Incidence of Postoperative Infection Following Simultaneous Bilateral Knee Arthroplasty: A Systematic Review and Meta-Analysis
Bashar Reda, Raed Sharaf

TL;DR
This study reviews infection rates after a single surgery for both knees and finds low but variable infection rates.
Contribution
The study provides pooled infection rates for simultaneous bilateral knee arthroplasty using a systematic review and meta-analysis.
Findings
Pooled prevalence of superficial infection was 0.86%.
Pooled prevalence of deep infection was 0.84%.
Significant heterogeneity was observed across all analyses.
Abstract
Total knee arthroplasty is one of the most common orthopedic procedures. Simultaneous bilateral knee arthroplasty involves performing total knee arthroplasty on both knees in a single anesthetic session. This systematic review and meta-analysis followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020. A primary search was performed using PubMed, EBSCO, Scopus, Web of Science, Clarivate, and Google Scholar databases. Quantitative data synthesis was performed using MedCalc® Statistical Software version 20.115 to determine the pooled prevalence of the infection among patients who underwent simultaneous bilateral knee arthroplasty. The Newcastle-Ottawa Scale was used to assess study quality. We included 30 studies in our quantitative data synthesis, with a total population of 118,502 patients (237,004 knees). The pooled prevalence of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
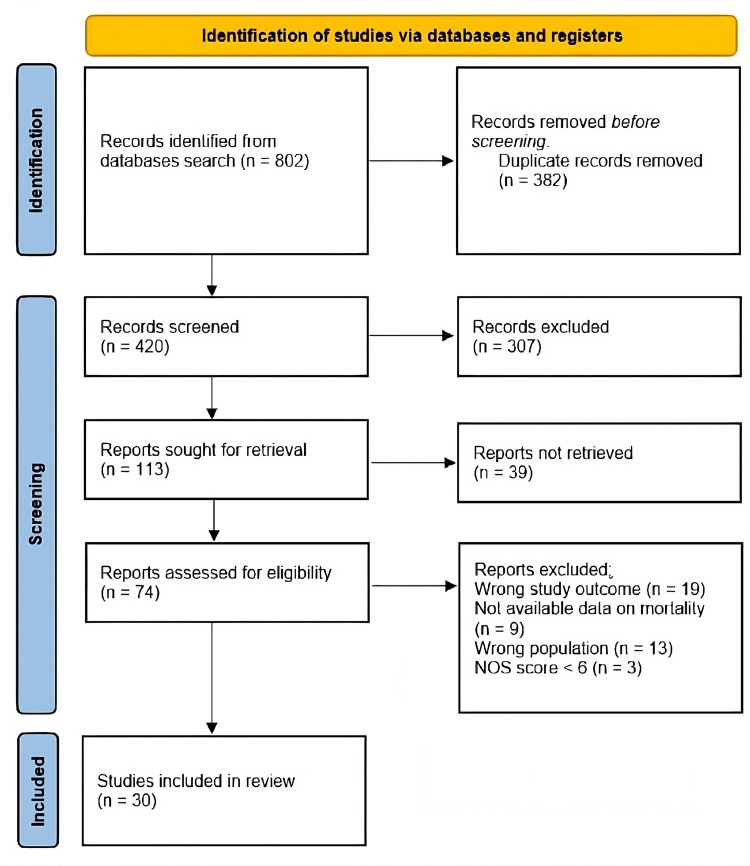 Figure 1
Figure 1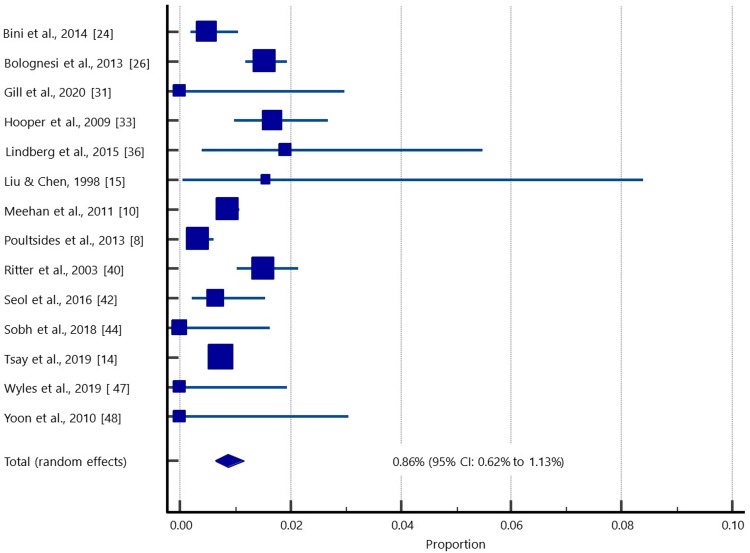 Figure 2
Figure 2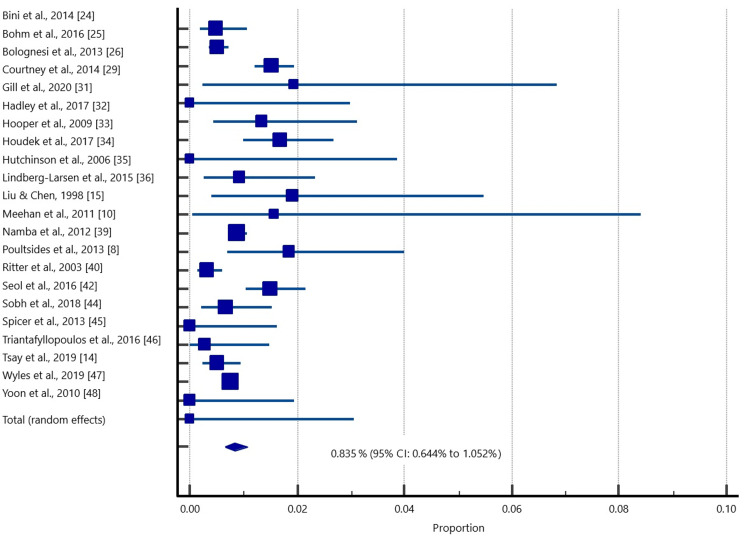 Figure 3
Figure 3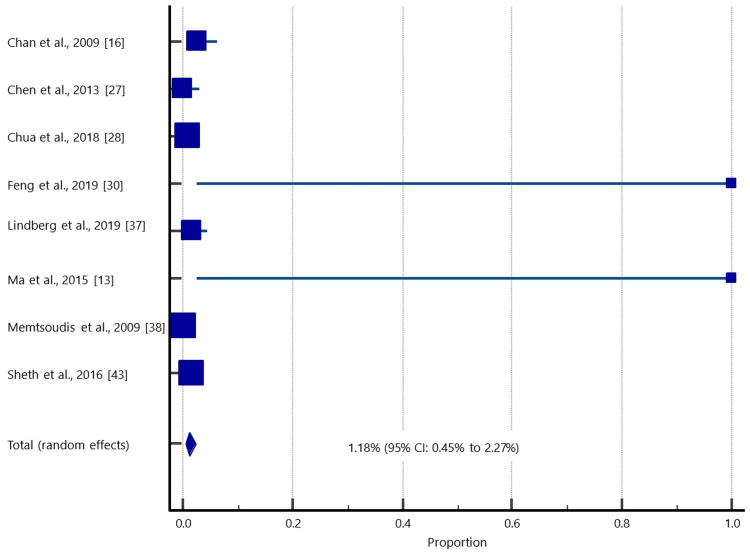 Figure 4
Figure 4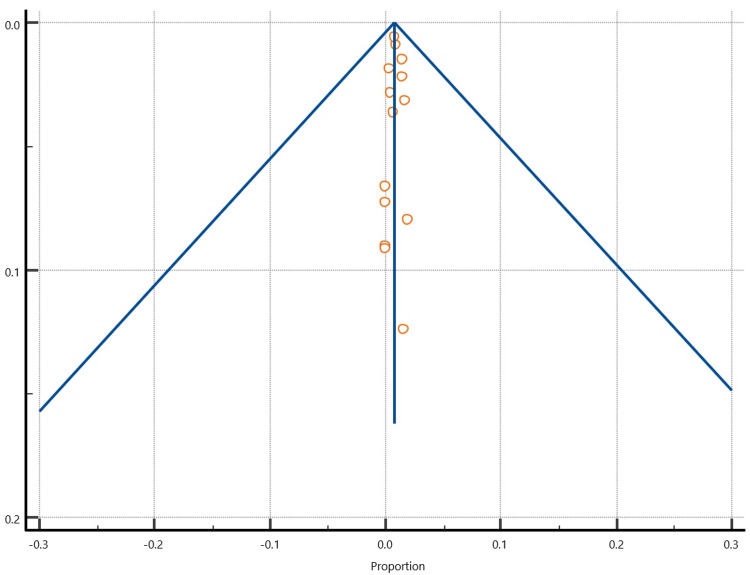 Figure 5
Figure 5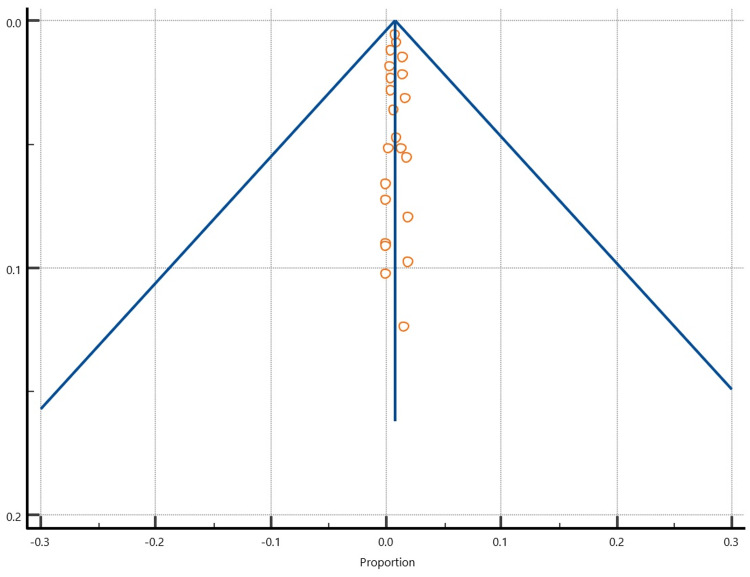 Figure 6
Figure 6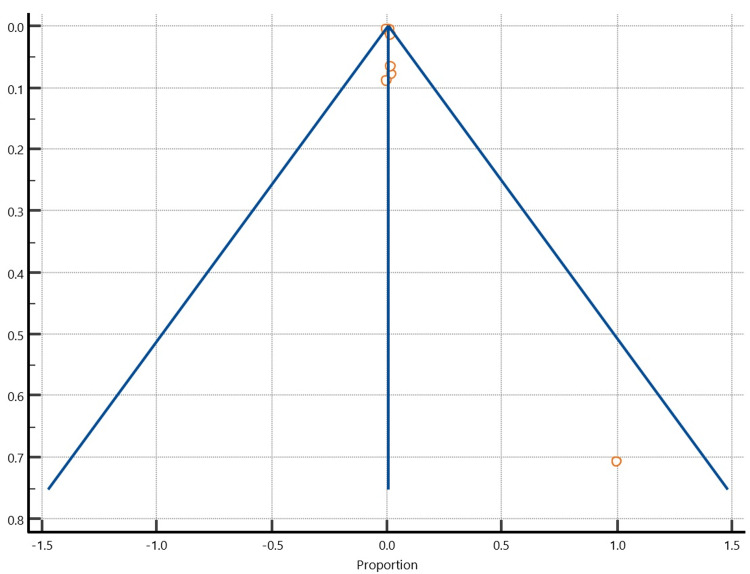 Figure 7
Figure 7| Study | Design | Country | Total population | Males (%) | Mean age, y | NOS |
| Bini et al., 2014 [ | Retrospective | USA | 1230 | 41.60% | 66 | 6 |
| Bohm et al., 2016 [ | Retrospective | Canada | 6349 | 41% | 64 | 7 |
| Bolognesi et al., 2013 [ | Retrospective | USA | 8307 | 22% | 73.3 | 6 |
| Chan et al., 2009 [ | Retrospective | UK | 159 | 57.90% | 66 | 7 |
| Chen et al., 2013 [ | Prospective | Singapore | 124 | 26.60% | 62.9 | 6 |
| Chua et al., 2018 [ | Retrospective | Australia | 23136 | 53.80% | 7 | |
| Courtney et al., 2014 [ | Retrospective | USA | 103 | 33% | 59.4 | 6 |
| Feng et al., 2019 [ | Prospective | China | 39 | 15.40% | 64.9 | 7 |
| Gill et al., 2020 [ | Retrospective | Australia | 122 | 37.70% | 70.6 | 7 |
| Hadley et al., 2017 [ | Retrospective | USA | 371 | 30% | 63.9 | 7 |
| Hooper et al., 2009 [ | Retrospective | New Zealand | 1012 | 65 | 8 | |
| Houdek et al., 2017 [ | Retrospective | USA | 94 | 57% | 52.2 | 8 |
| Hutchinson et al., 2006 [ | Prospective | Australia | 438 | 56% | 67 | 7 |
| Lindberg-Larsen et al., 2015 [ | Retrospective | Denmark | 157 | 47.10% | 64 | 7 |
| Lindberg-Larsen et al., 2019 [ | Prospective | Germany | 232 | 53.40% | 64.6 | 8 |
| Liu & Chen, 1998 [ | Retrospective | China | 64 | 5% | 66.7 | 6 |
| Ma et al., 2015 [ | Retrospective | China | 36 | 41.70% | 65.6 | 7 |
| Meehan et al., 2011 [ | Retrospective | USA | 11445 | 46.10% | 67.2 | 8 |
| Memtsoudis et al., 2009 [ | Retrospective | USA | 25179 | 66 | 7 | |
| Namba et al., 2012 [ | Retrospective | USA | 324 | 7 | ||
| Poultsides et al., 2013 [ | Retrospective | USA | 2825 | 37.60% | 65.2 | 8 |
| Ritter et al., 2003 [ | Retrospective | USA | 2050 | 44.20% | 69.9 | 6 |
| Seo JG et al., 2014 [ | Retrospective | South Korea | 420 | |||
| Seol et al., 2016 [ | Retrospective | South Korea | 759 | 5.70% | 68.3 | 7 |
| Sheth et al., 2016 [ | Retrospective | USA | 3933 | 42.70% | 64.9 | 8 |
| Sobh et al., 2018 [ | Retrospective | USA | 225 | 48% | 61 | 6 |
| Spicer et al., 2013 [ | Retrospective | Canada | 373 | 29% | 69.1 | 7 |
| Triantafyllopoulos et al., 2016 [ | Retrospective | USA | 1808 | 51% | 56.3 | 8 |
| Tsay et al., 2019 [ | Retrospective | USA | 27301 | 43.20% | 65.8 | 8 |
| Wyles et al., 2019 [ | Retrospective | USA | 188 | 42% | 61 | 8 |
| Yoon et al., 2010 [ | Retrospective | South Korea | 119 | 5.90% | 70 | 7 |
| Study | Sample size | Proportion (%) | 95% CI | Weight (%) |
|
Bini et al., 2014 [ | 1230 | 0.488 | 0.179 to 1.059 | 8.98 |
|
Bolognesi et al., 2013 [ | 4519 | 1.527 | 1.190 to 1.928 | 12.2 |
|
Gill et al., 2020 [ | 122 | 0 | 0.000 to 2.978 | 2.1 |
|
Hooper et al., 2009 [ | 1012 | 1.68 | 0.982 to 2.676 | 8.33 |
|
Lindberg-Larsen et al 2015 [ | 157 | 1.911 | 0.396 to 5.483 | 2.59 |
|
Liu & Chen, 1998 [ | 64 | 1.562 | 0.0396 to 8.401 | 1.2 |
|
Meehan et al., 2011 [ | 11445 | 0.874 | 0.711 to 1.062 | 13.28 |
|
Poultsides et al., 2013 [ | 2825 | 0.319 | 0.146 to 0.604 | 11.29 |
|
Ritter et al., 2003 [ | 2050 | 1.512 | 1.030 to 2.140 | 10.5 |
|
Seol et al., 2016 [ | 759 | 0.659 | 0.214 to 1.531 | 7.33 |
|
Sobh et al., 2018 [ | 225 | 0 | 0.000 to 1.626 | 3.43 |
|
Tsay et al., 2019 [ | 27301 | 0.755 | 0.655 to 0.864 | 13.74 |
|
Wyles et al., 2019 [ | 188 | 0 | 0.000 to 1.943 | 2.99 |
|
Yoon et al., 2010 [ | 119 | 0 | 0.000 to 3.052 | 2.06 |
| Total (random effects) | 52016 | 0.857 | 0.620 to 1.132 | 100 |
| Study | Sample size | Proportion (%) | 95% CI | Weight (%) |
| Bini et al., 2014 [ | 1230 | 0.488 | 0.179 to 1.059 | 6.13 |
| Bohm et al., 2016 [ | 6349 | 0.504 | 0.345 to 0.711 | 8.85 |
| Bolognesi et al., 2013 [ | 4519 | 1.527 | 1.190 to 1.928 | 8.49 |
| Courtney et al., 2014 [ | 103 | 1.942 | 0.236 to 6.839 | 1.2 |
| Gill et al., 2020 [ | 122 | 0 | 0.000 to 2.978 | 1.38 |
| Hadley et al., 2017 [ | 371 | 1.348 | 0.439 to 3.117 | 3.26 |
| Hooper et al., 2009 [ | 1012 | 1.68 | 0.982 to 2.676 | 5.67 |
| Houdek et al., 2017 [ | 94 | 0 | 0.000 to 3.848 | 1.1 |
| Hutchinson et al., 2006 [ | 438 | 0.913 | 0.249 to 2.322 | 3.64 |
| Lindberg-Larsen et al., 2015 [ | 157 | 1.911 | 0.396 to 5.483 | 1.71 |
| Liu & Chen, 1998 [ | 64 | 1.562 | 0.0396 to 8.401 | 0.78 |
| Meehan et al., 2011 [ | 11445 | 0.874 | 0.711 to 1.062 | 9.29 |
| Namba et al., 2012 [ | 324 | 1.852 | 0.683 to 3.987 | 2.97 |
| Poultsides et al., 2013 [ | 2825 | 0.319 | 0.146 to 0.604 | 7.81 |
| Ritter et al., 2003 [ | 2050 | 1.512 | 1.030 to 2.140 | 7.24 |
| Seol et al., 2016 [ | 759 | 0.659 | 0.214 to 1.531 | 4.96 |
| Sobh et al., 2018 [ | 225 | 0 | 0.000 to 1.626 | 2.28 |
| Spicer et al., 2013 [ | 373 | 0.268 | 0.00679 to 1.485 | 3.28 |
| Triantafyllopoulos et al., 2016 [ | 1808 | 0.498 | 0.228 to 0.943 | 6.98 |
| Tsay et al., 2019 [ | 27301 | 0.755 | 0.655 to 0.864 | 9.64 |
| Wyles et al., 2019 [ | 188 | 0 | 0.000 to 1.943 | 1.98 |
| Yoon et al., 2010 [ | 119 | 0 | 0.000 to 3.052 | 1.36 |
| Total (random effects) | 61876 | 0.835 | 0.644 to 1.052 | 100 |
| Study | Sample size | Proportion (%) | 95% CI | Weight (%) |
| Chan et al., 2009 [ | 159 | 2.516 | 0.690 to 6.316 | 12.25 |
| Chen et al., 2013 [ | 124 | 0 | 0.000 to 2.931 | 10.98 |
| Chua et al., 2018 [ | 23136 | 1.042 | 0.915 to 1.181 | 20.81 |
| Feng et al., 2019 [ | 1 | 100 | 2.500 to 100.000 | 0.36 |
| Lindberg-Larsen et al., 2019 [ | 232 | 1.724 | 0.472 to 4.355 | 14.08 |
| Ma et al., 2015 [ | 1 | 100 | 2.500 to 100.000 | 0.36 |
| Memtsoudis et al., 2009 [ | 25179 | 0.147 | 0.103 to 0.202 | 20.82 |
| Sheth et al., 2016 [ | 3933 | 1.602 | 1.233 to 2.045 | 20.33 |
| Total (random effects) | 52765 | 1.182 | 0.445 to 2.265 | 100 |
| Parameter | Superficial infection | Deep infection | Unspecified |
| Q chi2 | 62.1893 | 82.3301 | 275.0070 |
| DF {degrees of freedom} | 13 | 21 | 7 |
| Significance level | P < 0.0001 | P < 0.0001 | P < 0.0001 |
| I2 (inconsistency) | 79.10% | 74.49% | 97.45% |
| 95% CI for I2 | 65.58 to 87.30 | 61.31 to 83.18 | 96.34 to 98.23 |
| Egger's test | |||
| Intercept | 0.06168 | 0.1816 | 2.9529 |
| 95% CI | -1.8137 to 1.9371 | -1.0893 to 1.4525 | -4.0700 to 9.9759 |
| Significance level | P = 0.9441 | P = 0.7687 | P = 0.3432 |
| Begg's test | |||
| Kendall's Tau | 0.03297 | 0.09091 | 0.03704 |
| Significance level | P = 0.8695 | P = 0.5537 | P = 0.8979 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Orthopedic Infections and Treatments · Orthopaedic implants and arthroplasty
Introduction and background
The frequency of performing total knee arthroplasty (TKA) surgeries is constantly increasing in developed nations with an aging population and increasing obesity. The National Joint Registry (NJR) documented 102,177 primary knee replacement procedures in 2017, an increase of 3.7% from 2015. Additionally, 96.2% of these procedures were performed on patients with osteoarthritis. According to a data analysis conducted by the NJR and the Office of National Statistics, primary TKAs in England and Wales will increase by 117% between 2012 and 2030. Typically, 75-85% of patients report being satisfied (or "very satisfied") with the results of their surgeries, whereas the remaining 15.25% were dissatisfied (or "very dissatisfied) [1].
Interestingly, the satisfaction level after TKA is much lower than that after total hip arthroplasty, which emphasizes the necessity for additional investigation into the causes behind this [2,3]. Patient satisfaction might vary for various reasons and depends on the techniques used to evaluate the results, the preoperative expectations of the patients, or the general preoperative state. As it is convenient for surgeons, the National Health Service progression reports on TKA are now based on the results reported by the patients using the Oxford Knee Score. The approaches utilized after TKA for the same are outlined in the following section, along with their benefits and drawbacks.
Bilateral knee joint symptoms are common in individuals with severe end-stage degenerative joint disease and require joint replacement in both knees [4,5]. These patients have three surgical options: bilateral arthroplasty utilizing one surgical team while the patient is under anesthesia, simultaneous arthroplasty of both knees using two surgical teams, and staged surgery with a set duration between the two surgeries. However, there is disagreement about whether bilateral knee arthroplasty should be conducted simultaneously or in stages [6].
TKA is a safe and successful procedure, although periprosthetic joint infection (PJI), deep infections, and other postoperative sequelae remain major issues. PJI plays a significant role in implant failure and revision arthroplasty [7]. Compared to unilateral operations, simultaneous bilateral knee arthroplasty (simBTKA) is associated with a longer duration of hospital stay. The development of deep infections has been reported to predispose patients to longer operating times [8]. However, as of now, the results of previous studies examining the impact of simBTKA on PJIs have been inconsistent [9-11]. Therefore, it is still crucial to determine if these longer operations have a higher incidence of infection problems than staged and unilateral arthroplasties. Therefore, with this meta-analysis, we aimed to estimate the burden of postoperative infections following simBTKA.
This systematic review and meta-analysis were conducted in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines [12].
The search strategy for these studies was compiled using searches of PubMed, EBSCO, Scopus, and Web of Science through Clarivate and Google Scholar databases. We searched databases using keywords, MeSH terms, and the Boolean operators AND and OR. The search keywords included bilateral total knee arthroplasty, bilateral TKA, knee replacement, knee arthroplasty, infect, sepsis, SSI, surgical site infection, deep infection, superficial infection, simultaneous, simultaneous BTKA, single anesthetic, and simBTKA. In addition to database searches, we manually searched for articles via Google. Since TKA was first identified in the 1970s and 1980s, no language constraints were used, and publications from January 1970 to the present were searched.
Three writers assessed the titles, abstracts, and full texts of the findings to assess whether the search results fulfilled the criteria for inclusion in this systematic review. Conflicts between the two authors were resolved by discussion with the third author or by reaching an agreement. An email was used to contact the authors of the publications if further information on potential studies was required. All information relevant to the research subject was obtained from the included articles and entered into Microsoft Excel (Microsoft Corp., Redwood City, Calif., USA).
The Rayyan Intelligent Systematic Reviews website was used to manage the primary search results and eliminate duplicates. After performing title, abstract, and full-text screening, Microsoft Excel was used to extract data from the included studies.
The quality of the studies was assessed by two authors using the Newcastle-Ottawa Scale (NOS). The values for the quality evaluation items ranged from 0 to 9. A study was considered high quality if it earned seven or more.
For quantitative data synthesis, MedCalc® Statistical Software version 20.115 (MedCalc Software Ltd., 2022) was used. Data on superficial, deep, and unspecified infections were included in a proportional random effects meta-analysis, on which forest and funnel plots were constructed. The proportion of inter-study heterogeneity was measured using Higgin's I2 test, with a cut-off threshold for considerable heterogeneity set at I2>50%. Funnel plots were used to visually analyze publication bias with a cut-off point of a p-value of 0.1 or less.
Review
Results
In total, 802 studies were identified by using the aforementioned electronic databases. The exclusion of 382 studies due to duplicate detection and removal left 420 studies available for enrollment during the title and abstract screening. After screening titles and abstracts, 307 studies were eliminated. Thirty studies were included in the analysis after the full texts of the remaining 74 studies were evaluated. The search and study selection procedures are summarized in Figure 1.
PRISMA flow chart summarizing the search and screening processes
Characters of the included studies
After completing the search and screening of the primarily extracted studies, 30 studies were finally included for quantitative data synthesis: 8, 10, 13, 14, 15, 16, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 42, 43, 44, 45, 46, 47, 48. Twelve of the included studies were conducted in the USA: 8, 10, 14, 24, 26, 29, 32, 34, 38, 39, 40, 43, 44, 46, and 47. As shown in Table 1, the total population of each study ranged from 36 patients [13] to 27,301 patients [14], whereas the overall total population was 118,502 patients (237,004 knees). The proportion of males ranged from 5% to 57.9% [15-17] . The safety of simBTKA has been thoroughly investigated [18-20]. Additionally, complications such as infection, in addition to costs compared to anesthesia once or twice [21-23].
Superficial infection following simBTKA
Data from 52,016 patients (104,032 knees) were enrolled for quantitative data synthesis to estimate the pooled prevalence of superficial infection following simBTKA (Table 2; Figure 2). The pooled prevalence of superficial infection was estimated to be 0.86% (95% confidence interval [CI]: 0.62%-1.13%).
A forest plot showing the pooled superficial infection rate in patients who underwent simBTKA
Deep infection following simBTKA
For quantitative data synthesis to determine the pooled prevalence of deep infection following simBTKA, data from 61,876 patients (123,752 knees) were used (Table 3; Figure 3). The estimated overall prevalence of deep infection was 0.84% (95%, CI: 0.64%-1.05%).
A forest plot showing the pooled deep infection rate in patients who underwent simBTKA
Unspecified surgical site infection (SSI) rates
Eight studies did not specify the type of infection. Data comprising 52,765 patients (105,530 knees) were used to estimate the pooled prevalence of infection (Table 4; Figure 4), which was found to be 1.18% (95%, CI: 0.45%-2.27%).
A forest plot showing the pooled unspecified SSI rate in patients who underwent simBTKA
Test for heterogeneity and publication bias
There was significant heterogeneity (I2>50%) in all analyses (Table 5). Visual inspection of funnel plots to detect publication bias (Figures 5-7) reveals a symmetrical distribution of the plotted data.
A funnel plot showing the symmetrical distribution of the plotted superficial infection data
A funnel plot showing the symmetrical distribution of the plotted deep infection data
A funnel plot showing the symmetrical distribution of the plotted deep infection data
Discussion
The benefits of bilateral TKA performed under a single anesthetic regimen over bilateral arthroplasty performed in two stages include encouraging symmetrical rehabilitation of both knees, limiting invasive surgical procedures and anesthesia to a single event, possibly reducing the length of hospital stay, and, consequently, hospital costs related to TKA [4,5,17].
Our study aimed to estimate the prevalence of SSI following simBTKA by systematically reviewing current publications with relevant data. After a thorough screening, 30 studies were included in our meta-analysis, with a total population of 118,502 patients (237,004 knees). The pooled prevalence of superficial infection, deep infection, and unspecified SSI was estimated to be 0.86% (95%, CI: 0.62-1.13%), 0.84% (95%, CI: 0.64-1.05%), and 1.18% (95%, CI: 0.45-2.27%), respectively. There was significant heterogeneity (I2 > 50%) in all analyses. Furthermore, inspecting funnel plots revealed a symmetrical distribution of plotted data.
The safety of simBTKA has been thoroughly investigated by Malahias et al. [18] and a meta-analysis by Liu et al. [19]. According to Malahias et al., there is some evidence that simBTKA is just as safe as staged BTKA (staBTKA) in trials with patients with similar baseline demographics [18].
Upon comparing simBTKA with staBTKA, some studies have found fewer complications, such as infections, with simBTKA having lower rates of infection than staBTKA [8,20]. This finding is partially consistent with that of a recent meta-analysis that found that superficial infections occurred more frequently after staBTKA than after single anesthetic BTKA; however, periprosthetic infections occurred at similar rates [21]. The majority of single-anesthetic BTKA studies, however, do not differentiate between simBTKA and staBTKA; therefore, it is impossible to assume that the results and costs of both treatments will be similar [22]. As a result, few of these studies have provided sufficient data to compare the complication rates of simBTKA and staBTKA.
It is essential, however, to recognize that a staged operation postpones the full advantages of bilateral TKA until after the completion of both procedures. Additionally, when TKA is performed using a staged approach, a painful contralateral knee makes effective postoperative rehabilitation more challenging in patients with bilateral knee osteoarthritis and substantial flexion contractures. Increased stress in the contralateral knee after TKA is, therefore, believed to accelerate the development of osteoarthritis in the knee [23].
Recommendations
We recommend that further studies be conducted to provide higher-quality evidence to assess infection rates in simBTKA and its trends.
Conclusions
From this meta-analysis, we reveal that the rates of infection following simBTKA are relatively low but heterogeneous, as the data shows marked variability. Superficial infections were more common than deep infections; however, there was a small difference in their prevalence. However, since the reliability of our findings was limited owing to the significant heterogeneity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Joint Registry for England, Wales and Northern Ireland. 14th Annual Report Wales N 2882017 https://www.hqip.org.uk/resource/national-joint-registry-14th-annual-report-2017/
- 2Total knee arthroplasty in younger patients evaluated by alternative outcome measures J Arthroplasty Klit J Jacobsen S Rosenlund S Sonne-Holm S Troelsen A 9129172920142426909710.1016/j.arth.2013.09.035 · doi ↗ · pubmed ↗
- 3The John Insall Award: Patient expectations affect satisfaction with total knee arthroplasty Clin Orthop Relat Res Noble PC Conditt MA Cook KF Mathis KB 354345220061696703510.1097/01.blo.0000238825.63648.1e · doi ↗ · pubmed ↗
- 4Safety and efficacy of bilateral total knee arthroplasty J Arthroplasty Cohen RG Forrest CJ Benjamin JB 497502121997926878810.1016/s 0883-5403(97)90171-6 · doi ↗ · pubmed ↗
- 5Bilateral total knee replacement under one anesthetic Clin Orthop Relat Res Gradillas EL Volz RG 81531979 https://journals.lww.com/corr/Citation/1979/05000/Bilateral_Total_Knee_Replacement_Under_One.28.aspx 477067 · pubmed ↗
- 6Simultaneous and staged bilateral total knee arthroplasty J Bone Joint Surg Am Hardaker WT Jr Ogden WS Musgrave RE Goldner JL 247250601978 https://europepmc.org/article/med/641093641093 · pubmed ↗
- 7Total joint arthroplasties: current concepts of patient outcomes after surgery Rheum Dis Clin North Am Jones CA Beaupre LA Johnston DW Suarez-Almazor ME 71863320071736769310.1016/j.rdc.2006.12.008 · doi ↗ · pubmed ↗
- 8Infection following simultaneous bilateral total knee arthroplasty J Arthroplasty Poultsides LA Memtsoudis SG Vasilakakos T 92952820132393792010.1016/j.arth.2013.07.005 · doi ↗ · pubmed ↗