An Unusual Case of Severe Pre-eclampsia and Pulmonary Edema Following Single Fetal Demise in an In Vitro Fertilization (IVF)-Conceived Twin Gestation: A Twisted Tale of Twins
Smruti A Mapari, Deepti Shrivastava, Gautam N Bedi, Paschyanti R Kasat

TL;DR
This case report describes a rare instance where a twin pregnancy led to severe health issues after one fetus died, highlighting a gap in obstetric research.
Contribution
The novelty lies in documenting a unique case of pre-eclampsia and pulmonary edema following fetal demise in a twin gestation, with limited prior literature.
Findings
A single fetal death at 24 weeks led to severe maternal hypertension and pulmonary edema.
No exact matches were found in peer-reviewed literature for this specific clinical presentation.
The case highlights a gap in understanding complications following fetal demise in twin pregnancies.
Abstract
There has been a notable rise in instances of multiple-fetus pregnancies over the last decade, attributed to the widespread adoption of assisted reproductive technologies. Moreover, these pregnancies have been associated with the use of drugs to induce ovulation. While some cases involve the loss of one twin with minimal consequences for the surviving twin, the demise of a fetus after the first trimester, especially beyond three months into the pregnancy, can significantly impact the health of both the mother and the surviving fetus. Unfavorable outcomes linked to the loss of one twin after the first trimester include impaired physical growth of the surviving fetus, preterm delivery, neurological abnormalities, and, in certain instances, the death of the surviving twin. This report provides a detailed account of a specific case involving twin pregnancies where a single fetal death…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1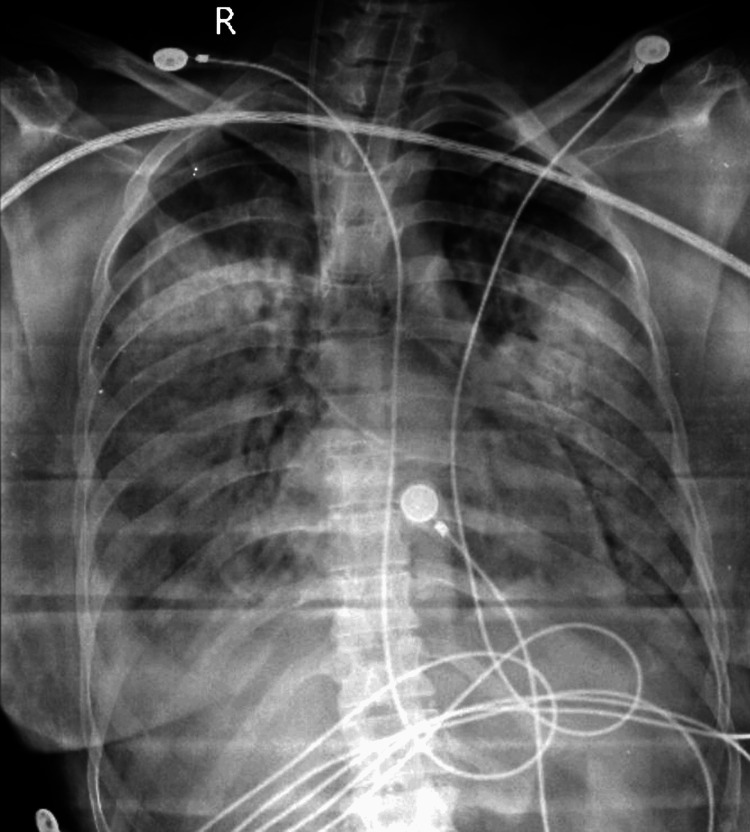 Figure 2
Figure 2 Figure 3
Figure 3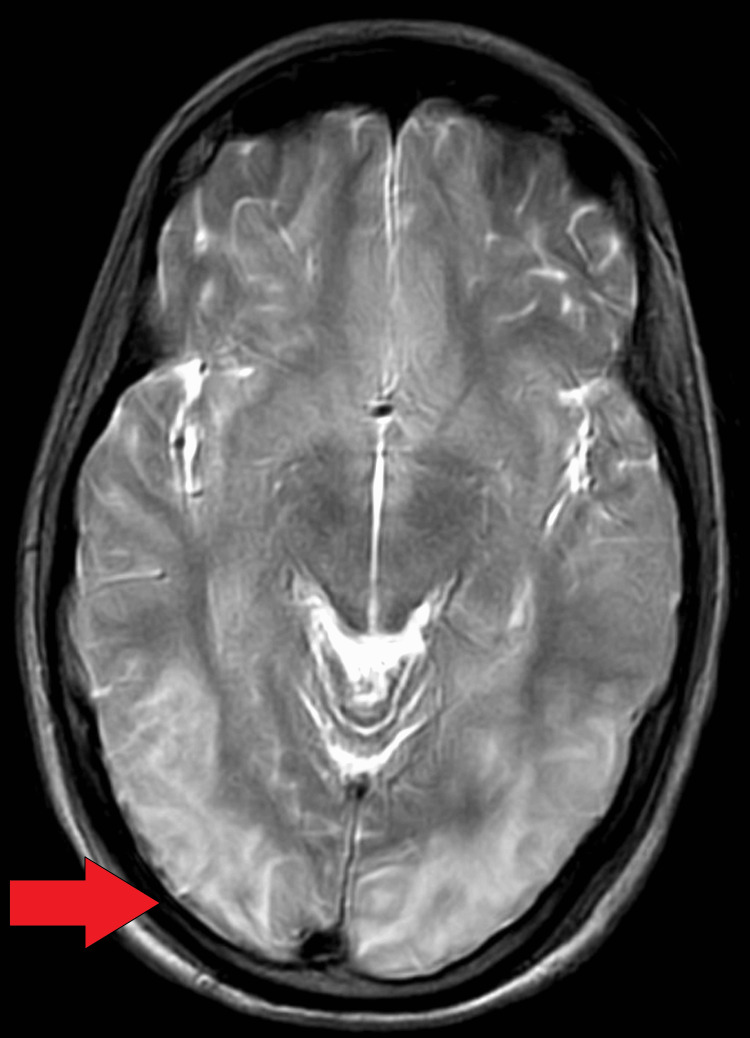 Figure 4
Figure 4 Figure 5
Figure 5| Parameter | Patient values | Normal Range |
| Hemoglobin | 11.2 g/DL | 12-16 g/DL |
| Total leukocyte count | 11000 /nm3 | 4,500-11,000 /nm3 |
| Platelets | 1.83 x 103/mcL | 1.5-4.5 x 103 /mcL |
| Alanine transaminase | 16 U/L | <35 U/L |
| Aspartate aminotransferase | 37 U/L | 14-36 U/L |
| Urea | 20 mg/dl | 7-17 mg/dl |
| Serum creatinine | 0.9 mg/dl | 0.52-1.04 mg/dl |
| Lactate dehydrogenase | 496 U/L | 140-280 U/L |
| Uric acid | 6.5 mg/dl | 2.5-6.5 mg/dl |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAssisted Reproductive Technology and Twin Pregnancy · Pregnancy and preeclampsia studies · Prenatal Screening and Diagnostics
Introduction
It is relatively uncommon for a single fetus to experience demise within the first three months of pregnancy in twin pregnancies without significant adverse effects on the survival and development of the other fetus [1]. Nevertheless, twin pregnancies inherently pose higher risks for unfavorable outcomes affecting both maternal and fetal health. The primary contributors to perinatal morbidity and mortality in such cases are intrauterine growth retardation and premature birth [2]. A less common, yet impactful, obstetric complication associated with heightened rates of morbidity and mortality for both the fetus and the mother is the demise of a fetus following the completion of the first trimester. This occurrence has been correlated with substantial adverse effects on the physical and neurological development of the surviving fetus, resulting in additional psychological stress for both the obstetrician and the parents [3]. Furthermore, such incidents have been associated with maternal disseminated intravascular coagulation. In cases of pre-eclampsia, a condition characterized by a progressive clinical course, the only effective treatment is the delivery of the placenta [1,4]. This report presents a rare case involving dichorionic twins in a 31-year-old female who developed pre-eclampsia following the intrauterine demise of one fetus. While there are a limited number of case reports documenting the resolution of pre-eclampsia after the demise of one twin, instances of pre-eclampsia developing after the demise of a fetus have not been widely reported.
Case presentation
This case presentation involves a 31-year-old G2A1 woman at 24+4 weeks of gestational age with a dichorionic diamniotic twin pregnancy conceived through in vitro fertilization. The patient, who had a cervical stitch in situ, presented for a routine antenatal check-up, during which the incidental discovery of the demise of one twin was made. The demise of the single fetus occurred at 24 weeks of gestation, resulting in severe pregnancy-induced hypertension with pulmonary edema (Figure 1).
Twins delivered at 24 weeks of gestation: A) Twin Fetus; B) Fetus with IUD.IUD: Intra-uterine death.
While the patient's vital signs were stable, a per-abdomen examination revealed a detectable heart rate for only one fetus through fetal Doppler. Subsequent ultrasonography confirmed the intrauterine fetal demise of one twin and indicated intrauterine growth retardation (IUGR) in the surviving fetus. Blood investigations revealed elevated lactate dehydrogenase (LDH) and uric acid levels, while liver enzymes remained within normal limits. Additional details can be found in Table 1.
Table 1: Laboratory investigation of the patient.
<table><tbody><tr><td rowspan="1" colspan="1">Parameter</td><td rowspan="1" colspan="1">Patient values</td><td rowspan="1" colspan="1">Normal Range</td></tr><tr><td rowspan="1" colspan="1">Hemoglobin</td><td rowspan="1" colspan="1">11.2 g/DL</td><td rowspan="1" colspan="1">12-16 g/DL</td></tr><tr><td rowspan="1" colspan="1">Total leukocyte count</td><td rowspan="1" colspan="1">11000 /nm3</td><td rowspan="1" colspan="1">4,500-11,000 /nm3</td></tr><tr><td rowspan="1" colspan="1">Platelets</td><td rowspan="1" colspan="1">1.83 x 10<sup>3</sup>/mcL</td><td rowspan="1" colspan="1">1.5-4.5 x 10<sup>3</sup> /mcL</td></tr><tr><td rowspan="1" colspan="1">Alanine transaminase</td><td rowspan="1" colspan="1">16 U/L</td><td rowspan="1" colspan="1"><35 U/L</td></tr><tr><td rowspan="1" colspan="1">Aspartate aminotransferase</td><td rowspan="1" colspan="1">37 U/L</td><td rowspan="1" colspan="1">14-36 U/L</td></tr><tr><td rowspan="1" colspan="1">Urea</td><td rowspan="1" colspan="1">20 mg/dl</td><td rowspan="1" colspan="1">7-17 mg/dl</td></tr><tr><td rowspan="1" colspan="1">Serum creatinine</td><td rowspan="1" colspan="1">0.9 mg/dl</td><td rowspan="1" colspan="1">0.52-1.04 mg/dl</td></tr><tr><td rowspan="1" colspan="1">Lactate dehydrogenase</td><td rowspan="1" colspan="1">496 U/L</td><td rowspan="1" colspan="1">140-280 U/L</td></tr><tr><td rowspan="1" colspan="1">Uric acid</td><td rowspan="1" colspan="1">6.5 mg/dl</td><td rowspan="1" colspan="1">2.5-6.5 mg/dl</td></tr></tbody></table>The patient's medical history included hypothyroidism, for which she had been taking Tab Thyrox 37.5 mg until it was discontinued after her last delivery. She had undergone three ovum pick-ups and experienced one embryo transfer failure. Additionally, a diagnostic hysteroscopy uncovered an anterior wall septum, leading to septoplasty; a non-patent left ostia, prompting lateral wall metroplasty; and the instillation of platelet-rich plasma. The patient, admitted on the same day due to these findings, initially exhibited stable conditions and normal blood pressure. However, her blood pressure spiked to 180/110 mmHg the next day.
Upon admission, the patient was prescribed IV labetalol and prophylactic magnesium sulfate. Subsequently, she developed anasarca, prompting consultation with an emergency treating physician. The treatment plan included IV labetalol, tab Nicardia, IV Lasix, and continuous monitoring of vital signs and fetal heart rate. Complaints of breathlessness led to a chest X-ray, revealing evidence of pulmonary edema consistent with generalized anasarca (Figure 2).
Pulmonary edema.
Despite treatment, the patient's blood pressure remained uncontrolled. Consequently, a joint decision to terminate the pregnancy for the mother's health was made. Cervical stitch removal and insertion of an intra-cervical Foley catheter with misoprostol administration were performed for cervical dilation and contractions. Twins were delivered, with one showing no signs of life post-delivery. Autopsy of both fetuses and the placenta yielded no discernible cause for fetal death. The patient's blood pressure normalized post-delivery, indicating that maternal complications, including pregnancy-induced hypertension and pulmonary edema, were associated with the demise of one fetus (Figure 3).
Improvement in pulmonary edema after treatment.
An MRI brain plain with magnetic resonance venography (MRV) revealed T2 fluid-attenuated inversion recovery (FLAIR) hyperintense foci over the bilateral corona radiata, bilateral cerebellum, left occipital cortex, midbrain, and pons. No diffusion restriction or blooming features suggestive of reversible posterior leukoencephalopathy syndrome, a common complication of hypertensive disorders of pregnancy, were observed (Figures 4-5).
Abnormal hyperintense lesions confluent in both parieto-occipital lobes on T2-weighted MRI scan.
Abnormal hyperintense lesion confluent in both parieto-occipital lobes upon FLAIR scan.FLAIR: Fluid-Attenuated Inversion Recovery.
Discussion
Research studies indicate an incidence rate of 2.5% to 6% for fetal death in twin pregnancies, a figure notably higher than the 0.3% to 0.6% range observed in pregnancies with a single fetus [3-5]. In pregnancies with a single fetus, intrauterine death is reported as insignificant at any specific point during the pregnancy. In contrast, in cases of twin pregnancies, the demise of one fetus within the initial three months has relatively fewer repercussions on the development and survival of the remaining fetus. However, if fetal death occurs in the second trimester or later, significant adverse outcomes are observed for both maternal and fetal health. Such instances are associated with complications like intrauterine growth restriction (IUGR), perinatal mortality, preeclampsia, and preterm labor [5,6].
Interestingly, some cases suggest an increased survival rate for the second fetus when the death of the first fetus occurs at 33 gestational weeks [1]. Twin pregnancies, particularly those of monochorionic origin, report higher rates of single fetal deaths (50%-70%) compared to pregnancies of dichorionic origin [3]. Complications related to single fetal deaths in or after the second trimester include IUGR, chromosomal anomalies, compromised physical growth, neurological disorders, umbilical cord anomalies, and sepsis. Maternal morbidities in these cases include preeclampsia, placental abruptions, and other complications with potentially significant adverse outcomes [7-8]. Cases involving the continuation of pregnancy for more than six weeks after the death of one fetus are associated with serious complications. The most significant consequence is the potential development of diffuse intravascular coagulation (DIC), primarily caused by the release of thromboplastin and fibrin protein into the mother's bloodstream by the deceased fetus, commonly referred to as 'fetal death syndrome' [9].
The existing literature includes reports of complete resolution of preeclampsia following the death of a solitary fetus [10]. However, in our investigation, an unexpected scenario unfolded: preeclampsia manifested after the death of a single fetus. Neither of the two groups in our study experienced a case of DIC after a single intrauterine fetal death [11]. While a single intrauterine fetal death generally leads to a favorable outcome, our case deviated from this norm, as the event triggered the development of preeclampsia, further complicating the mother's health. It is crucial to counsel both parents on the necessity of a post-mortem examination of the deceased fetus, especially when the cause of death is undefined. Placental analysis for various aspects should also be considered. Given that neurological and physical abnormalities are common complications when a single fetus perishes in a twin pregnancy, a comprehensive physical and neural assessment should be conducted using various radiological and imaging modalities. This radiological screening can aid in identifying any abnormalities and managing them, with regular monitoring of postnatal fetal growth [3,7,8].
Conclusions
This represents a rare occurrence where the development of pre-eclampsia followed the demise of a single intrauterine fetus. While typically favorable outcomes are observed after the death of a single fetus, unfortunately, our case does not align with this trend. The existing literature documents cases where pre-eclampsia completely resolves after the death of a single fetus, but our unique case, hitherto unreported, demonstrates the opposite phenomenon. It underscores the variability and complexity inherent in obstetrics, emphasizing that each pregnancy is valuable and warrants diligent efforts to achieve positive outcomes for both the mother and the fetus. This case serves as a poignant reminder that the field of obstetrics continually presents unexpected scenarios. The uniqueness of this case highlights the need for further research, particularly in the realm of twins and their intricate narratives. Recognizing the distinctiveness of this situation, there is a call for more in-depth investigations to broaden our understanding and contribute to the evolving knowledge within obstetrics.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Review of twin pregnancies with single fetal death: management, maternal and fetal outcome J Obstet Gynaecol India Jain D Purohit RC 1801836420142496650110.1007/s 13224-013-0500-5PMC 4061330 · doi ↗ · pubmed ↗
- 2Perinatal outcomes in twin pregnancies complicated by maternal morbidity: evidence from the WHO Multicountry Survey on Maternal and Newborn Health BMC Pregnancy Childbirth Santana DS Silveira C Costa ML 4491820183045390810.1186/s 12884-018-2082-9PMC 6245698 · doi ↗ · pubmed ↗
- 3Single fetal demise in twin pregnancy-a great concern but still a favorable outcome Diseases Stefanescu BI Adam AM Constantin GB Trus C 33920213394694610.3390/diseases 9020033 PMC 8161807 · doi ↗ · pubmed ↗
- 4Monofetal death in multiple pregnancies: Risks for the co-Twin, risk factors and obstetrical management Eur J Obs Gynecol Reprod Biol Gaucherand P Rudigoz RC Piacenza JM 11111555199410.1016/0028-2243(94)90064-77958148 · doi ↗ · pubmed ↗
- 5Prognosis of the co-twin following spontaneous single intrauterine fetal death in twin pregnancies: a systematic review and meta-analysis BJOG Mackie FL Rigby A Morris RK Kilby MD 56957812620193046117910.1111/1471-0528.15530 · doi ↗ · pubmed ↗
- 6Twin pregnancy with intrauterine death of one twin Am J Obs Gynecol Enbom JA 424429152198510.1016/s 0002-9378(85)80152-64014334 · doi ↗ · pubmed ↗
- 7Single intrauterine fetal demise in twin pregnancies and pregnancy outcomes J South Asian Feder Obst Gynae Reddy AC Vasanthalakshmi GN 137141132021
- 8Conservative management of single fetal death in twin pregnancy at a tertiary health institution in southern Nigeria: a case report J Dent Med Sci Babah OA. Olamijulo A Ayanbode OS Sanusi MM 7983132014