Endoscopic submucosal dissection combined with endoscopic hand suturing for a laterally spreading tumor spanning the anastomosis after radical resection of a rectal carcinoma
Shibo Song, Yi Liu, Lizhou Dou, Guiqi Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
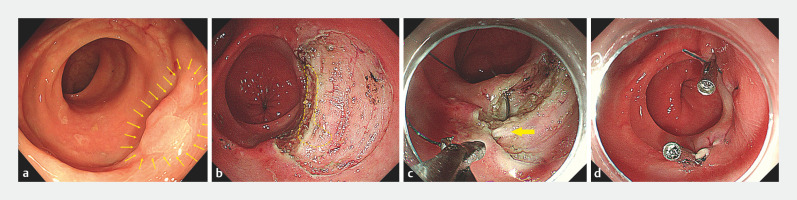 Fig. 1
Fig. 1- —CAMS Innovation Fund for Medical Sciences (CIFMS)
- —Sanming Project of Medicine in Shenzen Municipality10.13039/501100012151
- —Beijing Hope Run Special Fund of Cancer Foundation of China
- —Capital’s Funds for Health Improvement and Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Metastasis and carcinoma case studies · Gastrointestinal Tumor Research and Treatment
Precancerous lesions or early cancers located at the anastomosis after radical resection of a rectal carcinoma are relatively rare 1 2 . Recently, several studies have suggested that endoscopic submucosal dissection (ESD) is a favorable treatment for such lesions 3 4 5 ; however, because of severe adhesion in the submucosa of lesions that are located at the anastomosis, partial excision of the circular muscle layer may be required to prevent positive margins. We report a novel measure combining endoscopic hand suturing (EHS) with ESD, to close the postoperative defect following this, which is expected to be an ideal endoscopic method for precancerous lesions or early cancers that span the anastomosis after radical resection of a rectal carcinoma.
A 50-year-old man who underwent radical surgery for rectal cancer 1 year previously was diagnosed on follow-up with a 1.5 × 1.2-cm laterally spreading tumor (LST) spanning the anastomosis (about 5 cm from the anal verge) ( Fig. 1 a ). Although the biopsy of lesion showed low grade intraepithelial neoplasia (LGIN), given its malignant potential, the patient underwent ESD. The lesion was removed en bloc with partial muscularis propria to ensure the negative margin ( Fig. 1 b ). We sutured the defect with EHS ( Video 1 ). The muscularis propria was also partially sutured to avoid submucosal dead space ( Fig. 1 c ). Clips were used to fix the tail and head of the suture ( Fig. 1 d ). The resection and suture times were 41 and 30 minutes, respectively. No adverse events occurred. Histologically, complete resection of the LGIN was obtained.
Endoscopic images showing: a a 1.5×1.2-cm laterally spreading tumor (yellow arrows) spanning the anastomosis; b the defect left after endoscopic submucosal dissection (the yellow circle represents the area where partial muscularis propria was removed); c the defect being sutured, with the muscularis propria partially sutured to avoid submucosal dead space (yellow arrow); d the closed defect without dehiscence, with clips used to fix the tail and head of the suture.
A rectal defect after endoscopic submucosal dissection with partial excision of the circular muscle layer is completely closed using endoscopic hand suturing.Video 1
The use of ESD combined with EHS to treat an LST spanning the anastomosis has not been previously reported. Despite severe submucosal adhesion at the anastomotic site, it was still possible to remove the lesions en bloc with ESD, thereby preventing the patient needing to undergo further surgery, while EHS effectively prevented any wound-related adverse events. Further clinical experience with this technique is desirable.
Endoscopy_UCTN_Code_TTT_1AQ_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Matsunaga K Sasaki K Nozawa H Clinicopathological characteristics of anastomotic recurrence after curative resection for colorectal cancer: comparison with nonanastomotic local recurrences Dis Colon Rectum 202366 e 1014 e 102236649156 10.1097/DCR.0000000000002566 · doi ↗ · pubmed ↗
- 2Jung WB Yu CS Lim SB Anastomotic recurrence after curative resection for colorectal cancer World J Surg 20174128529410.1007/s 00268-016-3663-227481350 · doi ↗ · pubmed ↗
- 3Chen Z Dou L Zhang Y Safety and efficacy of endoscopic submucosal dissection for metachronous early cancer or precancerous lesions emerging at the anastomotic site after curative surgical resection of colorectal cancer Ann Transl Med 20208141110.21037/atm-20-206433313156 PMC 7723546 · doi ↗ · pubmed ↗
- 4Maehata T Kato M Ochiai Y Feasibility of endoscopic submucosal dissection for colorectal neoplasia at anastomotic sites: a retrospective study Surg Endosc 2020345495550010.1007/s 00464-019-07346-031932934 · doi ↗ · pubmed ↗
- 5Wang L Liu ZQ Liu JZ Endoscopic submucosal dissection for anastomotic lesions after colorectal surgery J Gastroenterol Hepatol 20233842443210.1111/jgh.1606336398853 · doi ↗ · pubmed ↗