrine | 0 | 0.0 | --- | ---. --- | 0 | 0.0 | --- | ---. --- | 0 | 0.0 | --- | ---. --- | ||
| Hematopoietic | 7 | 8.5 | 0.826 | 0.331–1.703 | 3 | 1.9 | 1.555 | 0.312–4.542 | 10 | 10.4 | 0.961 | 0.460. –1.768 | ||
| Undetermined | 3 | 3.1 | 0.972 | 0.195–2.837 | 0 | 0.0 | --- | ---. --- | 3 | 3.1 | 0.972 | 0.195–2.837 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiation Dose and Imaging · Effects of Radiation Exposure
INTRODUCTION
Ionizing radiation is a carcinogen, and the relationship between exposure dose and cancer risk is linear and limitless^ 1 ^. Safety limits for work are based on populations exposed to single high dose or on patients exposed to high doses of radiotherapy^ 2–4 ^, in addition to experimental studies; but occupational exposure is chronic at low doses. To clarify doubts about the validity of safety limits for work, cohort studies of nuclear industry workers were carried out in developed countries and did not demonstrate conclusive results regarding the association between occupational exposure to ionizing radiation and cancer mortality, although some positive associations have been found^ 1 ^ in relation to lung^ 5,6 ^ and prostate^ 7,8 ^ cancer, multiple myeloma^ 9–12 ^, and leukemia^ 10–14 ^. No studies of this nature were identified with Brazilian workers.
The questioning regarding illness and death from cancer resulting from exposure to ionizing radiation in the work environment from a radiological and nuclear company in the city of São Paulo, combined with the lack of national studies, gave rise to this study, which aimed to compare cancer mortality among workers exposed to ionizing radiation with mortality in the general population of the city of São Paulo and the subgroups monitored and not monitored for gamma and X radiation in a work unit based in the city of São Paulo.
METHODS
Study design and population
Open historical cohort in a target population of 6,394 workers from a public company in the city of São Paulo (SP) in the research, development, and applications in the radiological and nuclear areas. The cohort began on 08/31/1956, the date of the company's founding, and ended on 12/31/2016. Each worker was included in the cohort from the date they joined the company, and the end of follow-up corresponded to the date of death or the end of the cohort.
Inclusion criteria included having a formal employment record and at least one day of work at the company, after which workers would be at risk of exposure to gamma and X radiation. Workers who refused to participate were considered losses of the study as well as the lack of information about whether or not workers had passed away.
Sources and data collection
Identification, demographic, and functional data were obtained from records from the company's administrative sector, that is: name, date of birth, affiliation, hometown, General Registration (Brazilian identification document – RG) of the Public Security Secretariats, Individual Taxpayer Registration (CPF), voter ID, start and end date of employment, initial education, positions occupied and date of death (if applicable). Information on exposure to gamma and X radiation was obtained from monthly dosimetric records from the reading of individual external chest dosimeters at the company from 1961 to 2016.
Mortality data were only available at the company and in official sources limited to the state of São Paulo, namely the Mortality Information Improvement Program of the Municipal Health Secretariat of the Municipality of São Paulo (Programa de Aprimoramento de Informações de Mortalidade da Secretaria Municipal de Saúde do Município de São Paulo – PRO-AIM), the Information Center Health Surveillance Strategies of the Health Secretariat of the state of São Paulo (Centro de Informações Estratégicas de Vigilância em Saúde da Secretaria da Saúde do Estado de São Paulo – CIEVS-SP), and the SEADE Foundation. Consultation of the databases in PRO-AIM and CIEVS-SP used the probabilistic linkage technique (by crossing the name, name of the mother, and date of birth) and in SEADE, deterministic linkage (by crossing the name, name of the mother, date of birth, name of the father, hometown, CPF, RG, dates of start and end of employment) with preference given to PRO-AIM records. The underlying cause of death was recorded according to the International Classification of Diseases – 10^th^ Revision (ICD-10).
To classify the vital status of each worker, workers reportedly dead were considered "deceased" and a worker who was receiving a salary or pension was considered "alive." By consulting the database and the homepage of the Regional Electoral Court with national coverage^ 15 ^ and the homepage of the Federal Revenue Service^ 15 ^, those with regular voter ID and CPF were considered "alive," those with death information were considered "deceased," and those missing information were considered "ignored."
Demographic and mortality records for the city of São Paulo were obtained from DATASUS^ 16 ^ from 1996 to 2016, and underlying causes of death were recorded according to ICD-10.
Study variables
Sociodemographic and functional variables: gender, date of birth, start and end date of employment, end date of monitoring in the cohort, age at start and end of employment, age at death (deceased), age at end date of cohort (living), positions (categorized according to level of education into mid-level positions, higher level positions, transition from mid-level to higher level positions, and unknown).
Exposure to gamma and X radiation: were categorized into monitored and unmonitored subgroups for exposure to gamma and X radiation^ 17 ^.
Vital status: alive, deceased or unknown.
Causes of death: death records were categorized into all causes, all cancers, all causes except cancer, and by cancer site. Cancer categories considered, according to ICD-10, the group of malignant neoplasms (C00 to C97)^ 18 ^, in situ neoplasms (D00 – D09), benign neoplasm of brain^ 19 ^ (D32 and D33), and neoplasms of uncertain or unknown behavior (D37–D48). Deaths of unknown underlying cause were coded as R99 by the researcher.
Neoplasms were grouped according to type (solid, unspecified, and hematopoietic), risk factors (alcohol consumption, smoking, work, and exposure to gamma and X radiation)^ 20 ^, and organic systems according to the ICD-10 classification of neoplasms^ 16 ^ (Chart A of the Supplementary Material).
Statistical analyses
Descriptive analysis stratified by gender of the quantitative variables was carried out using means, medians, standard deviations, minimum and maximum values; proportions were set from the qualitative variables. Crude mortality rates (CMR) were estimated by dividing the number of deaths observed by the number of person-years, which comprises the number of years that workers attended follow-up between the start and end dates from the cohort.
Compare the risk of mortality between populations (exposed and unexposed) was carried out by the use of standardized mortality ratio (SMR), obtained by dividing the number of deaths observed by the number of deaths expected using the indirect method^ 21,22 ^. SMR were stratified by gender, age, and calendar period (calculation method described in the Supplementary Material). A 95% confidence interval (95%CI) was considered for statistical significance.
External analysis compared mortality in the study population with that in the city of São Paulo from 1996 to 2016. Age groups at the end of follow-up were 15 to 34.9 years old, 35 to 49.9 years old, and 50 years old or older. Calendar periods were 01/01/1996–12/31/2002, 01/01/2003–12/31/2009, and 01/01/2010–12/31/2016. Internal analysis compared the mortality of monitored workers with the mortality of unmonitored workers from 1993 to 2016, given the reduced number of death records prior to 1993. Age groups at the end of follow-up were 15 to 34.9 years old, 35 to 49.9 years old, and 50 years old and older. Calendar periods were 01/01/1993–12/31/2000, 01/01/2001–12/31/2008, and 01/01/2009–12/31/2016.
Software
Microsoft Excel, version 365, was used to calculate the crude and standardized rates. STATA – Statistics/Data Analysis, version 13.1, was used for descriptive analyses and the calculation of standardized ratios.
Ethical aspects
The study was approved by the Research Ethics Committee of the School of Public Health of Universidade de São Paulo, CAAE No. 54944616.6.0000.5421 of 08/29/2016. The company authorized the study to be carried out with workers who signed the Informed Consent. For workers who could not be contacted, the Term of Responsibility was approved by the Research Ethics Committee of the Municipal Health Secretariat of the Municipality of São Paulo on 08/31/2018.
RESULTS
6,394 workers’ records were found, of which 676 were lost to follow-up and 14 refused to participate, totaling 690 (10.8%) losses, with 5,704 (89.2%) remaining workers. 82 workers who ended follow-up before 1996 were excluded from external analysis, leaving a study population of 5,622 (87.9%) workers. From internal analysis, 61 participants who ended follow-up before 1993 were excluded, making up a study population of 5,643 (88.3%) workers. Steps are illustrated in Figure 1.
Target population and study population; company working in research, development, and applications in the radiological and nuclear areas, São Paulo, 1993–2016.
Table 1 shows the characteristics of the study population, consisted majorly of males (74.0%), aged 60 years old or older (56.4%), with a mean of 61.7 years (SD=9.9).
For both genders, mean follow-up time was 35.3 years (SD=8.9). The majority of the population had been employed for less than 5 years (57.8%), with a mean of 9.5 years (SD=12.4).
Workers in mid-level positions were the most frequent (50.0%), followed by those who moved from mid- to higher level positions (39.6%).
External monitoring due to risk of exposure to gamma and X radiation was observed in 58.3% of workers. Among the workers monitored, 69.5% had an accumulated radiation dose below 10.0 mSv. The mean accumulated dose in the monitored subgroup was 14.9 mSv (SD=35.7), with a median of 3.0 mSv, a minimum of 0.0 mSV, and a maximum of 656.2 mSv.
At the end of follow-up, 781 (13.8%) workers had died. Cardiovascular diseases were the main causes of deaths, accounting for 224 of them (28.8%); neoplasms were the second most common cause of death, with 196 (25.1%) cases; and undefined or unspecified causes were the third, with 15.4% of deaths (the Supplementary Material presents Table A, which shows deaths according to ICD-10 chapters, and Table B, which shows deaths due to cancer by site).
In relation to the positions held, a higher proportion of cancer deaths was observed in the category of higher-level positions (38.0%), followed by the category of mid-level positions that migrated to higher-level ones (28.9%), higher-level positions (22.2%), and unknown (12.5%).
CMR for all causes was 629.2/100,000 person-year, being higher among men than women. CMR for all cancers was 157.9/100,000 person-year, being higher among women than men. Considering organic systems, the largest CMR due to neoplasms were in the digestive (64.4/100,000), respiratory (33.8/100,000), and genitourinary systems (29.0/100,000), and hematogenous neoplasms (14.5/100,000) (Table 2).
Table 3 shows SMR in external analysis. A lower risk of deaths from all causes was observed in the study population with SMR=0.224 (95%CI 0.208–0.240) when compared to the population of the city of São Paulo, as well as between men and women.
External analysis showed a lower risk of death from all cancers in the study population, with SMR=0.439 (95%CI 0.379–0.505) when compared to the population of the city of São Paulo, a pattern also observed among men and women.
Similar results were observed in relation to deaths by types of cancer (solid, unspecified, and hematogenous), by risk factor (alcoholism, smoking, work, and gamma and X radiation), and between the different organic systems. Exceptions occurred in females, showing no statistically significant difference in relation to the city of São Paulo in terms of deaths from hematogenous cancers, cancers related to alcoholism, work, gamma and X radiation, and almost all organic systems.
Table 4 shows SMR in the internal analysis. A lower risk of deaths from all causes was observed in the monitored subgroup with SMR=0.685 (95%CI 0.618–0.758) when compared to the unmonitored subgroup, as well as between men and women.
Internal analysis showed a lower risk of death from all cancers in the monitored subgroup with SMR=0.723 (95%CI 0.585–0.884) when compared to the unmonitored subgroup, in males and females.
The results observed showed that deaths by types of cancer (solid, unspecified, and hematogenous), by risk factor (alcoholism, smoking, work, and gamma and X radiation), and between different organic systems did not present statistically significant differences between the monitored and unmonitored subgroups. Exceptions occurred among solid cancers, those related to smoking and the respiratory system, which showed a lower risk of death among the ones followed-up.
DISCUSSION
This work sought to compare cancer mortality among workers at a company in the radiological and nuclear areas in the city of São Paulo with the general population of workers followed-up and not followed-up for gamma and X radiation.
The main causes of death were cardiovascular diseases, neoplasms and ill-defined causes, a profile similar to that currently observed worldwide^ 23 ^ and in Brazil^ 24 ^, although, in some countries, cancers are the first cause of death in the age range up to 69 years old^ 25 ^. Ill-defined causes were possibly due to limited quality of available data, including potential under-registration of cancer deaths in the state of São Paulo and coverage of death registration periods, initiated by PRO-AIM in the city of São Paulo in 1996, with no records of deaths among workers prior to that period and in other locations.
Standardized mortality ratios in external analysis showed that the risks of death from all causes were lower in the study population, in males and females, compared to those in the city of São Paulo. These results suggest the healthy worker effect. In relation to other studies^ 10,11,13,26–29 ^, SMR were not as low as those observed in this study. This points to the contribution that limited information on deaths may have had on this result as well as to the positive effects of preventive strategies applied to the study population.
The risk of deaths from all cancers showed a less pronounced reduction than the risk of deaths from all causes (excluding cancers), when compared with the population of the city of São Paulo. This was observed in the study population and both in male and female strata. This difference between standardized mortality ratios (from all causes except cancer and from cancer) is consistent with the healthy worker effect, which is generally less marked for cancer deaths than for other causes of death^ 13,14,30,31 ^.
Among the factors that may have contributed to the healthy worker effect were access to health services by the study population, both through medical insurance and occupational health services, promoting treatment of diseases, examinations to detect risk factors of cardiovascular diseases and cancer screening, leading to a reduction in mortality^ 31 ^. The higher proportion of cancer deaths in the highest socioeconomic level shows that access to education and medical care may have led to an increase in cancer diagnoses.
Occupational exposure in the external analysis was assessed indirectly through the selection of cancers related to occupational exposures with sufficient evidence in humans^ 20 ^. Even without the selection of cancers related only to chemical substances, this allowed the indirect assessment of exposure to chemicals, for which no systematic records were found in the company. Both men and women in the study population had a lower risk of mortality from cancers associated with occupational exposure. A similar result was obtained through the analysis of the group of radiogenic cancers with sufficient evidence in humans^ 20 ^, which showed a lower risk of death due to exposure to gamma and X radiation in the study population, among men and women, which was also observed in other studies^ 3 ^. These results can again be attributed to preventive strategies and access to health care; however, they do not rule out the possibility that individually considered cases may be linked to exposure to carcinogenic agents present in the work environment.
Internal mortality analysis evaluated the monitored subgroup against the non-monitored one using the latter as a reference. Internal analysis had the advantage of comparing more similar populations in relation to factors linked to the healthy worker effect. Results showed that the monitored subgroup, of men and women, had a lower risk of mortality from all causes compared to the unmonitored one. This result suggests an internal healthy worker effect^ 3,32,33 ^. In relation to cancer mortality, there was a lower risk of cancer deaths in the monitored subgroup and between the male and female strata. Similar results were found in the literature^ 2,3,32 ^.
Lower SMR was more marked in mortality from all causes than from all cancers among monitored men and in the monitored subgroup, but among monitored women, this reduction was more present in mortality from all cancers. This result may be a random event due to the small number of deaths among women, or point to the possibility that women resorted to screening and detection of cancers. Breast cancer can be detected in the early stages through mammography and cervical cancer through oncotic cytology, both screening methods that are already well established in public health^ 34–36 ^.
Results showed that there were no differences between the two groups in relation to deaths by types of cancer (solid, unspecified, and hematogenous), by risk factors (alcoholism, smoking, work, and gamma and X radiation), and between the different organic systems. Exceptions were solid cancers, those related to smoking and those of the respiratory system. These results suggest that there are possibly fewer smokers among monitored workers. Literature studies show that smoking is unlikely to be a risk factor for cancer among workers in the nuclear industry^ 37,38 ^. Other studies have shown similar results^ 39,40 ^.
The only organic system that showed a statistically significant increase in the risk of death in the monitored subgroup was the musculoskeletal system. However, due to the small number of deaths, it may have been a random event. Similar results have been reported in the literature^ 5,40–42 ^.
Successes and limitations
The main limitations of the study regarded access and quality of data. Death records were restricted to the state of São Paulo; however, this is the state with the best socioeconomic level and mortality records. The relatively small number of deaths, especially among women, determined the option of grouping cancers in order to obtain more consistent results.
Flaws in dosimetric records, especially in the initial phases of the company, were also a limitation. Furthermore, 70% of the monitored population had an accumulated radiation dose of up to 10 mSv. This characteristic, positive from the worker's health point of view, was an impediment to an assessment by accumulated dose stratum, determining the categorization between monitored and unmonitored.
Despite the relatively small number of deaths, the option for standardized mortality ratio analysis provided consistent results, evaluating monitored and unmonitored workers for gamma and X radiation.
As a success, the 60-year follow-up of a cohort of workers is highlighted, a desirable period to analyze cancer mortality, which was a great benefit. The study also allowed to analyze a population with the majority of men and women over 50 years of age, a desirable age range for analyzing cancer mortality.
Although international cohorts of nuclear industry workers have had a larger number of participants^ 3–5,7,8,11,12,27,28,42 ^, this cohort had a relevant number and took place in one of the largest companies in this field in Brazil, making it possible to add knowledge to the national reality. Furthermore, this is one of the few evaluations of cancer deaths in females, which is uncommon among studies in the nuclear sector.
A prominent factor is the healthy worker effect, indicating that disease prevention and health promotion measures provided by occupational health, together with access to health services, reduced mortality from cancer and other diseases.
SMR showed lower mortality from cancer and all causes among exposed workers and among those monitored for gamma and X radiation, which can be attributed to the quality of protective measures in the workplace and health control of these workers. These results suggest the occurrence of the healthy worker effect and the benefits arising from good practices in health and safety at work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation Health risks from exposure to low levels of ionizing radiation: BEIR VII phase 2Washington National Academies 200610.17226/1134025077203 · doi ↗ · pubmed ↗
- 2Mc Geoghegan D Binks K The mortality and cancer morbidity experience of employees at the Chapelcross plant of British Nuclear Fuels plc, 1955-95J Radiol Prot 200121322125010.1088/0952-4746/21/3/30211594650 · doi ↗ · pubmed ↗
- 3Mc Geoghegan D Binks K The mortality and cancer morbidity experience of workers at the Capenhurst uranium enrichment facility 1946-95J Radiol Prot 200020438140110.1088/0952-4746/20/4/30311140711 · doi ↗ · pubmed ↗
- 4Smith PG Douglas AJ Mortality of workers at the Sellafield plant of British Nuclear Fuels Br Med J (Clin Res Ed.)1986293655184585410.1136/bmj.293.6551.845PMC 13416353094683 · doi ↗ · pubmed ↗
- 5Beral V Fraser P Carpenter L Booth M Brown A Rose G Mortality of employees of the Atomic Weapons Establishment, 1951-82BMJ 1988297665175777010.1136/bmj.297.6651.7573142540 PMC 1834407 · doi ↗ · pubmed ↗
- 6Wing S Shy CM Wood JL Wolf S Cragle DL Frome EL Mortality among workers at Oak Ridge National Laboratory: evidence of radiation effects in follow-up through 1984 JAMA 199126511139714021999879 · pubmed ↗
- 7Fraser P Carpenter L Maconochie N Higgins C Booth M Beral V Cancer mortality and morbidity in employees of the United Kingdom Atomic Energy Authority, 1946-86BMJ 199367361562410.1038/bjc.1993.113PMC 19682778439513 · doi ↗ · pubmed ↗
- 8Beral V Inskip H Fraser P Booth M Coleman D Rose G Mortality of employees of the United Kingdom Atomic Energy Authority, 1946–1979 Br Med J (Clin Res Ed.)1985291649344044710.1136/bmj.291.6493.440PMC 14163163926232 · doi ↗ · pubmed ↗