Optimizing Physiotherapeutic Approaches in Parkinson’s Disease Post-spinal Fixation Surgery: A Case Report
Prajyot Ankar, Neha P Arya, Tejaswini Fating, Anam R Sasun

TL;DR
This case report shows how a tailored physiotherapy program improved mobility and function in a Parkinson’s patient after spinal surgery.
Contribution
The paper presents a novel rehabilitation approach for Parkinson’s patients post-spinal fixation surgery, emphasizing strength training and functional outcomes.
Findings
The rehabilitation program significantly improved joint range of motion and muscle strength.
Functional independence and balance were notably enhanced post-intervention.
Lower limb function and disability scores showed marked improvement.
Abstract
Patients with Parkinson's disease (PD) exhibit both a severe neuromuscular disorder and low bone quality at presentation. These issues are made worse by inactivity and a chairbound state. Each and every pathologic and degenerative process that affects the naturally aging spine also affects these individuals. Stooped posture is a symptom of a disease and can easily cause spinal degeneration. PD is associated with many physical abnormalities that cause a unique and specific need for rehabilitation. Patients' experiences highlight the challenges doctors face in diagnosis, treatment, and rehabilitation. This case report details the rehabilitation of a 67-year-old patient with PD who underwent spinal fixation for spinal stenosis and presented with complaints of weakness in both lower limbs. An advanced rehabilitation program was devised, primarily emphasizing strength training to enhance…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1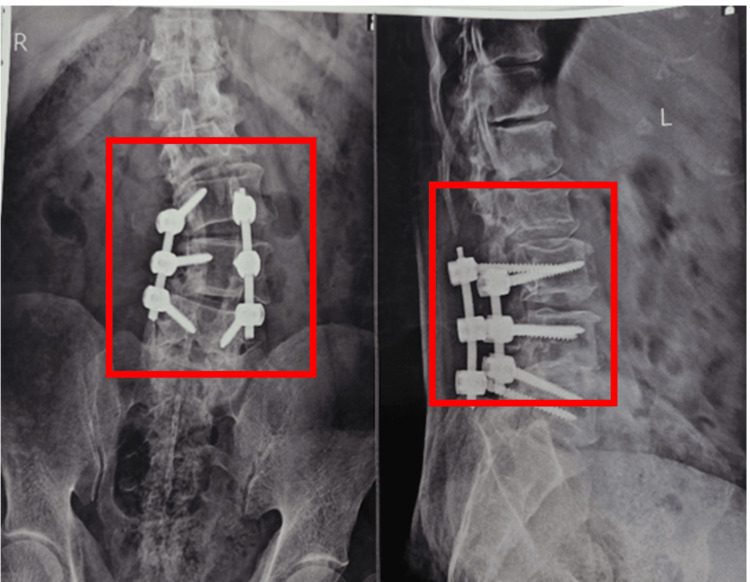 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4| Muscle group | Action | Left | Right |
| Shoulder | Flexors | 3- | 3- |
| Extensors | 3- | 3- | |
| Abductors | 3- | 3- | |
| Adductors | 3 | 3 | |
| Elbow | Flexors | 3 | 3 |
| Extensors | 3 | 3 | |
| Wrist | Flexors | 2+ | 2+ |
| Extensors | 2+ | 2+ | |
| Hip | Abductors | 2 | 2 |
| Adductors | 2 | 2 | |
| Flexors | 2- | 2- | |
| Extensors | 2- | 2- | |
| Knee | Extensors | 3- | 3- |
| Flexors | 2+ | 2+ | |
| Ankle | Plantar Flexors | 3- | 3- |
| Dorsiflexors | 2+ | 2+ |
| Joints | Movement | Right | Left |
| Shoulder | Flexion | 0-110˚ | 0-105˚ |
| Extension | 0-35˚ | 0-35˚ | |
| Adduction | 0-115˚ | 0-120˚ | |
| Elbow | Flexion | 0-145˚ | 0-145˚ |
| extension | 145-0˚ | 145-0˚ | |
| Wrist | Flexion | 0-65˚ | 0-60˚ |
| Extension | 0-68˚ | 0-70˚ | |
| Hip | Flexion | 0-30˚ | 0-35˚ |
| Extension | 0-5˚ | 0-5˚ | |
| Knee | Flexion | 0-60˚ | 0-60˚ |
| Ankle | Plantarflexion | 0-45˚ | 0-45˚ |
| Dorsiflexion | 0-10˚ | 0-10˚ |
| Problem identified | Physiotherapy goals | Interventions |
| Patient education | Education and counsel to patients | Patient education about his condition and the importance of physiotherapy explanation about the treatment. |
| Lower extremity weakness | To improve lower extremity muscle strength | Active assisted hamstring curls, dynamic quadriceps, VMO strengthening, progressing to active exercises, active assisted SLR, hip abduction in supine lying progressing to active SLR and hip abduction in side-lying, ankle pumps (10 reps x 2 sets), pelvic bridging (5 reps x 2 sets), wall supported squats (5 reps x 2 sets), PNF rhythmic stabilization to hamstring and quadriceps. |
| Upper extremity weakness | To improve the strength of the upper extremities. | Shoulder girdle strengthening with ½ kg dumbbell, bicep curls with ½ kg, wrist strengthening with ½ kg, gripping activities (10 reps x 2 sets). |
| Reduced movement amplitude | To improve movement quality and amplitude | LSVT BIG exercises – floor to ceiling, side to side (10 reps x 2 sets). |
| Difficulty in walking | To improve gait pattern | Walking with the support of a walker after 2 weeks progressed to unsupported walking, walking on the foot marks, treadmill walking around the obstacles and over the obstacles. |
| Unable to maintain dynamic balance | To improve dynamic balance | Weight shifting in standing, multidirectional functional reach in standing, heel raises, toe raises, balancing upon the unstable surface (10 reps x 2 sets) |
| Compromised cardiovascular fitness | To enhance oxygen consumption capacity | Treadmill training for 10 min daily with rest intervals, progressing to 20 mins daily. |
| To improve resting tremors | To decrease resting tremors | Progressive resistance training programme using weighted vests. (10 reps, 2 sets) |
| Outcome measures | Pre-treatment | Post-treatment |
| Oswestry Disability Index | 30 | 14 |
| Functional Independence Measure | 100 | 119 |
| Lower limb functional scale | 32 | 48 |
| Berg Balance scale | 22 | 40 |
| Muscle group | Action | Left | Right |
| Shoulder | Flexors | 3 | 3 |
| Extensors | 3 | 3 | |
| Abductors | 3 | 3 | |
| Adductors | 3 | 3 | |
| Elbow | Flexors | 3+ | 3+ |
| Extensors | 3+ | 3+ | |
| Wrist | Flexors | 3 | 3 |
| Extensors | 3 | 3 | |
| Hip | Abductors | 3- | 3- |
| Adductors | 3- | 3- | |
| Flexors | 3- | 3- | |
| Extensors | 3- | 2- | |
| Knee | Extensors | 3 | 3 |
| Flexors | 3 | 3 | |
| Ankle | Plantar Flexors | 3 | 3 |
| Dorsiflexors | 3- | 3- |
| Joints | Movement | Right | Left |
| Shoulder | Flexion | 0- 170˚ | 0-172˚ |
| Extension | 0-50˚ | 0-50˚ | |
| Adduction | 0-160˚ | 0-160˚ | |
| Elbow | Flexion | 0-145˚ | 0-145˚ |
| extension | 145-0˚ | 145-0˚ | |
| Wrist | Flexion | 0-75˚ | 0-76˚ |
| Extension | 0-70˚ | 0-70˚ | |
| Hip | Flexion | 0-75˚ | 0-78˚ |
| Extension | 0-15˚ | 0-20˚ | |
| Knee | Flexion | 0-135˚ | 0-135˚ |
| Ankle | Plantarflexion | 0-48˚ | 0-50˚ |
| Dorsiflexion | 0-15˚ | 0-15˚ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParkinson's Disease and Spinal Disorders · Parkinson's Disease Mechanisms and Treatments · Botulinum Toxin and Related Neurological Disorders
Introduction
Parkinson's disease (PD), also known as neurodegenerative disease, is a disease that primarily affects the central nervous system (CNS) of the brain. PD, in particular, affects the substantia nigra, a region of the brain located in the midbrain [1]. It is worth noting that PD becomes more common as we get older. Research shows that about 1.5% of people age 60 and older may have PD. Importantly, this means that the risk of PD increases as people get older [2]. PD is a degenerative disease that affects the brain and involves the loss of neurons responsible for dopamine production [3]. It is accompanied by motor symptoms such as tremors, slow movement (bradykinesia), rigidity, and difficulty in controlling the body [4]. The five types of pain experienced by PD patients are musculoskeletal pain, central pain, neuropathic pain, akathisia pain, and dystonia-related pain. Additionally, people with PD often experience symptoms such as thinking and memory problems (cognitive confusion), mood swings, and problems with automatic body functions (autonomic dysfunction). Patients with PD are more likely to experience postoperative complications and unintended revision surgeries following spinal fusion, according to prior research. Furthermore, fusion rates are generally lower and outcomes are worse for PD patients undergoing surgery, particularly for those who have multi-tiered fusion. Although the exact cause is not fully understood, it is believed that a combination of events and environmental influences contributed to its development [5]. Treatment of PD requires a combination of medication and physical therapy to improve the quality of life of people with PD. This report investigates physical therapy after spine surgery in a patient with PD-like symptoms [6]. Management of postoperative complications, especially when neurological disease occurs, causes serious problems in treatment. The combination of spinal pathology and PD-like symptoms in the brain needs to be specialized and treated to return to normal [7].
Of the various pathways that underlie pain related to PD, 40 to 90% of reported symptoms are related to musculoskeletal pain. Complementary therapies, such as physiotherapy and chiropractic adjustments, are recommended for the treatment of musculoskeletal pain. These therapies target joint mobility, motor strengthening, pain management, and postural training exercises. The clinical picture becomes particularly difficult in patients who undergo spine surgery after showing symptoms of PD [8]. It is a serious disease caused by a combination of non-physical symptoms that cause serious complications, especially in spine-related surgical procedures [9]. Interactions between motor control, movement, and post-exercise recovery should be planned and monitored in Parkinson's patients. In this article, we will describe the treatment of a patient with PD characteristics who underwent spine surgery but later developed complications [10]. Postural deformities such as torticollis, anterior neck, Pisa syndrome, and scoliosis are common disabilities in PD and atypical PD [11]. These malformations have a multifactorial pathophysiology that includes muscle stiffness, axial dystonia, myopathy-related weakness, muscle weakness, and spinal cord changes [12]. The impact of these factors varies between patients and specific symptoms. It is a complex disease with many symptoms affecting both motor and non-motor systems. These may include irregular sleep patterns, psychological disorders (such as anxiety and depression), cognitive impairments, and functional disorders (such as constipation or mild gastrointestinal problems) [13].
Case presentation
A 67-year-old male patient with Grade 2 PD visited the outpatient department, complaining of difficulty walking and maintaining balance. The patient had a history of radiating lower back pain with tingling numbness in bilateral lower limbs, along with weakness in the lower limbs, a year ago. Initially, the symptoms were milder. The patient consulted a local practitioner who prescribed medications, but there was no relief after one month. He visited another hospital with the same complaints, and a magnetic resonance imaging (MRI) was conducted, revealing spinal canal stenosis. Surgery was recommended, and the procedure was performed a week later. Postoperatively, the patient experienced a reduction in pain and tingling numbness, but weakness in the lower limbs persisted. Unfortunately, the patient was not engaged in any rehabilitation. Additionally, two years ago, the patient reported involuntary movements in both upper and lower limbs, coupled with difficulty in maintaining balance. Following the medical consultation, the diagnosis was Grade 2 PD, and ongoing treatment was prescribed. However, no referral was provided for rehabilitation. The patient also has a six-year history of hypertension. Currently, the patient has visited the physiotherapy outpatient department for rehabilitation.
Clinical findings
Consent was obtained prior to the examination. The patient was conscious, cooperative, and oriented to time, place, and person. The patient was examined in a supine position and displayed a mask-like facial expression, and a fully healed scar of approximately 10 cm was noted on the lower back area. During palpation, muscle tone examination indicated a grade 3+ (increased muscle tone) for the upper limbs and a grade 2+ (normal muscle tone) for the lower limbs, as per the tone grading system. Manual muscle testing (MMT) was conducted, revealing reduced muscle strength, particularly pronounced in the lower limbs. All the superficial, deep, and combined cortical sensations were intact. Postural examination showed a forward head posture, shoulder protraction, and a flat back posture. Balance assessment was also conducted using the Berg Balance Scale (BBS), revealing impaired balance. Table 1 shows the examination findings of MMT.
Table 1: Manual muscle testing pre-rehabilitation5+: Complete range of motion (ROM) against gravity with maximal resistance, 4: complete ROM against gravity with moderate resistance, 3+: complete ROM against gravity with minimal resistance, 3: complete ROM against gravity, 3-: some but not complete ROM against gravity, 2+: Initiates motion against gravity, 2: complete ROM with gravity eliminated, 2-: Initiates motion if gravity is eliminated, 1: Evidence of slight contractility but no joint motion, 0: No contraction palpated
<table><tbody><tr><td rowspan="1" colspan="1">Muscle group</td><td rowspan="1" colspan="1">Action</td><td rowspan="1" colspan="1">Left</td><td rowspan="1" colspan="1">Right</td></tr><tr><td rowspan="4" colspan="1">Shoulder</td><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Abductors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Adductors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="2" colspan="1">Elbow</td><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="2" colspan="1">Wrist</td><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">2+</td><td rowspan="1" colspan="1">2+</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">2+</td><td rowspan="1" colspan="1">2+</td></tr><tr><td rowspan="4" colspan="1">Hip</td><td rowspan="1" colspan="1">Abductors</td><td rowspan="1" colspan="1">2</td><td rowspan="1" colspan="1">2</td></tr><tr><td rowspan="1" colspan="1">Adductors</td><td rowspan="1" colspan="1">2</td><td rowspan="1" colspan="1">2</td></tr><tr><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">2-</td><td rowspan="1" colspan="1">2-</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">2-</td><td rowspan="1" colspan="1">2-</td></tr><tr><td rowspan="2" colspan="1">Knee</td><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">2+</td><td rowspan="1" colspan="1">2+</td></tr><tr><td rowspan="2" colspan="1">Ankle</td><td rowspan="1" colspan="1">Plantar Flexors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Dorsiflexors</td><td rowspan="1" colspan="1">2+</td><td rowspan="1" colspan="1">2+</td></tr></tbody></table>Table 2 depicts the range of motion (ROM) findings pre-rehabilitation.
Table 2: Range of motion examination pre-rehabilitation
<table><tbody><tr><td rowspan="1" colspan="1">Joints</td><td rowspan="1" colspan="1">Movement</td><td rowspan="1" colspan="1">Right</td><td rowspan="1" colspan="1">Left</td></tr><tr><td rowspan="3" colspan="1">Shoulder</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-110˚</td><td rowspan="1" colspan="1">0-105˚</td></tr><tr><td rowspan="1" colspan="1">Extension</td><td rowspan="1" colspan="1">0-35˚</td><td rowspan="1" colspan="1">0-35˚</td></tr><tr><td rowspan="1" colspan="1">Adduction</td><td rowspan="1" colspan="1">0-115˚</td><td rowspan="1" colspan="1">0-120˚</td></tr><tr><td rowspan="2" colspan="1">Elbow</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-145˚</td><td rowspan="1" colspan="1">0-145˚</td></tr><tr><td rowspan="1" colspan="1">extension</td><td rowspan="1" colspan="1">145-0˚</td><td rowspan="1" colspan="1">145-0˚</td></tr><tr><td rowspan="2" colspan="1">Wrist</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-65˚</td><td rowspan="1" colspan="1">0-60˚</td></tr><tr><td rowspan="1" colspan="1">Extension</td><td rowspan="1" colspan="1">0-68˚</td><td rowspan="1" colspan="1">0-70˚</td></tr><tr><td rowspan="2" colspan="1">Hip</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-30˚</td><td rowspan="1" colspan="1">0-35˚</td></tr><tr><td rowspan="1" colspan="1">Extension</td><td rowspan="1" colspan="1">0-5˚</td><td rowspan="1" colspan="1">0-5˚</td></tr><tr><td rowspan="1" colspan="1">Knee</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-60˚</td><td rowspan="1" colspan="1">0-60˚</td></tr><tr><td rowspan="2" colspan="1">Ankle</td><td rowspan="1" colspan="1">Plantarflexion</td><td rowspan="1" colspan="1">0-45˚</td><td rowspan="1" colspan="1">0-45˚</td></tr><tr><td rowspan="1" colspan="1">Dorsiflexion</td><td rowspan="1" colspan="1">0-10˚</td><td rowspan="1" colspan="1">0-10˚</td></tr></tbody></table>Investigations
The patient underwent an MRI before surgery, which showed the bilateral lateral recess is narrowed and the left-sided disc posterior disc protrusion at the L1-L2 disc level that is indenting over the anterior thecal sac. A widespread disc bulge with e/o causes the spinal canal to shrink at the L2-L3, L3-L4 disc level, obliterating the right and bilateral lateral recesses. At the L4-L5 disc level, there is e/o inferior disc extrusion that results in nearly complete spinal canal obliteration, as shown in Figure 1.
Pre-operative MRI showing compression at L1-L5 (red circle)
Figure 2 depicts a post-operative X-ray showing spinal fixation.
The post-operative X-ray of the lumbar spine (red squares)
Physiotherapy interventions
A physiotherapy protocol was customized for the patient according to the impairments, and the duration of the rehabilitation program was eight weeks. Table 3 shows the physiotherapy rehabilitation protocol.
Table 3: Physiotherapy interventionReps: repetition, sec: second, Min: minutes, PNF: Proprioceptive Neuromuscular Facilitation, VMO: Vastus Medialis Oblique, LSVT: Lee Silverman Voice Treatment, SLR: Straight Leg Raising
<table><tbody><tr><td rowspan="1" colspan="1">Problem identified</td><td rowspan="1" colspan="1">Physiotherapy goals</td><td rowspan="1" colspan="1">Interventions</td></tr><tr><td rowspan="1" colspan="1">Patient education</td><td rowspan="1" colspan="1">Education and counsel to patients</td><td rowspan="1" colspan="1">Patient education about his condition and the importance of physiotherapy explanation about the treatment.</td></tr><tr><td rowspan="1" colspan="1">Lower extremity weakness</td><td rowspan="1" colspan="1">To improve lower extremity muscle strength</td><td rowspan="1" colspan="1">Active assisted hamstring curls, dynamic quadriceps, VMO strengthening, progressing to active exercises, active assisted SLR, hip abduction in supine lying progressing to active SLR and hip abduction in side-lying, ankle pumps (10 reps x 2 sets), pelvic bridging (5 reps x 2 sets), wall supported squats (5 reps x 2 sets), PNF rhythmic stabilization to hamstring and quadriceps.</td></tr><tr><td rowspan="1" colspan="1">Upper extremity weakness</td><td rowspan="1" colspan="1">To improve the strength of the upper extremities.</td><td rowspan="1" colspan="1">Shoulder girdle strengthening with ½ kg dumbbell, bicep curls with ½ kg, wrist strengthening with ½ kg, gripping activities (10 reps x 2 sets).</td></tr><tr><td rowspan="1" colspan="1">Reduced movement amplitude</td><td rowspan="1" colspan="1">To improve movement quality and amplitude</td><td rowspan="1" colspan="1">LSVT BIG exercises – floor to ceiling, side to side (10 reps x 2 sets).</td></tr><tr><td rowspan="1" colspan="1">Difficulty in walking</td><td rowspan="1" colspan="1">To improve gait pattern</td><td rowspan="1" colspan="1">Walking with the support of a walker after 2 weeks progressed to unsupported walking, walking on the foot marks, treadmill walking around the obstacles and over the obstacles.</td></tr><tr><td rowspan="1" colspan="1">Unable to maintain dynamic balance</td><td rowspan="1" colspan="1">To improve dynamic balance</td><td rowspan="1" colspan="1">Weight shifting in standing, multidirectional functional reach in standing, heel raises, toe raises, balancing upon the unstable surface (10 reps x 2 sets)</td></tr><tr><td rowspan="1" colspan="1">Compromised cardiovascular fitness</td><td rowspan="1" colspan="1">To enhance oxygen consumption capacity</td><td rowspan="1" colspan="1">Treadmill training for 10 min daily with rest intervals, progressing to 20 mins daily.</td></tr><tr><td rowspan="1" colspan="1">To improve resting tremors</td><td rowspan="1" colspan="1">To decrease resting tremors</td><td rowspan="1" colspan="1">Progressive resistance training programme using weighted vests. (10 reps, 2 sets)</td></tr></tbody></table>Figure 3 depicts the patient performing treadmill training.
Treadmill training
Figure 4 shows the patient walking on the treadmill over the obstacles.
Treadmill training with obstacles
Outcome measures
Assessment for outcome measures was taken pre- and post-rehabilitation on the eighth week, which included examination for ROM, MMT, and the following measures mentioned in Table 4.
Table 4: Outcome measures
<table><tbody><tr><td rowspan="1" colspan="1">Outcome measures</td><td rowspan="1" colspan="1">Pre-treatment</td><td rowspan="1" colspan="1">Post-treatment</td></tr><tr><td rowspan="1" colspan="1">Oswestry Disability Index</td><td rowspan="1" colspan="1">30</td><td rowspan="1" colspan="1">14</td></tr><tr><td rowspan="1" colspan="1">Functional Independence Measure</td><td rowspan="1" colspan="1">100</td><td rowspan="1" colspan="1">119</td></tr><tr><td rowspan="1" colspan="1">Lower limb functional scale</td><td rowspan="1" colspan="1">32</td><td rowspan="1" colspan="1">48</td></tr><tr><td rowspan="1" colspan="1">Berg Balance scale</td><td rowspan="1" colspan="1">22</td><td rowspan="1" colspan="1">40</td></tr></tbody></table>Table 5 shows MMT findings post-rehabilitation.
Table 5: MMT findings post-rehabilitationMMT: Manual muscle testing
<table><tbody><tr><td rowspan="1" colspan="1">Muscle group</td><td rowspan="1" colspan="1">Action</td><td rowspan="1" colspan="1">Left</td><td rowspan="1" colspan="1">Right</td></tr><tr><td rowspan="4" colspan="1">Shoulder</td><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="1" colspan="1">Abductors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="1" colspan="1">Adductors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="2" colspan="1">Elbow</td><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">3+</td><td rowspan="1" colspan="1">3+</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3+</td><td rowspan="1" colspan="1">3+</td></tr><tr><td rowspan="2" colspan="1">Wrist</td><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="4" colspan="1">Hip</td><td rowspan="1" colspan="1">Abductors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Adductors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr><tr><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">2-</td></tr><tr><td rowspan="2" colspan="1">Knee</td><td rowspan="1" colspan="1">Extensors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="1" colspan="1">Flexors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="2" colspan="1">Ankle</td><td rowspan="1" colspan="1">Plantar Flexors</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">3</td></tr><tr><td rowspan="1" colspan="1">Dorsiflexors</td><td rowspan="1" colspan="1">3-</td><td rowspan="1" colspan="1">3-</td></tr></tbody></table>Table 6 shows ROM examination post-rehabilitation.
Table 6: ROM examination post-rehabilitationROM: Range of motion
<table><tbody><tr><td rowspan="1" colspan="1">Joints</td><td rowspan="1" colspan="1">Movement</td><td rowspan="1" colspan="1">Right</td><td rowspan="1" colspan="1">Left</td></tr><tr><td rowspan="3" colspan="1">Shoulder</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0- 170˚</td><td rowspan="1" colspan="1">0-172˚</td></tr><tr><td rowspan="1" colspan="1">Extension</td><td rowspan="1" colspan="1">0-50˚</td><td rowspan="1" colspan="1">0-50˚</td></tr><tr><td rowspan="1" colspan="1">Adduction</td><td rowspan="1" colspan="1">0-160˚</td><td rowspan="1" colspan="1">0-160˚</td></tr><tr><td rowspan="2" colspan="1">Elbow</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-145˚</td><td rowspan="1" colspan="1">0-145˚</td></tr><tr><td rowspan="1" colspan="1">extension</td><td rowspan="1" colspan="1">145-0˚</td><td rowspan="1" colspan="1">145-0˚</td></tr><tr><td rowspan="2" colspan="1">Wrist</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-75˚</td><td rowspan="1" colspan="1">0-76˚</td></tr><tr><td rowspan="1" colspan="1">Extension</td><td rowspan="1" colspan="1">0-70˚</td><td rowspan="1" colspan="1">0-70˚</td></tr><tr><td rowspan="2" colspan="1">Hip</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-75˚</td><td rowspan="1" colspan="1">0-78˚</td></tr><tr><td rowspan="1" colspan="1">Extension</td><td rowspan="1" colspan="1">0-15˚</td><td rowspan="1" colspan="1">0-20˚</td></tr><tr><td rowspan="1" colspan="1">Knee</td><td rowspan="1" colspan="1">Flexion</td><td rowspan="1" colspan="1">0-135˚</td><td rowspan="1" colspan="1">0-135˚</td></tr><tr><td rowspan="2" colspan="1">Ankle</td><td rowspan="1" colspan="1">Plantarflexion</td><td rowspan="1" colspan="1">0-48˚</td><td rowspan="1" colspan="1">0-50˚</td></tr><tr><td rowspan="1" colspan="1">Dorsiflexion</td><td rowspan="1" colspan="1">0-15˚</td><td rowspan="1" colspan="1">0-15˚</td></tr></tbody></table>Discussion
The field of PD rehabilitation has been marked by a great deal of diversity. Physical exercise was initially suggested as a therapeutic approach for PD several years ago [14,15]. Since then, rehabilitation therapies have been viewed as a complementary measure to pharmacological and surgical interventions, aiming to optimize functional abilities [16]. Common rehabilitation approaches, including general physiotherapy involving stretching, muscle strengthening, balance, and postural exercises, as well as occupational therapy and treadmill training, are often employed to enhance mobility in individuals with PD [17]. Notably, resistance training is utilized to boost muscle strength, improving gait performance, while stretching helps alleviate the shortening of flexor muscles that contribute to abnormal flexed posture in PD. Lee Silverman Voice Treatment-BIG therapy (LSVT-BIG) emphasizes enhancing movement amplitude to attain larger, swifter, and more precise motions, with the goal of restoring typical movement patterns. By encouraging substantial movements, the therapy aims to counteract hypokinesia by influencing the individual's perception of their movement amplitude [18,19]. Promising results were observed in the restoration of motor functions after just one osteopathic therapy session or a chiropractic manipulation program. Similar to this, musculoskeletal disorders have been treated with a variety of approaches, with a focus on releasing neurological compromise, mobilizing restricted structures, and maximizing the function of afflicted muscles and joints [20].
The physiotherapy management of post-spinal surgery complications in a patient presenting with features of PD is a multifaceted challenge, requiring a tailored and multidisciplinary approach. A customized physiotherapy plan was implemented for eight weeks, which included strength training for both upper and lower limbs, balance training, aerobic training, and LSVT-BIG exercises to improve movement amplitude. A post-rehabilitation evaluation for outcomes was taken at the end of the eighth week, which included the MMT, Oswestry Disability Index, functional independence measure, lower limb functional scale, and BBS, which showed significant improvement likely to be generalized strength, independence for activities of daily living, balance, and lower extremity function. This shows the importance of a planned physiotherapy rehabilitation program in PD. The fact that this was a case report with only one patient observed, the lack of post-treatment X-rays, which made the study observational and the functional outcomes assessed are the study's limitations. Additional research is needed on PD patients who have undergone spinal surgeries.
Conclusions
This case report underscores the intricate interplay of spinal surgery complications and PD manifestations, emphasizing the necessity for comprehensive rehabilitation. The tailored eight-week physiotherapy intervention, encompassing strength and balance training, aerobic exercises, and LSVT-BIG therapy, yielded significant improvements. The observed enhancements in functional independence, balance, and muscle strength, as reflected in the post-treatment outcome measures, highlight the efficacy of an approach in addressing the complex needs of individuals with coexisting spinal and neurological conditions. This case underscores the importance of integrating rehabilitation strategies into the management of postoperative complications in Parkinson's patients, contributing valuable insights for future clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Priorities in Parkinson's disease research Nat Rev Drug Discov Meissner WG Frasier M Gasser T 3773931020112153256710.1038/nrd 3430 · doi ↗ · pubmed ↗
- 2Prevalence and incidence of Parkinson's disease in Europe Eur Neuropsychopharmacol von Campenhausen S Bornschein B Wick R 4734901520051596370010.1016/j.euroneuro.2005.04.007 · doi ↗ · pubmed ↗
- 3Clinical practice. Diagnosis and initial management of Parkinson's disease N Engl J Med Nutt JG Wooten GF 1021102735320051614828710.1056/NEJ Mcp 043908 · doi ↗ · pubmed ↗
- 4Motor symptoms in Parkinson's disease: a unified framework Neurosci Biobehav Rev Moustafa AA Chakravarthy S Phillips JR 7277406820162742245010.1016/j.neubiorev.2016.07.010 · doi ↗ · pubmed ↗
- 5An update on the diagnosis and treatment of Parkinson disease CMAJ Rizek P Kumar N Jog MS 1157116518820162722126910.1503/cmaj.151179 PMC 5088077 · doi ↗ · pubmed ↗
- 6Parkinson's disease BMJ Clarke CE 44144533520071776203610.1136/bmj.39289.437454.ADPMC 1962892 · doi ↗ · pubmed ↗
- 7Spino-pelvic alignment after surgical correction for developmental spondylolisthesis Eur Spine J Labelle H Roussouly P Chopin D Berthonnaud E Hresko T O'Brien M 117011761720081860035010.1007/s 00586-008-0713-y PMC 2527424 · doi ↗ · pubmed ↗
- 8Scoliosis in the elderly: a follow-up study Spine (Phila Pa 1976) Robin GC Span Y Steinberg R Makin M Menczel J 35535971982621571910.1097/00007632-198207000-00005 · doi ↗ · pubmed ↗