Surgical release of the chest wall skin and fascia for sclerodermatous graft versus host disease causing restrictive lung disease: A case report
Mitchell Nash, Kim Cartwright, Rebecca Nguyen, Peter Middleton, Peter Maitz

TL;DR
A patient with severe skin GVHD causing lung issues had surgery to improve chest expansion and quality of life, with mixed long-term results.
Contribution
This case report explores surgical release of chest wall skin and fascia as a treatment for sclerodermatous GVHD-related restrictive lung disease.
Findings
Surgical release with split skin grafting improved the patient's lung function and quality of life subjectively.
The patient requested a second surgical procedure, indicating perceived benefit.
Despite initial improvement, lung function continued to decline over time.
Abstract
Graft versus host disease (GVHD) remains a significant source of morbidity and mortality in the setting of allogeneic stem cell transplantation. Skin involvement is reported to be as high as 70–95 % in this group with GVHD and the severity of the involvement varies widely. Surgical management of complications of severe cutaneous GVHD is uncommon and is rarely mentioned as a treatment option. We present a case of severe sclerodermatous skin changes restricting chest expansion and exercise tolerance to the point of limiting basic activities of daily life. A 54-year-old male presents with severe restrictive lung disease from sclerodermatous graft versus host disease (GVHD) after stem cell transplant for Chronic Myeloid Leukaemia (CML). He experienced limited symptomatic relief from maximal medical therapy and photochemotherapy, and subsequently underwent a skin release and split skin…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
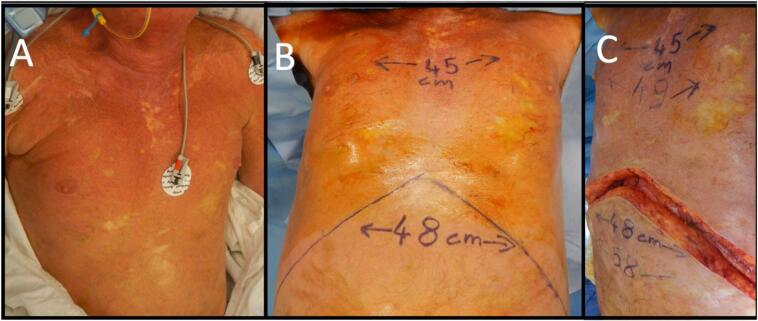 Figure 1
Figure 1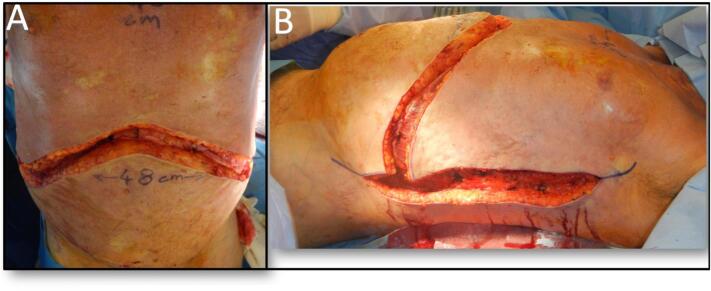 Figure 2
Figure 2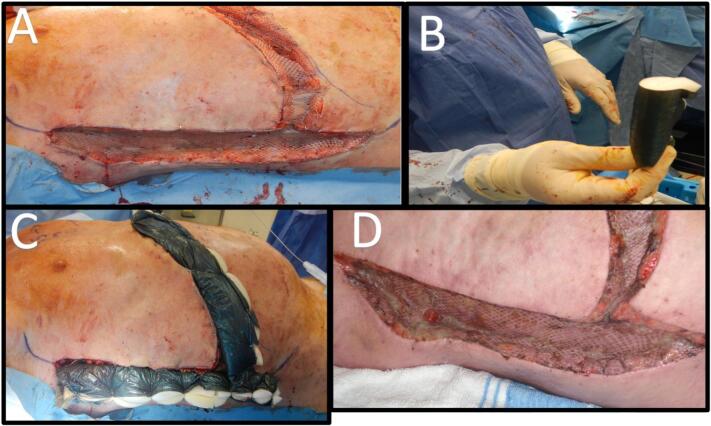 Figure 3
Figure 3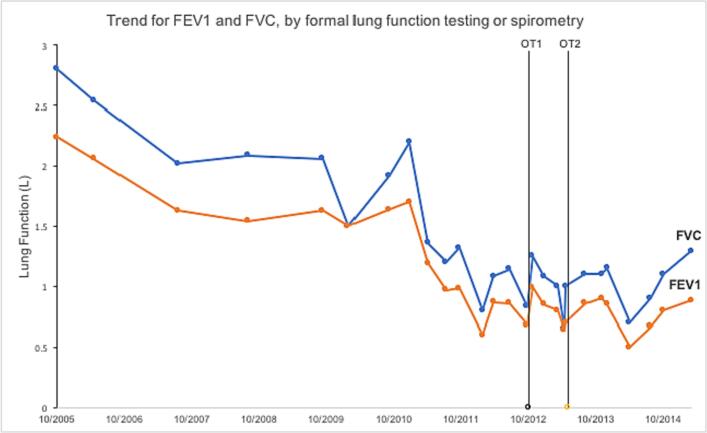 Figure 4
Figure 4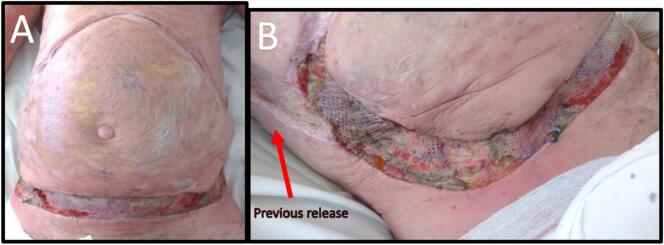 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHematopoietic Stem Cell Transplantation · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Systemic Sclerosis and Related Diseases
Introduction
1
Graft versus host disease (GVHD) remains a significant source of morbidity and mortality in the setting of allogeneic stem cell transplantation [1]. Skin involvement is reported to be as high as 70–95 % in this group with GVHD and the severity of the involvement varies widely [2,3]. Severe skin involvement and the resultant scarring can lead to restrictive lung disease. Surgical management of complications of severe cutaneous GVHD is uncommon and is rarely mentioned as a treatment option [1,4,5]. Surgical management of cutaneous GVHD is controversial with conflicting evidence from a scarce number of Level IV studies [[6], [7], [8]]. This work has been reported in line with the scare criteria [9].
In De Novo Scleroderma, skin grafts from clinically normal skin to a sclerodermatous bed become sclerodermatous. This suggests that the skin changes are due to the underlying disrupted vascular bed with activated fibroblasts, otherwise a split skin graft taken from a normal donor site would heal as a normal skin graft, rather than take on the characteristics of sclerodermatous skin. In the reverse scenario, when sclerodermatous skin is grafted onto a normal bed, it remains sclerodermatous, suggesting that the skin changes are irreversible. Otherwise, improvement in skin quality would be expected of sclerodermatous skin grafted onto a normal bed. Sclerodermatous skin used as a split skin graft does take though and can allow closure of traumatic or chronic wounds as well as surgical wounds from skin release.
Escharotomies have long been a mainstay of treatment for circumferential deep burns which cause a torniquet effect and result in poor perfusion to the affected limb [10,11]. Chest escharotomies have been used to improve ventilation in patients with impaired chest expansion from full thickness chest burns [12].
Case presentation
2
A 54-year-old male presents with severe restrictive lung disease from sclerodermatous GVHD following matched sibling myeloablative allogenic stem cell transplant for Chronic Myeloid Leukaemia (CML) in 2001. This was conducted prior to subsidised tyrosine kinase inhibitors being available in Australia to patients with CML in chronic phase. He remained in remission following his allograft.
His other general medical history included obstructive sleep apnea on home CPAP, hypertension, gastroesophageal reflux, and osteoporosis. Pre-operative transthoracic echocardiogram was notable for mild-to-moderate impairment of left ventricular systolic function without significant valvular abnormalities. His medications at time of surgery are summarized in Table 1.Table 1. Regular medications at time of surgery.Table 1. Tacrolimus 3 mg mane/2 mg noctePregabalin 225 mg BDPrednisone 20 mg dailyPantoprazole 40 mg nocteTrimethoprim/sulfamethoxazole 160/800 mg BD twice weeklyCitalopram 10 mg nocteAzithromycin 250 mg BDFolic acid 5 mg dailySeretide (fluticasone/salmeterol) 250/25 μg 2 puffs BDMagnesium aspartate 1500 mg BDFelodipine 2.5 mg maneCholecalciferol 1000 units dailyTramadol 50 mg TDSIntravenous gammoglobulin 30 g monthlyOxycontin 5 mg BDZoledronic acid 5 mg yearly
He developed grade 2–3 skin, gastrointestinal and hepatic acute GVHD which settled with high dose steroids and cyclosporin. Despite continued immunosuppression, he developed chronic extensive GVHD from approximately twelve months post-transplant, initially involving his liver, followed by inflammatory immune myositis, mono-neuritis multiplex, chronic inflammatory demyelinating polyneuropathy, with left phrenic nerve palsy and left hemidiaphragm paralysis. Sclerodermatous skin involvement was first noted three and a half years post-transplant.
Immunosuppressive therapies included steroids, cyclosporin, sirolimus, tacrolimus, rituximab, and romidepsin, with monthly intravenous gammaglobulin. He was managed with psoralen-ultraviolet A (PUVA) photochemotherapy, and due to ongoing deterioration, was subsequently commenced on extra-corporeal photopheresis, on twice monthly maintenance therapy prior to surgery.
Despite these treatments, he experienced symptomatic and clinical deterioration, with declining lung function tests, difficulty swallowing, weight loss and abdominal pain due to the constriction of his sclerodermatous GVHD. In the 18 months prior to surgery, he had 6 separate hospital admissions for acute-on-chronic respiratory failure in the setting of his interstitial pulmonary GVHD and CO_2_ retention; 3 of these admissions required high dependency unit (HDU) for non-invasive ventilation (NIV). Formal lung function tests performed 3.5 months pre-operatively were consistent with severe restrictive lung disease, with FEV1 0.86 L (23 % predicted), FVC 1.14 L (23 % predicted), and FEV1/FVC of 75 %.
He was referred to a Burns Unit, for consideration of skin and soft tissue release with split skin grafting, to possibly improve his restrictive lung disease. Although there was no clear precedent to this treatment, the patient was willing to undergo this surgery as his quality of his life had become severely limited by his disease, particularly in the preceding twelve months.
He underwent elective surgery on the 15th of October 2012 carried out by the senior author. He had an uncomplicated peri-operative stay, including a planned 24 h in intensive care post-operatively, intubated and ventilated. He was noted to a have a grade III larynx requiring two-operator intubation with video-laryngoscope support and a fibre-optic scope.
At the time of surgery, he was noted to have widespread abnormal soft tissue (Fig. 1A) with extensive thick scarring (fascial-like bands) from the skin surface extending deep to his intercostal muscles. The pattern of escharotomy was anterior chest subcostal margin and mid-axillary (Fig. 2). The escharotomies were released from skin to deep facia, exposing serratus anterior, intercostals, external oblique and rectus muscles, using scalpel and diathermy. Foam rolled into a cylinder with Acticoat [Smith & Nephew] stapled on was used to deliver some compression on the vertical walls of the wound (Fig. 3B/C). Due to the location of the escharotomies, no postoperative splinting was feasible, and standard chest physiotherapy was performed. A sample of this tissue was sent for histopathology, reported as non-specific scar tissue and fibrosis. On table, he had a tidal volume increase of 100 mL, from 360 to 460 mL (PEEP 6cmH2O, Peak Airway pressure 21cmH2O). His chest transverse measurement (from midaxillary line) increased from 45 to 49 cm, and his abdominal girth increased from 48 to 58 cm (Fig. 1C).Fig. 1A: Skin appearance immediately pre-operatively.B: Chest and abdominal measurements prior to surgery.C: Measured increase on table post release and grafting.Fig. 1. Fig. 2Depth of surgical release, through deep fascia exposing underlying musculature.A Subcostal.B Mid-axillary.Fig. 2. Fig. 3A: Intra-op post graft inset.B: Acticoat foam tube dressingC: Dressing in situ.D: Early (day 10) graft result.Fig. 3
Post-operatively, the patient described a subjective improvement in exercise tolerance and was able to return to enjoying lawn bowls. His informal spirometry improved significantly, from an FEV1 of 0.68 L, and FVC of 0.83 L pre-operatively, to 0.99 L and 1.25 L respectively post-operatively. Unfortunately, he did not undergo formal lung function testing immediately prior to surgery to allow for comparison. 9 months post-operatively, his lung function on spirometry had continued to regress, with an FEV1 of 0.7 L and FVC of 0.9 L, which was marginally better than his spirometry 4 months pre-operatively (Fig. 4).Fig. 4. Trend for Forced Expiratory Volume-one second (FEV1) and Forced Vital Capacity (FVC), as measured by formal lung function testing or spirometry, over time, with dates marked for escharotomy and skin grafting of chest (OT1) and abdominal (OT2) wall.Fig. 4
The patient requested further skin release, and in May 2013 underwent an inferior transverse (supra-pubic) and longitudinal (meeting existing mid-axillary graft) abdominal skin release and split skin grafting (Fig. 5). His abdominal expansion increased 10 cm transversely and 4 cm longitudinally, with an immediate tidal volume increase of 50 mL. Informal spirometry showed a modest and transient improvement in FEV1 and FVC, from 0.64 L and 0.65 L pre-operatively, to 0.7 L and 1.0 L respectively post-operatively (Fig. 4). His spirometry results appeared to subsequently stabilise, although he was commenced on methotrexate in March 2014, which may potentially confound the benefits of his surgeries.Fig. 5A: Further 10 cm transverse and 4 cm vertical skin release on table resulting in an increase of 50mls tidal volume.B: Note the maintained width of mature grafts from previous release.Fig. 5
In support for the benefit surgical release, in his 9 admissions to hospital post-surgery, he did not require HDU for NIV, which is in contrast to the 18 months prior to his surgery where 3 out of 6 admissions required NIV. However, there was a clear downward trend of his lung diffusing capacity over time, reflecting the clear progression of his interstitial lung disease and the resulting decrease in function. The patient unfortunately passed away in December 2015, following a sudden cardiac arrest. An autopsy was not carried out and his death was presumed due to progression of his disease.
Discussion
3
Beredjiklian released joint contractures in the setting of cutaneous GVHD in 3 patients [8]. He found the released joints showed some initial improvement but relapsed to their pre-surgical range of motion. These releases involved a capsule release with or without muscle or tendon division/lengthening. No comment is made by the author specifying the incision or any skin lengthening procedures such as z plasties.
In contrast, a case report by Kim et al. released bilateral cubital fossa, axillae and shoulder contractures with multiple Y—V plasties. The underlying joints were normal and the improved range of motion was maintained at 9 months post-operatively [7].
Escharotomies of the chest are a standard management of full thickness burns restricting ventilation, as they may help relieve respiratory and hemodynamic dysfunctions [12]. Post-burn scar contractures which restrict movement are routinely released with split skin grafting with improved range of motion in combination with physiotherapy and splinting [12,13]. Thus, the premise that releasing thick chest wall scarring, with skin grafts should improve lung function and exercise tolerence in this case of cutaneous GVHD. However, despite initial improvement in hand-held spirometry results, formal lung function tests did not show any lasting objective improvement. A potentional confounder of the outcome of this surgery is ongoing progression of his interstitial pulmonary GVHD which had detoriated with time, in addition to the progression of his cutaneous GVHD.
The skin release objectively and subjectively improved the patient's function, given the objective improvement in lung function tests and the patient's request for further release surgery. This demonstrated that for this patient at least, they felt their quality of life was improved by the intervention and justified the hospital stay, pain and high-risk anaesthetic.
The authors conclude that there was no objective, sustained improvement in his lung function, although the decline in his lung function stabilised. Delineating between ongoing scarring and contraction of the split skin grafts (reducing their effect) versus ongoing disease progression is more difficult. Given the rarity of this presentation, we would suggest that the decision for surgery is best decided by a multi-disciplinary team approach in a case-by-case basis. Thus, surgical release and split skin grafting requires further evaluation to establish a clear role in the treatment of restrictive lung disease due to cutaneous GVHD. In this case escharotomy and skin grafting was a successful option to improve the quality of life of a patient and provide relief, at least temporarily, of the symptoms of restrictive lung disease. With appropriate informed consent, it is a potential treatment option for patients with this rare severe disease.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
SYDNEY LOCAL HEALTH DISTRICT - CRGH.
HUMAN RESEARCH ETHICS COMMITTEE.
Approval No. CH 62/6/2015-215.
Funding
No financial support or grants were received for this work.
Author contribution
Prof Maitz – study concept and design, review of manuscript, Snr Author/Primary Surgeon.
Dr. Nash - Writing of manuscript (primary author)/data collection, assistant surgeon.
Prof Cartwright: editing and rewriting of manuscript, data analysis.
Dr. Nguyen: editing/review of manuscript, data collection, research.
Prof. Middleton: review of manuscript, data collection.
Guarantor
Prof Maitz.
Dr. Kim Cartwright.
Research registration number
N/A.
Conflict of interest statement
Nil.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Komanduri K.V.Couriel D.Champlin R.E.Graft-versus-host disease after allogeneic stem cell transplantation: evolving concepts and novel therapies including photopheresis Biol. Blood Marrow Transplant.121Jan 20061610.1016/j.bbmt.2005.11.00316399595 · doi ↗ · pubmed ↗
- 2Hymes S.R.Sousa I.C.Herskovitz I.Alousi A.M.Cowen E.W.Skin signs of graft versus host disease J. Am. Dermatol.6642013535.e 1535.e 16(Elsevier)
- 3Sbano P.Rubegni P.De Aloe G.B.Guidi S.Fimiani M.Extracorporeal photochemotherapy for treatment of fasciitis in chronic graft-versus-host disease Bone Marrow Transplant.338Jan 26 20048698701474319010.1038/sj.bmt.1704436 · doi ↗ · pubmed ↗
- 4PA.R.AD.MH.L.PS.Z.YL.Cowen Edward W.Rippled skin, fasciitis, and joint contractures J. Am. Dermatol.596Dec 1 200810701074(American Academy of Dermatology, Inc.)10.1016/j.jaad.2008.08.023PMC 259193119022104 · doi ↗ · pubmed ↗
- 5Weitz M.BS.MJ.BD.Extracorporeal Photopheresis Versus Alternative Treatment for Chronic Graft-versus-host Disease after Haematopoietic Stem Cell Transplantation in Paediatric Patients (Review)Jan 1, 201412610.1002/14651858.CD 009898.pub 224569961 · doi ↗ · pubmed ↗
- 6Burns P.B.Rohrich R.J.Chung K.C.The levels of evidence and their role in evidence-based medicine 1281 Jul 201130531010.1097/PRS.0b 013e 318219 c 171PMC 312465221701348 · doi ↗ · pubmed ↗
- 7Kim J.B.Liakopoulou E.Watson J.S.Successful treatment of refractory joint contractures caused by sclerodermatous graft versus host disease J. Plast. Reconstr. Aesthet. Surg.6110 Oct 200812351238(Elsevier)1750995510.1016/j.bjps.2007.03.036 · doi ↗ · pubmed ↗
- 8Beredjiklian P.K.Drummond D.S.Dormans J.P.Davidson R.S.Brock G.T.August C.Orthopaedic manifestations of chronic graft-versus-host disease J. Pediatr. Orthop.185Sep 1998572575974640210.1097/00004694-199809000-00002 · doi ↗ · pubmed ↗