Knife-assisted incision for restoring esophageal lumen after surgical exclusion
Francesco Azzolini, Ernesto Fasulo, Francesco Vito Mandarino, Alberto Barchi, Silvio Danese

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1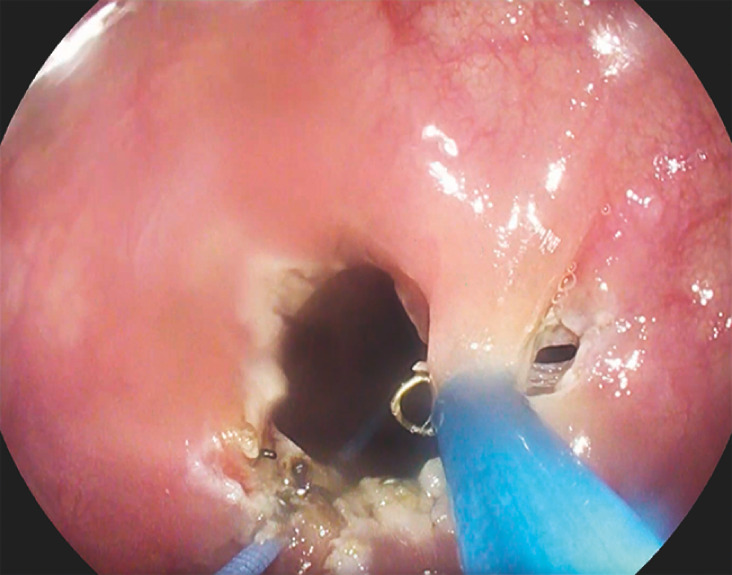 Fig. 2
Fig. 2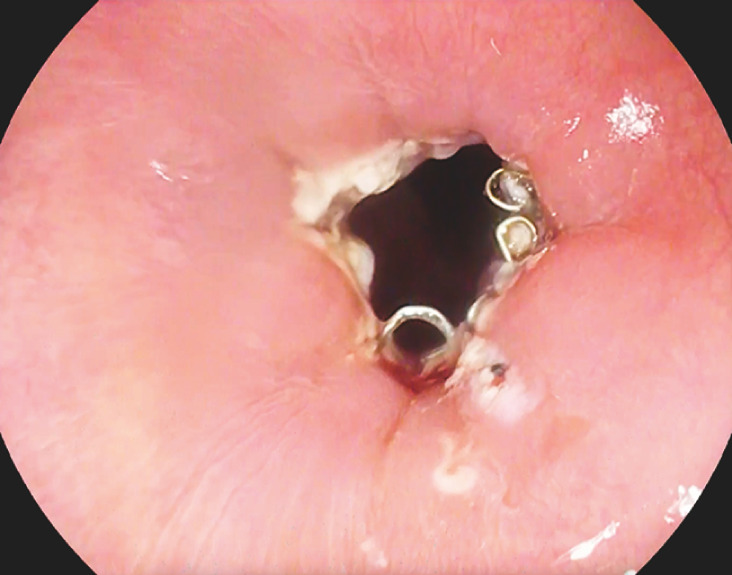 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Tracheal and airway disorders · Dysphagia Assessment and Management
Surgical repair with esophageal exclusion is a life-saving surgery for patients with mediastinitis following mid-esophageal perforation 1 . This is followed by either spontaneous recanalization of the organ or subsequent surgery to restore lumen patency 2 .
We present the case of a patient who underwent endoscopic restoration of the esophageal lumen after unsuccessful spontaneous recanalization following esophageal exclusion.
A 41-year-old man, with known achalasia, underwent pneumatic endoscopic dilation at another center, resulting in a 6 cm longitudinal laceration of the lateral esophageal wall. The patient developed mediastinitis and was treated by surgical repair of the laceration and esophageal exclusion with proximal staple line division.
At 4 months post-surgery, the patient continued to experience dysphagia with a liquid diet. Postoperative esophagograms revealed poor contrast passage across the staple lines. The patient was referred to our unit for endoscopic recanalization ( Video 1 ). Endoscopically, we found a moderate stenosis (caliber 6 mm) at the staple line site ( Fig. 1 ).
Endoscopic esophageal lumen recanalization after surgical exclusion.Video 1
Initial appearance of the esophageal lumen.
Initially, we placed a guidewire in the stapled lumen and performed dilation with Savary–Gilliard bougies up to 9 mm. Then, we extensively incised the fibrosis between the residual lumen and the stapled lumen using an L-type dissector (Finemedix, Daegu, Korea) ( Fig. 2 ). Finally protruding staple sutures were removed by cold forceps.
Incision of the fibrosis with L-type dissector (Finemedix, Daegu, Korea) to separate staples.
As a result, a well-patent esophageal lumen, traversable with a standard gastroscope (caliber 9.8 mm), was achieved ( Fig. 3 ). No leaks were detected on the intraprocedural esophagogram.
Final view: the staple line site was traversed by a standard gastroscope.
On the first postoperative day, an X-ray with contrast medium showed smooth contrast passage throughout the esophagus. The patient was discharged after resuming a soft diet. At the 3-month follow-up, he reported having no dysphagia.
To the best of our knowledge, this is the first report of endoscopic recanalization after surgical esophageal exclusion and describes a potential treatment option for similar complex cases.
Endoscopy_UCTN_Code_TTT_1AO_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lampridis S Mitsos S Hayward M The insidious presentation and challenging management of esophageal perforation following diagnostic and therapeutic interventions J Thorac Dis 2020122724273410.21037/jtd-19-409632642181 PMC 7330325 · doi ↗ · pubmed ↗
- 2Paramesh V Rumisek JD Chang FC Spontaneous recanalization of the esophagus after exclusion using nonabsorbable staples Ann Thorac Surg 1995591214121510.1016/0003-4975(94)00965-a 7733724 · doi ↗ · pubmed ↗