Family Medicine Residents’ Perspectives in Dermatology Training
Jessica Howard, Lauren Hayley Siegel, Kelly Mok, Shannon Sibbald, Ken Masters, sathyanarayanan varadarajan

TL;DR
This study explores how training with a family physician in dermatology helps residents gain confidence and skills to better handle skin-related issues in their future practice.
Contribution
The study provides new insights into the value of dermatology training with family physicians for family medicine residents.
Findings
Residents experienced personal and professional enrichment through the training.
Residents gained a better understanding of system barriers and facilitators in dermatology.
Training with a family physician improved residents' comfort and skills in dermatology.
Abstract
This article was migrated. The article was marked as recommended. Purpose:Dermatological concerns are one of the most common presentations in family practice. Residents often feel inadequately prepared to address these concerns after graduation. This preliminary qualitative study was conducted to gain insight from residents about their post-graduate training in dermatology with a family physician practicing in dermatology. Methods:Family medicine residents (within five years of graduation) who completed their training at an academic family medicine centre in rural Southwestern Ontario affiliated with the local University’s Department of Family Medicine were interviewed (n=7). Phenomenological analysis was performed on the interviews using qualitative principles of immersion and emergence. Results: Three main themes based on training with a family physician were identified: 1)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
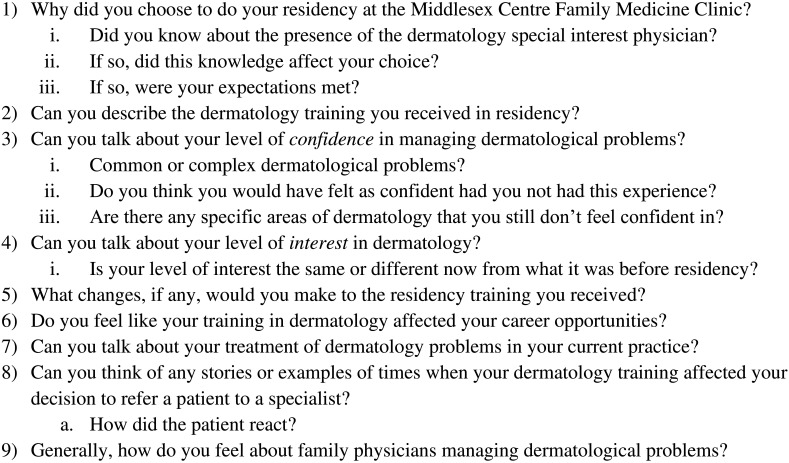 Figure 1
Figure 1| Procedures | |
|---|---|
| Incise and drain abscesses | Insert sutures |
| Repair laceration | Perform skin biopsies |
| Excise dermal lesions | Remove a foreign body |
| Perform wound debridement | Perform cryotherapy |
| Perform electrocautery | Scrape skin for fungus |
| Use a wood lamp | Release subungual hematoma |
| Drain acute paronychia | Partially remove a toenail |
| Perform wedge excision | Pare skin callus |
| Participant ID | Sex | Supervisor (JH or Other) | Years since residency |
|---|---|---|---|
| LY | M | Other | 1 |
| AO | F | Other | 4 |
| YH | F | JH | 1 |
| JS | F | Other | 2 |
| DZ | F | JH | 1 |
| KR | F | Other | 0 |
| HY | F | Other | 0 |
| Theme | Sub-themes |
|---|---|
| Clinical Competency | Confidence |
| Comfort | |
| Satisfaction | |
| Transferrable Skills | Diagnosis and treatment |
| Transferable skills | |
| Patient-centered care | |
| Health System Challenges | Referrals |
| Gap in Canadian healthcare | |
| Urban/rural care |
| Theme | Quotation Number | Quotation |
|---|---|---|
| Clinical Competency | 1 |
|
| Clinical Competency | 2 |
|
| Clinical Competency | 3 |
|
| Clinical Competency | 4 |
|
| Transferable Skills | 5 |
|
| Transferable Skills | 6 |
|
| Transferable Skills | 7 |
|
| Transferable Skills | 8 |
|
| Transferable Skills | 9 |
|
| Transferable Skills | 10 | “
|
| Health Systems Challenges | 11 |
|
| Health Systems Challenges | 12 |
|
| Health Systems Challenges | 13 |
|
| Health Systems Challenges | 14 |
|
| Health Systems Challenges | 15 |
|
| Health Systems Challenges | 16 |
|
| Health Systems Challenges | 17 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedicine and Dermatology Studies History · Diversity and Career in Medicine · Healthcare Systems and Technology
Introduction
The family physician’s office is commonly the first place where patients present with skin conditions, with up to one-quarter of primary care visits involving skin disorders ( Branch, Collins and Wintroub, 1983; Kerr et al., 2010).The ability of family physicians to identify and treat common dermatologic conditions has been shown to reduce wait times for referrals to specialists and increase patient satisfaction ( Chuh et al., 2005; Merenstein et al., 2007). The shortage of practicing dermatologists in Canada has been well-documented ( Chow and Searles, 2010; Heughan et al., 2008). In general, wait times for health services have increased over the last decade, with patients living in rural areas experiencing significantly longer wait times compared to their urban counterparts ( Sibley and Weiner, 2011; Yadav et al., 2016). According to a 2016 report ( Bosco and Oandasan, 2016), only 3.1% of specialists practice in rural areas in Canada.A 2018 study based in Ontario, Canada ( Micieli and Alhusayen, 2018) reported that there were 0.47 dermatologists per 100,000 people in rural areas compared to 1.96 dermatologists per 100,000 people in urban areas. There is a need for family physicians to be able to accurately diagnose and treat common dermatological problems, especially in rural communities where there are a lack of specialists.
The increasing incidence of skin conditions in an aging population have contributed to the increased demand for dermatological procedures ( Dall et al., 2013; Kosmadaki and Gilchrest, 2013). With proper training, family physicians are capable of performing diagnostic and treatment procedures in dermatology with good correlation to dermatologists ( Chuh et al., 2005; Merenstein et al., 2007). A study by Wetmore et al. (2005) presented a comprehensive list of procedures that a graduate from a Canadian family practice training program should learn and be able to perform ( Table 1). However, the time in which trainees are given to acquire these skills is limited. As such, efforts have been taken to increase the amount of education medical students receive in dermatology. A 2017 survey of medical schools across Canada ( Hu and Vender, 2018) revealed that an average of 25.6 hours of undergraduate education was dedicated to dermatology, a 25% increase in teaching time compared to 2008. Despite an increase in the average number of faculty members specializing in dermatology between 2008 and 2017, a lack of faculty was frequently cited as a barrier to allocating more teaching time to dermatology ( Hu and Vender, 2018).
There is a lack of empirical evidence on family physicians’ views towards undergraduate and postgraduate training in dermatology regarding the effectiveness of training and usefulness of these skills in practice. We set out to fill this gap in the literature through a qualitative study of recently graduated family medicine residents. The purpose of this qualitative study was to gain a first-hand account of post-graduate training in dermatology from residents that completed their Family Medicine Residency block at a family medicine clinic, where they received extra dermatology-specific training. It was expected that the results of this preliminary study would provide novel insight into post-graduate medical training with the specific intention of guiding quality improvement initiatives in the organization of family medicine residency programs.
Methods
This study employed a qualitative, phenomenological approach to data collection and analysis ( Dowling, 2007). Qualitative methodologies are increasingly popular in the field of health care because they allow for the unbiased collection and presentation of participant experiences ( Meyer, 2000). While novel findings may not be generalizable to other settings, lessons may emerge which can be used to restructure and enhance existing practice. This study was approved by the Health Sciences Research Ethics Board at Western University (Protocol #109008).
Setting
Middlesex Centre Family Medicine Clinic (MCFMC), in rural Southwestern Ontario, is an academic clinic affiliated with the Department of Family Medicine at the Schulich School of Medicine and Dentistry, Western University.
The MCFMC is a core teaching site for the regional postgraduate family medicine program at Western University, situated in Ilderton, Ontario and is staffed by six family physicians. The patients of MCFMC are primarily those who live in the rural setting and are employed in agricultural professions.
A unique educational opportunity for residents at MCFMC is the participation in ‘skin clinics’. Skin clinics are run once a week by one of the family physicians at the centre (author JH) who holds a diploma in Practical Dermatology and a focused practice designation in dermatology. This allows residents to receive additional, hands-on training in dermatology, which is not available to the majority of residents that complete their training at other Canadian family medicine clinics.
Participants and recruitment
Residents that completed their Family Medicine Residency Block at MCFMC within five years prior to the time of this study were recruited to participate in this study (n= 7). Participants were recruited by a secondary investigator (LHS) via email and provided with a letter of information and consent. Interviews continued to be scheduled until saturation was reached (when no new concepts were discovered during analysis of interviews). No compensation was provided to participants.
Interviews
A semi-structured interview guide was developed after a review of the literature, namely papers by Uzuner et al. (2010) and Bosco and Oandasan (2016), followed by discussion and consensus from all members of the research team. Each participant participated in a 1:1, semi-structured interview, conducted by a secondary investigator that had no prior relationship with or authority over the participants. Following phenomenological guidelines, the interviewer allowed the participants to guide the interview to the topics that they found relevant or skip questions that they did not find relevant ( Smith and Osborn, 2003). In keeping with the iterative nature of qualitative methods, the interview guide underwent modification during the data collection process as emerging themes led to the development of new questions and the removal of others. Interviews were guided by nine open-ended questions and related probing statements ( Figure 1).
Semi Structured Interview Guide.
Interview analysis
Audio recordings were transcribed verbatim by a transcriptionist and all identifiers were removed. Transcripts were then coded and sorted into content areas with the support of on-line analysis software (Dedoose). Each of the content areas were read in detail and summarized into emerging patterns using the qualitative principles of immersion and emergence ( Thorne, 2000). New data were compared to emerging themes from previous transcripts in an iterative and reciprocal manner ( Barnett-Page and Thomas, 2009). Field notes were reviewed and incorporated into the analysis to verify and validate findings. Themes and sub-themes were developed to reflect the most salient patterns within and across coded topic areas. This study also employed the ‘constant comparison’ method to make comparisons at each stage of the analysis to identify similarities and differences within and across interviews ( Miles and Huberman, 1994).
In order to ensure credibility and validity of the analysis, a multidimensional research team consisting of individuals with varying experiences in the analysis of the data; this supported triangulation of our findings ( Barnett-Page and Thomas, 2009). Triangulation improves validity of the results by allowing multiple perspectives to explore issues, despite the inherently different biases and strengths of those involved ( Barnett-Page and Thomas, 2009). Emerging interpretations were reviewed and challenged by the research team and discrepancies were resolved via discussion and consensus of the team ( Charmaz, 2006).
Results/Analysis
Seven residents that completed their Family Medicine Residency Block at MCFMC within five years prior to the time this study began were recruited to participate in this study ( Table 2). In total there was one male and six females. Two participants were in residency at the time of the study and the remaining five ranged from one to four years since completing their residency. Two participants were directly supervised by the special interest dermatology physician (JH) and the remaining five were supervised by other physicians at the clinic. All residents at the centre received more exposure to dermatology than residents at other Ontario centres.
From data analysis, three main themes were identified: 1) Clinical Competency 2) Transferrable Skills, and 3) Health System Challenges ( Table 3) . Quotes that illustrate each theme have been provided in Table 4.
Theme 1: Clinical Competency
The theme ‘ Clinical Competency’ includes three subthemes; confidence, comfort and satisfaction. Residents felt that their confidence in dermatology improved as a direct result of the increased training they received in dermatological procedures, whether JH was their immediate supervisor or simply available for consultation at the clinic. LY explained that her confidence was improved simply in terms of the volume of patients and procedures to which she was exposed. Another participant explained that he was more comfortable with dermatology as a result of the training. In addition, participants expressed improved personal satisfaction with their competence and abilities to treat dermatological problems.
Theme 2: Transferrable Skills
Diagnosis and treatment of dermatological problems is a complex process. Participants felt that their experiences in the clinic not only enabled them to enhance their skills, but also had them challenging themselves to diagnose before second-guessing . From a professional standpoint, the majority of participants felt that the additional training they received in dermatology made their skills transferrable to other areas of medicine. One participant felt that what they learned in clinic helped build their confidence in being able to do procedures outside of their family medicine rotations and another participant explained applying his dermatology training in the emergency room. Lastly, participants revealed the ability to provide better patient-centered care as a result of their dermatology training.
Theme 3: Health System Challenges
The third theme, ‘ Health System Challenges’, contains the sub-themes referrals, gap in Canadian healthcare, and urban/rural care. Many participants spoke of the benefit of being able to treat dermatological problems as a family physician without having to refer to a dermatologist. AO described a specific task that she was able to do that family physicians without dermatology training might not. However, many participants also expressed that they knew their limits and would still refer to a specialist as needed.Addressing gaps in the Canadian health care was a subtheme that was articulated by several participants. Many participants thought that family physicians were filling a need in the health care system by addressing dermatological problems. This was thought to be taking away some of the burden from an already taxed system. When asked how they felt about family physicians managing dermatology, a resident responded by saying that they believed it to be a good usage of resources. Of importance to some residents was how dermatological training by family physicians was addressing a need in the rural communities, given the difficulties it may cause for some patients to commute.
Discussion
Family physicians are well-positioned to treat and manage skin problems, especially in our over-burdened healthcare system ( Chuh et al., 2005; Merenstein et al., 2007). The presence of a teaching centre in Southwestern Ontario with a family physician who has a focused practice in dermatology has created a unique opportunity for family medicine residents. At this centre, residents receive additional hands-on training in dermatology and the opportunity to participate in weekly “skin clinics”. Due to the novelty of this experience, we believed gaining a first-hand account of resident experiences from the residents involved was important to better understand perceived benefits for future research and allow potential lessons to be shared more broadly.
This qualitative study revealed many positive outcomes overall. Participating residents described improvements not only in their skills in dermatology, but also in their comfort and confidence with these skills. Participants described their decreased need to refer to specialists and the subsequent benefit to patients and the overall healthcare system. Ultimately, training in this unique environment led participants to describe increased personal satisfaction and better patient-centered care.
There are several recommendations to improve practice across family medical clinics, and medical education more broadly. Firstly, the quality of dermatology training at the undergraduate levels should be improved. This should include didactic teaching as well as more opportunities for hands-on learning. Secondly, residents would benefit from increased training opportunities at the postgraduate level and continued professional development beyond this. Although dermatology teachings in Canadian medical schools has increased between 2008 and 2017, the overwhelming majority of residents are uncomfortable assessing and managing dermatological issues in patients. Providing increased clinical rotations with participation from community dermatologists and teaching of clinical skill sessions can provide a higher level of clinical exposure to residents for increased learning opportunities.Lastly, teaching centres would benefit from the increased presence of teaching physicians with speciality training.
Limitations
In part because of the small population from which to recruit from and also because of our target of residents training with family physicians practicing dermatology, we completed this study with a small sample. Although this study did reach saturation, a larger sample would have allowed a broader perspective into dermatological training in family medicine residency. Furthermore, all participants completed their family medicine residency at MCFMC, which may have led to a uniform demographic. However, clinical observations outside of the study corroborate the responses given by the participants. Future studies may benefit from conducting qualitative analyses of both residents and family physicians that completed their residency at different clinics in both rural and urban settings.
Conclusion
Dermatological diagnostic and procedural skills remain a perceived deficit by family medicine residents and physicians. This is supported by evidence for more dermatological training in medical school and residency to improve comfort with these skills to better serve patients. The intriguing initial observations from our study demonstrate that training with a family physician practicing in dermatology can elevate competency and skills in dermatological care as well as more broadly.
Take Home Messages
- •Primary care physicians with training in dermatology can help to address gaps in the healthcare system
- •Dermatological skills remain a perceived deficit by family medicine residents; there is need for more didactic teaching and hands-on learning in dermatology during residency
- •Clinical rotations with community dermatologists can help residents improve their dermatological skills and ability to provide patient-centred care
Notes On Contributors
Jessica Howard, MD, CCFP, Dip P Derm, is an Assistant Professor in the Department of Family Medicine at the Schulich School of Medicine & Dentistry, Western University in London, Ontario. Dr. Howard is a practicing family physician who holds a diploma in Practical Dermatology and a focused practice designation in dermatology.
Lauren Hayley Siegel, MSc, is the clinical faculty research coordinator for the Department of Family Medicine at the Schulich School of Medicine & Dentistry, Western University in London, Ontario.
Kelly Mok is an undergraduate student in the Department of Epidemiology & Biostatistics at Western University in London, Ontario.
Shannon Sibbald, PhD, MSc, is an Assistant Professor in the School of Health Studies, Department of Family Medicine, and Schulich Interfaculty Program in Public Health at Western University in London, Ontario. Dr. Sibbald’s interests and field of research are within interdisciplinary health and health systems research as well as implementation science ORCID ID: https://orcid.org/0000-0002-4328-6489
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barnett-Page E. and Thomas J. (2009) Methods for the synthesis of qualitative research: a critical review. BMC Medical Research Methodology. 9(1), p.59. 10.1186/1471-2288-9-59 19671152 PMC 3224695 · doi ↗ · pubmed ↗
- 2Bosco C. and Oandasan I. (2016) Review of Family Medicine Within Rural and Remote Canada: Education, Practice, and Policy. Mississauga, ON: College of Family Physicians of Canada.
- 3Branch W. T.Jr Collins M. and Wintroub B. U. (1983) Dermatologic practice: implications for a primary care residency curriculum. Journal of Medical Education. 58(2), pp.136–142. 10.1097/00001888-198302000-00007 6822984 · doi ↗ · pubmed ↗
- 4Charmaz K. (2006) Constructing grounded theory: a practical guide through qualitative analysis. Thousand Oaks, CA; SAGE.
- 5Chow E. Y. and Searles G. E. (2010) The amazing vanishing Canadian dermatologist: Results from the 2006 Canadian dermatology association member survey. Journal of Cutaneous Medicine and Surgery. 14(2), pp.71–79. 10.2310/7750.2010.09025 20338122 · doi ↗ · pubmed ↗
- 6Chuh A. A. Wong W. C. Wong S. Y. Lee A. (2005) Procedures in primary care dermatology. Australian Family Physician. 34(5), pp.347–351.15887937 · pubmed ↗
- 7Dall T. M. Gallo P. D. Chakrabarti R. West T. (2013) THE CARE SPAN: An Aging Population And Growing Disease Burden Will Require A Large And Specialized Health Care Workforce By 2025. Health Affairs. 32(11), pp.2013–2020. 10.1377/hlthaff.2013.0714 24191094 · doi ↗ · pubmed ↗
- 8Dowling M. (2007) From Husserl to, van Manen. A review of different phenomenological approaches. International Journal of Nursing Studies. 44(1), pp.131–142. 10.1016/j.ijnurstu.2005.11.026 16412442 · doi ↗ · pubmed ↗