An epidermal growth factor receptor compound mutation of L858R with S768I in advanced non-small-cell lung cancer: a case report
Sara Boukansa, Ismail Mouhrach, Fatima El Agy, Laila Bouguenouch, Mounia Serraj, Bouchra Amara, Yassine Ouadnouni, Mohamed Smahi, Badreeddine Alami, Nawfel Mellas, Zineb Benbrahim, Hinde El Fatemi

TL;DR
A patient with a rare double EGFR mutation in lung cancer showed long-term survival with afatinib treatment.
Contribution
Demonstrates the potential efficacy of EGFR-TKIs in rare complex EGFR mutations through a case report.
Findings
Patient with L858R/S768I EGFR mutation had 51 months of overall survival on afatinib.
Median progression-free survival exceeded 39 months in this case.
Highlights therapeutic potential of EGFR-TKIs for complex mutations.
Abstract
In the current treatment landscape for non-small cell lung cancers, epidermal growth factor receptor-tyrosine kinase inhibitors have emerged as a well-established treatment option for patients with advanced or metastatic disease. This is particularly true for those with commonly occurring epidermal growth factor receptor mutations. However, the therapeutic efficacy of these agents for so-called rare epidermal growth factor receptor mutations, and in particular those characterized by a high degree of complexity, such as double mutations, remains a subject of clinical uncertainty. In this context, we present the case of a 64-year-old man of Moroccan descent, a lifelong non-smoker, diagnosed with metastatic non-small cell lung cancer characterized by a complex epidermal growth factor receptor mutation encompassing L858R and S768I. The patient subsequently underwent afatinib-based…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
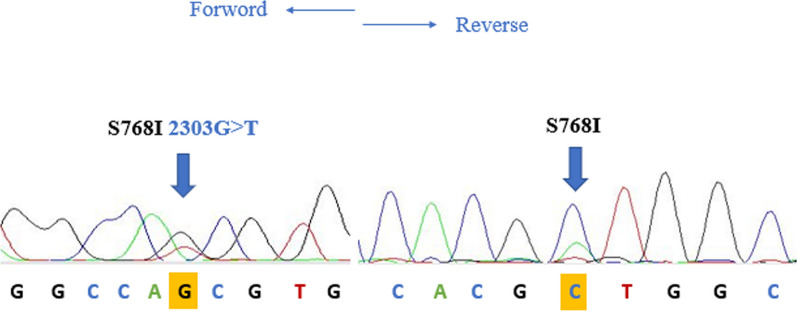 Figure 1
Figure 1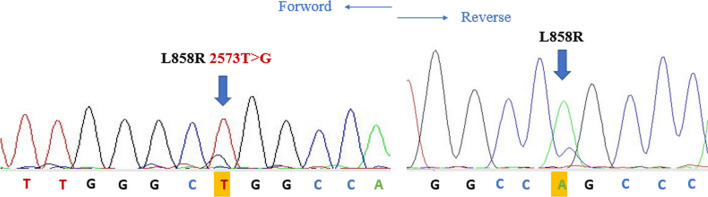 Figure 2
Figure 2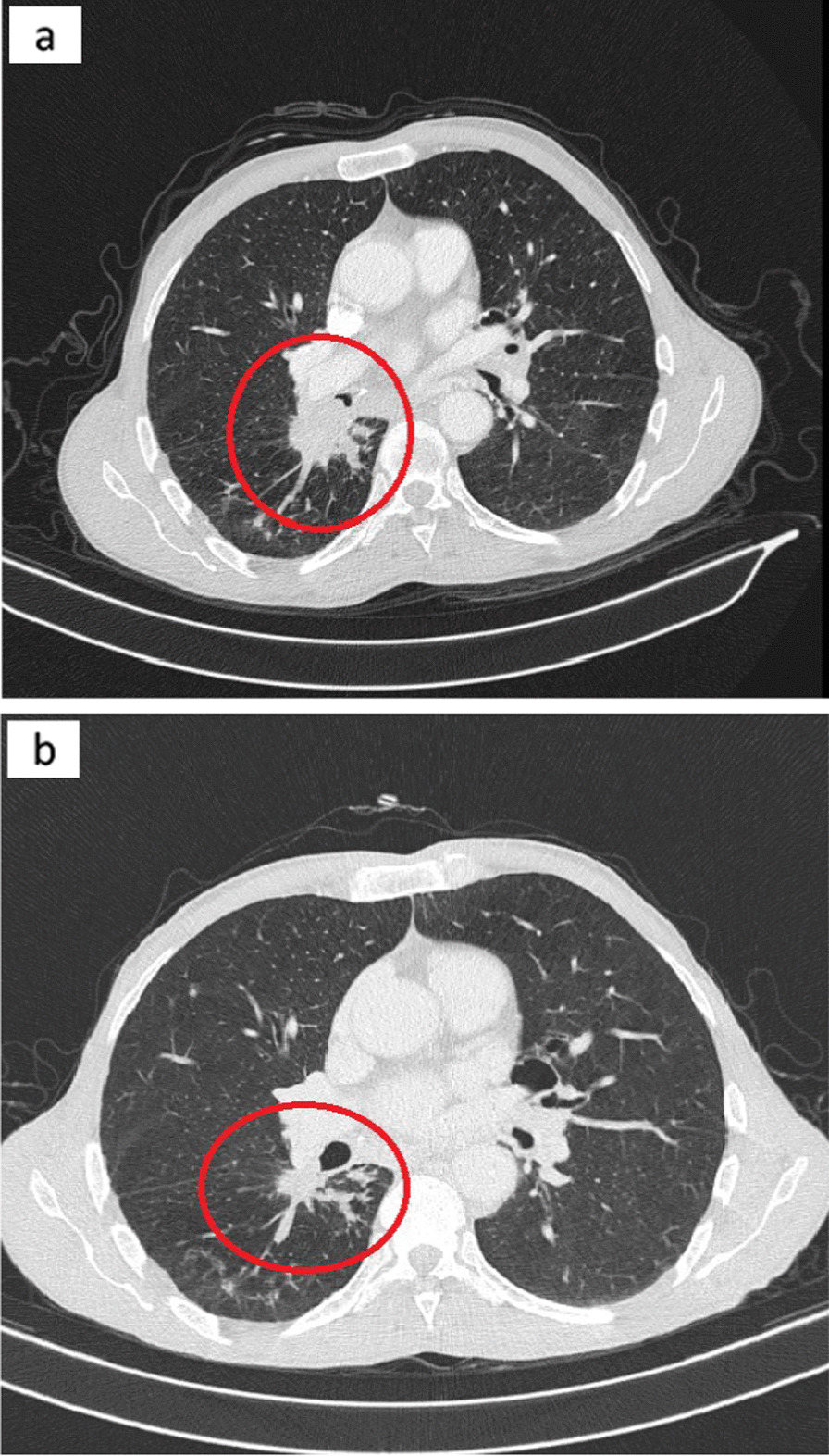 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Cancer therapeutics and mechanisms · Colorectal Cancer Treatments and Studies
Introduction
Lung cancer is ranked as the most common cause of cancer-related death worldwide. Non-small cell lung cancers (NSCLCs) are currently the most prevalent form, accounting for approximately 80–85% of all lung cancer cases [1]. The majority of patients diagnosed with lung adenocarcinoma are often in advanced stages (stage IV) and derive modest benefit from nonselective cytotoxic chemotherapy [2]. However, the discovery of epidermal growth factor receptor (EGFR) mutations in 2004 has revolutionized the treatment of these patients [3]. Patients with NSCLC with an activating mutation within the epidermal growth factor receptor (EGFR) exhibit a dramatic response to EGFR-tyrosine kinase inhibitors (EGFR-TKIs) [4]. 80–90% of activated EGFR mutations are normally located in exon 19 deletions and L858R substitution in exon 21 [5]. in addition to these known common mutations, there are other remaining rare mutations whose predictive value is still unclear. Some of these are expressed by the coexistence of two common or rare and common mutations together on different exons in the EGFR gene, which are called “compound mutations.” The clinical response of patients with compound EGFR mutations to EGFR‑TKIs remains unclear. Several studies indicate that individuals with compound EGFR mutations may show reduced responsiveness to TKI therapies compared with those with single mutations [6–9]. Additionally, different treatment efficacies have been associated with different types of EGFR compound mutations [10, 11]. While first-generation EGFR-TKIs could be a useful treatment option, recent studies suggest considering afatinib and osimertinib for patients with compound EGFR mutations, depending on their specific cases [12, 13]^.^ These alternative therapies require further investigation to understand their effectiveness and optimal application in the specific context of patients with compound EGFR mutations.
We present a case report of a patient with common L858R (exon 21) and rare S768I (exon 20) mutations treated with afatinib.
Case report
In April 2017, a 64-year-old male of Moroccan descent, a lifelong nonsmoker with no significant medical or family history, presented with a persistent productive cough accompanied by scant hemoptysis and grade 2 dyspnea, which had been ongoing for 3 months. These symptoms were part of a broader clinical picture marked by a progressive decline in his general health status. A comprehensive evaluation, including a chest computed tomography (CT) scan, unveiled a primary tumor mass measuring 95 mm × 69 mm × 66 mm in the lower right lobe of the lung. Additionally, the imaging indicated the presence of lymphangitic carcinomatosis and lymph node involvement on both the ipsilateral and contralateral sides of the thorax, classifying the disease as T4N3M0 according to the TNM staging system (stage IIIc). To establish a definitive histological diagnosis, a transbronchial lung biopsy was performed on the affected right lobe. Subsequently, formalin-fixed paraffin-embedded tissue sections, measuring 4 μm in thickness, were subjected to hematoxylin and eosin saffron (HES) staining, revealing the presence of acinar lung adenocarcinoma. Immunohistochemical staining confirmed the diagnosis, as it exhibited positivity for cytokeratin 7 (CK7) and transcription factor-1 protein (TTF1). The initial therapeutic approach involved first-line chemotherapy, combining cisplatin at a dosage of 75 mg/m^2^ with navelbine at 25 mg/m^2^. Early assessment via CT imaging, performed after the treatment period from 23/11/2017 to 22/12/2017, demonstrated a notable regression in tumor size (from 66 mm × 69 mm × 95 mm to 35 mm × 35 mm × 60 mm) following the initial courses of chemotherapy. However, subsequent CT scans after two cycles of treatment indicated the presence of lung and lymph node metastases, prompting a shift toward palliative chemotherapy. Following this transition, genetic profiling was conducted at the Department of Biomolecular CHU Hassan II to guide personalized therapeutic decisions. DNA extraction was performed from the available histological specimen using the QIAamp DNA FFPE Tissue Kit (Invitrogen), following the manufacturer’s protocols. Genetic analysis employed reverse transcription-polymerase chain reaction (RT-PCR) technology, with the quantitative PCR analysis utilizing the therascreen EGFR RGQ PCR Kit. This analysis revealed the presence of an activating co-mutant involving the L858R mutation in exon 21 (c.2573T>G) and the S768I mutation in exon 20 (c.2303G>T, p.S768I). These mutations were subsequently confirmed through SANGER sequencing (Figs. 1, 2). In April 2018, the patient was administered oral afatinib at a daily dose of 40 mg. A follow-up CT scan conducted 3 months post-initiation of afatinib treatment demonstrated a dramatic reduction in tumor size (Fig. 3), accompanied by a significant amelioration of symptoms such as dyspnea, cough, and hemoptysis. Remarkably, the patient exhibited excellent tolerance to afatinib therapy, facilitating a consistent improvement and a relatively slow progression rate of the disease. This response led to a period of disease stabilization until the detection of bone metastases in December 2020. Subsequent months witnessed a state of relative stability in the progression of the primary tumor and associated nodules, until the emergence of a brain metastasis in April 2021. At this juncture, deliberations surrounding potential stereotactic radiotherapy were undertaken; however, the patient opted against surgical intervention. Regrettably, as of the latest available update on 15 August 2022, we have received information confirming the patient’s death.Fig. 1. Electropherogram traces of exon 20 S768I positive mutation confirmed by Sanger sequencingFig. 2Electropherogram traces of exon 21 L858R positive mutation confirmed by Sanger sequencingFig. 3CT scan results showing the primary tumor in the right lower lobe of the lung before treatment (a), and the dramatic response 3 months post-afatinib treatment (b). The red circle represents the primary tumor before and after treatment
Discussion
The management of non-small cell lung cancer (NSCLC) has evolved significantly with a focus on identifying driver mutations, such as EGFR and ALK-EML4, within tumor samples to guide personalized treatment strategies. The epidermal growth factor receptor (EGFR) is a member of the ErbB family of receptor tyrosine kinases (RTK) [14]. In NSCLC, mutations in the intracellular region of EGFR have been observed in a range of 43–89% of cases [15]. Among these mutations, more than 90% are accounted for by EGFR TKI-sensitizing mutations, primarily involving exon 19 deletions and the exon 21 L858R substitution [16]. Notably, patients with tumors bearing these activating mutations typically exhibit substantial clinical and radiographic responses to EGFR tyrosine kinase inhibitors (TKIs) such as gefitinib, erlotinib, and afatinib [16].
In contrast, the S768I exon 20 substitution (serine replacing isoleucine at codon 768) is described as a rare mutation, representing ~ 1% of cases [17]. The rarity of S768I mutations has posed challenges in defining their role as molecular predictors of TKI response. However, recent studies have shed light on the clinical significance of S768I mutations in lung adenocarcinoma, demonstrating favorable responses to TKIs [18, 19].
Even rarer than the S768I substitution are compound mutations, which encompass not only single exon mutations, but also combinations of double mutations occurring across different exons of the EGFR gene. These compound mutations often involve a mix of common and rare mutations (Table 1). In our specific case, the compound mutation was identified as a co-occurrence of L858R exon 21 substitution and the exon 20 S768I mutation. This observation may be attributed to the genetic heterogeneity within EGFR mutation-positive non-small-cell lung cancer, leading to clonal evolution and the emergence of diverse molecular characteristics at the cellular level [20].Table 1. Clinical case summaries—insights from the literatureCase no.Age, yearsSexMutation typeTreatmentResponseOur case64MaleL858R + S768IAfatinibGRSvaton et al. [31]63FemaleG719X + S768IGefitinibGRMasahiro et al. [32]72FemaleG719X + S768IAfatinibGRYan et al. [33]62Femaledel 2239_2248 + insC + L858RErlotinibPDToshiki et al. [34]72MaleG719X + S768IOsimertinibGRSimionato et al. [35]69FemaleG719A + V769MOsimertinibGRJuan et al. [36]43Female19-Del + T790MChemotherapyPDHe et al. [37]64FemaleG724S + R776HAfatinibGRBao et al. [38]36MaleR670W + H835L + L833VAfatinib + osimertinibGRYang et al. [39]N/AMaleH773L + V774MOsimertinibGRLi et al. [40]53FemaleL833V + H835LAumolertinibGRN/A not available, GR good response, PD progressive disease
Recent studies have highlighted the complexity and heterogeneity of *EGFR *mutations in NSCLC tumors [20], raising questions about their implications for treatment efficacy. The frequency and response patterns of patients harboring complex mutations remain incompletely defined, primarily due to the limited number of different complex mutations. Generally, compound mutations involving frequent mutations demonstrate similar or improved sensitivity to EGFR-TKI therapy [9], and complex mutations, which combine frequent and sparse mutations (non-resistant), tend to exhibit comparable clinical responses to those associated with frequent mutations alone [21].
The L858R substitution emerges as the most prevalent mutation found in conjunction with other rare mutations [21, 22]. Several studies have emphasized the importance of specific compound mutations. For instance, patients with concomitant L858R and V834L or G873E mutations have demonstrated sensitivity to EGFR-TKIs comparable to those with single L858R mutations [22]. Additionally, the concomitant del-19 + L858R mutation has been associated with a more favorable clinical response to EGFR-TKIs [5].
However, the presence of compound mutations, such as L858R and S768I, in patients with NSCLC presents distinct clinical challenges. Multiple studies have consistently shown that patients with compound EGFR mutations tend to exhibit reduced sensitivity to TKI therapies compared with those with single EGFR mutations [6, 7, 23, 24]. Furthermore, emerging evidence suggests that the specific types of compound EGFR mutations may be linked to different treatment response patterns [11].
Moreover, the S768I mutation has been associated with resistance to first-generation EGFR-TKIs, such as gefitinib and erlotinib, which are commonly used for EGFR-mutated NSCLC [25–27]. In response to the intrinsic resistance displayed by the S768I mutation toward first-generation EGFR-TKIs, extensive efforts have been dedicated to exploring alternative therapeutic approaches. Second- and third-generation TKIs, including afatinib and osimertinib, have emerged as promising options, exhibiting notable efficacy against the S768I mutation [25, 28–30]. These agents demonstrate a selective binding affinity for the mutant EGFR, effectively surmounting the resistance mechanisms associated with the S768I alteration, thus providing a viable treatment avenue for patients harboring this specific co-mutation.
In the present report, we investigate the efficacy of afatinib EGFR-TKI in the context of a 64-year-old Moroccan male patient who was a lifelong nonsmoker and presented with concomitant L858R and S768I mutations. Remarkably, this patient exhibited an overall survival (OS) of 51 months and a median progression-free survival (PFS) exceeding 39 months following afatinib therapy. These outcomes significantly surpass those reported by Ling et al. [21], who observed a PFS of 6 months and an OS of 6.5 months in a 70-year-old male smoker (20 pack-years) with L858R + S768I complex mutation treated with gefitinib. This intriguing disparity suggests that the S768I + L858R co-mutation may enhance the interaction between EGFR and afatinib compared with gefitinib, resulting in a remarkable clinical response to afatinib TKIs.
Conclusion
EGFR mutation heterogeneity encompasses compound mutations, constituting a distinctive subgroup of patients with NSCLC with varying responses to EGFR tyrosine kinase inhibitors. The present report delineates a rare case of acinar lung adenocarcinoma harboring an L858R point mutation in exon 21 and a compound S768I EGFR substitution mutation. Following treatment with afatinib, this patient demonstrated a highly favorable therapeutic response exceeding 38 months. These findings underscore the complexity of EGFR mutations in NSCLC and emphasize the need for tailored treatment strategies to address the diversity of mutational profiles encountered in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D’Addario G Früh M Reck M Baumann P Klepetko W Felip E Metastatic non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment, and followup Ann Oncol 201021 Suppl. 511611910.1093/annonc/mdq 18920555059 · doi ↗ · pubmed ↗
- 2Sandler A Gray R Perry MC Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer N Engl J Med 2006355242542255010.1056/NEJ Moa 06188417167137 · doi ↗ · pubmed ↗
- 3Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350(21):2129-2139. doi:10.1056/NEJMOA 04093810.1056/NEJ Moa 04093815118073 · doi ↗ · pubmed ↗
- 4Witta SE Jotte RM Konduri K Randomized phase II trial of erlotinib with and without entinostat in patients with advanced non-small-cell lung cancer who progressed on prior chemotherapy J Clin Oncol 201230182248225510.1200/JCO.2011.38.941122508830 PMC 4798782 · doi ↗ · pubmed ↗
- 5Keam B Kim DW Park JH Rare and complex mutations of epidermal growth factor receptor, and efficacy of tyrosine kinase inhibitor in patients with non-small cell lung cancer Int J Clin Oncol 201419459460010.1007/S 10147-013-0602-123912954 · doi ↗ · pubmed ↗
- 6Kauffmann-Guerrero D Huber RM Reu SNSCLC patients harbouring rare or complex EGFR mutations are more often smokers and might not benefit from first-line tyrosine kinase inhibitor therapy Respiration 201895316917610.1159/00048417529190621 · doi ↗ · pubmed ↗
- 7Tam IYS Leung ELH Tin VPC Double EGFR mutants containing rare EGFR mutant types show reduced in vitro response to gefitinib compared with common activating missense mutations Mol Cancer Ther 2009882142215110.1158/1535-7163.MCT-08-121919671738 · doi ↗ · pubmed ↗
- 8Kobayashi S Canepa HM Bailey AS Compound EGFR mutations and response to EGFR tyrosine kinase inhibitors J Thorac Oncol 20138111812210.1097/JTO.0B 013E 3182781 E 35PMC 353104323242437 · doi ↗ · pubmed ↗