Characteristics and Outcomes of Stem Cell Transplant Patients during the COVID-19 Era: A Systematic Review and Meta-Analysis
Mona Kamal, Massimo Baudo, Jacinth Joseph, Yimin Geng, Omnia Mohamed, Mohamed Rahouma, Uri Greenbaum

TL;DR
This study reviews outcomes of stem cell transplant patients during the COVID-19 pandemic, finding high rates of severe illness and mortality.
Contribution
The study provides pooled event rates for severe outcomes and treatment use in stem cell transplant patients with COVID-19.
Findings
Stem cell transplant patients had a 21.1% pooled event rate for COVID-19-related deaths.
Hospital admissions for these patients reached 55.2%.
Dexamethasone improved survival in hospitalized patients with moderate to severe COVID-19.
Abstract
This systematic review and meta-analysis aims to identify the outcomes of stem cell transplant (SCT) patients during the COVID-19 era. Pooled event rates (PER) were calculated, and meta-regression was performed. A random effects model was utilized. In total, 36 eligible studies were included out of 290. The PER of COVID-19-related deaths and COVID-19-related hospital admissions were 21.1% and 55.2%, respectively. The PER of the use of hydroxychloroquine was 53.27%, of the receipt of immunosuppression it was 39.4%, and of the use of antivirals, antibiotics, and steroids it was 71.61%, 37.94%, and 18.46%, respectively. The PER of the time elapsed until COVID-19 infection after SCT of more than 6 months was 85.3%. The PER of fever, respiratory symptoms, and gastrointestinal symptoms were 70.9, 76.1, and 19.3%, respectively. The PER of acute and chronic GvHD were 40.2% and 60.9%,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
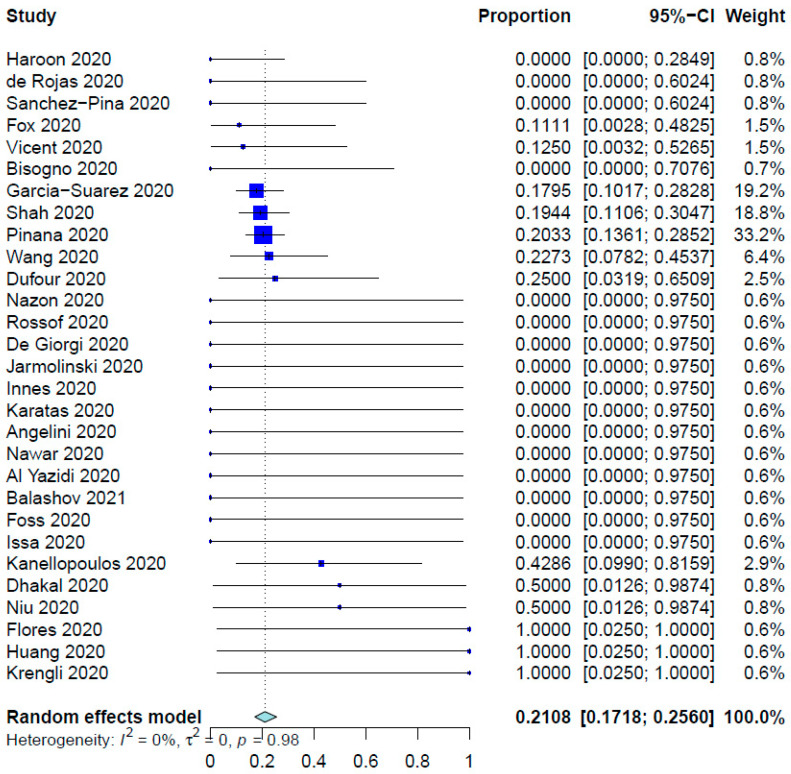 Figure 1
Figure 1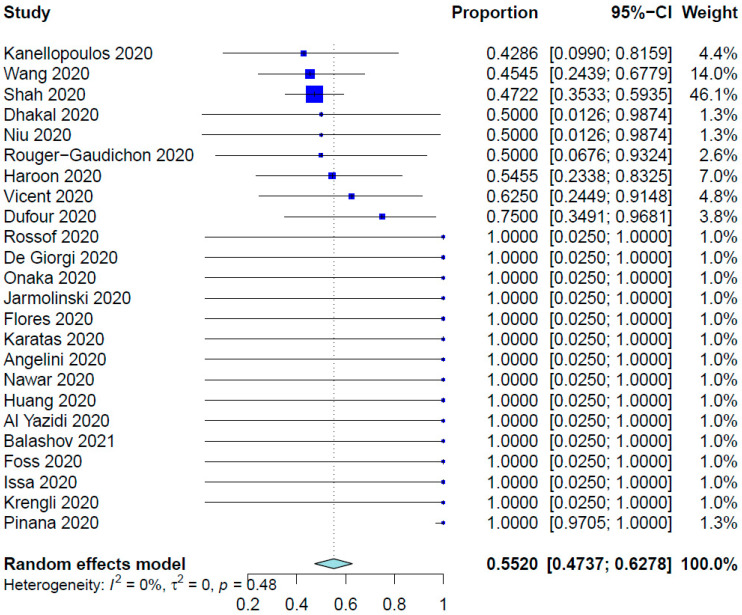 Figure 2
Figure 2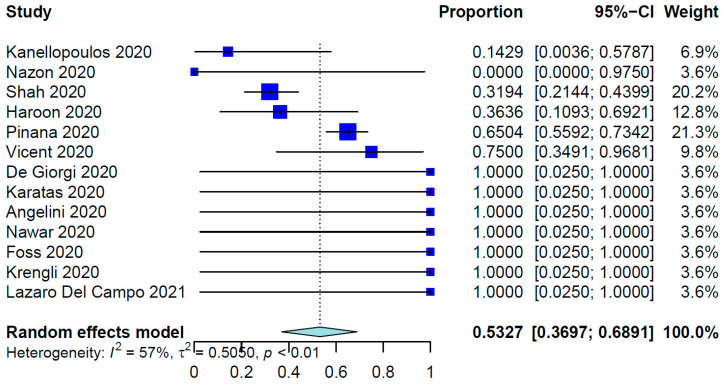 Figure 3
Figure 3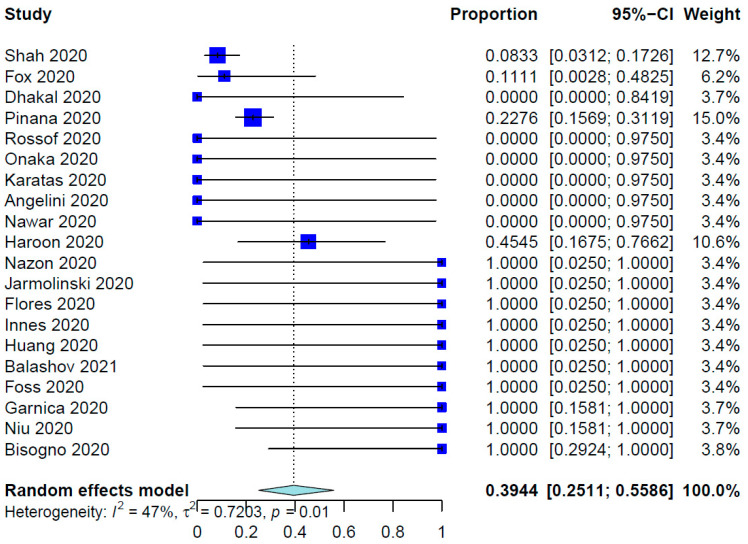 Figure 4
Figure 4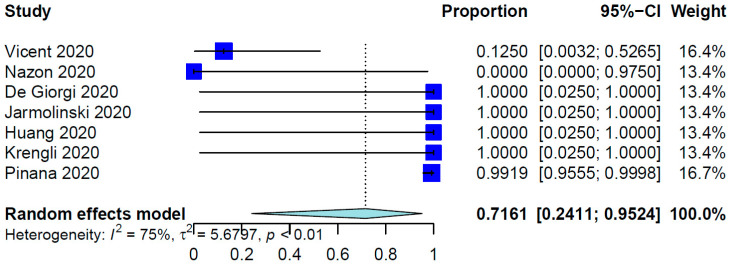 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · COVID-19 Clinical Research Studies · Hematopoietic Stem Cell Transplantation
1. Introduction
Preparation for safe effective bone marrow transplantation (BMT) for hematological cancers in the era of COVID-19 starts as early as the pre-transplantation screening phase [1]. During the management of BMT candidates, identification of carriers of COVID-19, and close monitoring of high-risk patients for early diagnosis of infection, with prompt clinical management of highly suspicious cases with false-negative results, are vitally important as part of effective clinical care. In addition, special considerations for infection prevention are raised before, during, and after BMT: psychological aspects, limitations on providers availability, availability of healthy donors, travel to BMT centers, and separation of patients from family, especially in the pediatric population [2,3,4,5,6].
The infectious diseases working parties of the American Society for Transplantation and Cellular Therapy and The European Society for Blood and Marrow Transplantation collaborated to overcome medical challenges during the COVID-19 era and optimize clinical care for stem cell transplantation (SCT) recipients. This much-needed effort encourages transplantation centers to continuously collect patient data and outcomes, initiates educational activities for providers, patients, and caregivers, and issues updated recommendations [7,8,9,10,11,12].
Recently, the number of bone marrow transplants has risen, and their outcomes have improved. This may be attributed to a sustained reduction in the rates of new COVID-19 cases; increased availability of vaccines, personal protective equipment, and trained staff; increased testing capacity; and adherence to social distancing, telemedicine visits, and patient education [2,5,13,14,15,16]. All of these factors also help the performance of BMT in urgent cases by reducing the burden on providers. Despite these efforts, SCT-related clinical care varies across institutions (guided by community prevalence and availability of infrastructure, personal protective equipment, and trained staff). At the early stages of the pandemic, some centers used unapproved agents for COVID-19 treatment based on new data that emerged almost daily, albeit from nonrandomized trials and after short follow-up times [2,12,17]. Additionally, clinical trial recruitment must still be improved as it has been compromised during the COVID-19 pandemic [18,19]. Furthermore, COVID-19 infection manifests in a wide range of symptoms that differ in profile and severity [20] and the published data regarding the clinical care and patients’ characteristics and outcomes during and after BMT are heterogeneous [4,21].
To date, there are no consensus guidelines as to the management of COVID-19 infections in the setting of pre- and post-BMT care. This systematic review and meta-analysis summarizes available data from studies addressing the impact of COVID-19 on BMT recipients to better guide precision care for these patients and overcome challenges in the transplantation setting. Such data are critical for patient prioritization and safety as well as enhancing multidisciplinary teamwork to improve clinical outcomes, reduce the burden on providers, and optimize the selection of alternative care plans and therapies as well as the use of medical resources [22,23].
2. Materials and Methods
This systematic review/meta-analysis was conducted according to the preferred reporting items for systematic reviews and meta-analyses guidelines [24].
2.1. Literature Search Engines and Terms Used
The MEDLINE (Ovid, New York, NY, USA), Embase (Ovid), Web of Science (Clarivate, London, UK), PubMed, and Cochrane Library (John Wiley & Sons, Hoboken, NJ, USA) databases were searched for publications in the English language from 1 December 2019 to 1 January 2021. The following search terms were used, with subject headings and keywords searched as needed: COVID-19, severe acute respiratory syndrome coronavirus 2, SARS-CoV-2, coronavirus infections, novel coronavirus, cancer, neoplasms, tumor, leukemia, lymphoma, melanoma, carcinoma, sarcoma, oncology, stem cell transplantation, bone marrow transplantation, etc. The search terms were combined with “or” if they represented similar concepts or combined with “and” if they represented different concepts. The complete search strategies are detailed in Supplementary Tables S1–S4.
2.2. Study Types Selected and Inclusion Criteria
The initial search included original studies (case reports, case series, and observational studies) as well as all types of editorials if they included enough patient-related clinical information owing to the rarity of the data. This is due to the rapid reporting during the COVID-19 pandemic, with some authors reporting valuable data in editorials, letters, comments, and conference papers. Eligible studies were required to address the following measurable outcomes in patients with hematological cancers who underwent BMT during the COVID-19 pandemic: rate of COVID-19 infection, emergency room visits, intensive care unit admission, hospital readmission, complications, thromboembolic events, need for supplemental oxygen therapy, need for invasive ventilation, fungal and other opportunistic infections, reinfection with COVID-19, and overall survival. We excluded other types of publications, including review articles, guidelines, experience, consensus, and abstracts. The Joanna Briggs Institute Critical Appraisal tools’ Checklist for Case Reports and Case Series and the Newcastle–Ottawa Quality Assessment Scale for Cohort Studies were used for the critical appraisal and quality assessment of the included papers [13,25,26], Supplementary Table S5.
2.3. Data Extraction and Statistical Analysis
Excel software (Microsoft, v11.0, Redmond, WA, USA) was used for data extraction. Categorical variables were expressed as frequencies, whereas continuous variables were reported as mean (± SD) values. The following patient variables were extracted from the included articles: age, sex, comorbidities, previous treatment, disease type, type of SCT, timing of SCT, timing of COVID-19 infection, treatment received for COVID-19, treatment delay or interruption owing to COVID-19, presence of graft-versus-host disease (GvHD), type of GvHD (acute or chronic), receipt of immunosuppressive agents (e.g., tacrolimus and sirolimus) at the time of COVID-19 diagnosis, and receipt of steroids at the time of COVID-19 diagnosis. Two investigators performed data extraction independently.
Pooled event rates (PERs) with 95% CIs were calculated. The inverse of the variance in the estimate was estimated using the DerSimonian–Laird method with a random effects model. Studies with double zeros were included in our meta-analysis and treatment arm continuity correction was applied in studies with zero-cell frequencies.
Hypothesis testing for equivalence was set at a two-tailed p-value of 0.05. Determining the heterogeneity was based on Cochran’s Q test with I^2^ values. In the case of heterogeneity (I^2^ > 50%), individual study inference analysis was performed via leave-one-out sensitivity analysis.
Funnel plots by graphical inspection and the Egger regression test were used for the assessment of publication bias. In the case of asymmetry positivity, visual assessment and Duval and Tweedie’s trim-and-fill methods were performed.
All analyses were performed using the R computing language (version 4.1.0) and RStudio application (version 1.4.1717) with the meta and metafor packages.
3. Results
A total of 290 studies were identified in the databases. After the exclusion of duplicate articles, 208 studies were screened, excluding 151 studies that were not eligible. This left 57 full-text articles to be assessed for eligibility. Thirty-six of these studies met our eligibility criteria [16,21,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60]. These studies included a total of 2011 patients, 516 of whom underwent SCT. Of these patients, 409 were diagnosed with COVID-19 after SCT. Supplementary Figure S1 shows a flow diagram of the preferred reporting items for systematic reviews and meta-analyses guidelines. Table 1 shows the study characteristics and patient demographics. The weighted mean (±SD) age of all SCT patients was 42.1 ± 22.4 years (only 23 articles mentioned patient ages). The weighted percentage of male patients was 61.25% (only 22 articles mentioned patient sex data).
A subgroup analysis was performed to describe the characteristics of the allogenic SCT patients. A mean age of 35.6 ± 23.9 (reported in 15/18 studies) in 104 allogeneic SCT patients was reported; those patients were predominately males (58.0%) (58/100) (reported in 14/18 studies). Matched unrelated, matched related, and haplo-identical (half-matched) donors represented 42.9% (33/77) (reported in 12/18 studies), 38.6% (32/88) (reported in 12/18 studies), and 30.3% (27/89) (reported in 12/18 studies) of allogenic SCT patients in the included studies, respectively. The infection rate in allogenic SCT patients was 93%.
For all SCT patients included in these studies, the COVID-19 infection rate was 79.23%. The mean time from SCT to COVID-19 infection was 10.01 months (95% CI, 8.26–12.14 months; data derived from 24 studies and 333 patients), whereas the range was 6.0 days to 86.4 months. Table 2 shows the outcomes of the meta-analysis. The pooled COVID-19-related mortality was 21.08% (95% CI, 17.18–25.60%) (Figure 1) and that for COVID-19-related hospital admission was 55.20% (95% CI, 47.37–62.78%) (Figure 2). The PER for the use of hydroxychloroquine was 53.27% (95% CI, 36.97–68.91%) (Figure 3). The PER for receipt of immunosuppressive agents was 39.44% (95% CI, 25.11–55.86%) (Figure 4 and Figure 5). Supplementary Figures S2 and S3 show the PERs for the use of antivirals (71.61%), antibiotics (37.94%), and steroids (18.46%). As shown in Supplementary Figure S4, the PERs for the timing of COVID-19 infection varied among all SCT patients diagnosed with COVID-19 within the first 100 days (39%), 100 days to 6 months (34%), and more than 6 months (85%) after SCT. The PER for fever as a presenting symptom was 70.89% (95% CI, 64.22–76.78%). The PER for respiratory symptoms as a presenting symptom was 76.14% (95% CI, 57.31–88.36%). The PER for acute GvHD was 40.20% (95% CI, 11.80–77.16%), whereas that for chronic GvHD was 60.91% (95% CI, 25.39–87.70%).
In a meta-regression analysis (Table 3), we sought to determine whether any of the following factors influenced the risk of COVID-19-related mortality in all included SCT patients: time to COVID-19 infection after SCT, presence of GvHD and its type, use of immunosuppression agents, use of steroids, use of hydroxychloroquine, use of antibiotics, use of antivirals, and hospital admission. We found that none of these factors significantly influenced the rate of COVID-19-related mortality after SCT.
In a meta-regression analysis (Table 3), we sought to determine whether any of the following factors influenced the risk of COVID-19–related mortality in all included SCT patients: time to SARS-CoV-2 infection after SCT, presence of GvHD and its type, use of immunosuppression agents, use of steroids, use of hydroxychloroquine, use of antibiotics, use of antivirals, and hospital admission. We found that none of these factors significantly influenced the rate of COVID-19–related mortality after SCT.
4. Discussion
The COVID-19 pandemic has brought challenges to the management of SCT recipients. Transplant recipients are immunocompromised and have an increased risk of severe COVID-19 infection and mortality. Therefore, deciding to proceed with SCT during the pandemic requires careful consideration of the benefits and risks. This meta-analysis provides essential information that can help clinical decisions toward the optimization of SCT recipients’ care during the pandemic. Herein, we summarize the available data from studies that addressed the impact of COVID-19 infection on SCT recipients.
As described above, we found that the PER for COVID-19-related mortality in SCT recipients was 21.08% (95% CI, 17.18–25.60%). This aligns with the attributable COVID-19 mortality rate of 25% in SCT recipients reported by Ljungman et al. [61]. Other researchers found that age greater than 70 years, uncontrolled hematological disease, an Eastern Cooperative Oncology Group grade of 3 or 4, a C-reactive protein level greater than 20 mg/dL, and neutropenia are associated with increased mortality risk [37]; use of azithromycin or low-dose corticosteroids was associated with decreased mortality risk; and use of hydroxychloroquine did not significantly improve the mortality rate. We tested the influence on mortality rate of the time to SARS-CoV-2 infection after SCT; presence of GvHD and its type; use of immunosuppressive agents, steroids, hydroxychloroquine, antibiotics, and antivirals; and hospital admission. None of these factors significantly influenced the COVID-19-related mortality rate after SCT, which may be attributed to small sample sizes in the studies we reviewed.
Nevertheless, the mortality rate in allogeneic SCT recipients who had COVID-19 (32%) at 30 days seemed to be relatively high, even when compared to COVID-19 hospitalized patients in other settings [62] and advanced age, advanced disease stage, and the need for mechanical ventilation were associated with an increased mortality rate [63]. Special safety measures must be implemented when dealing with stem cell donors with COVID-19 [64]. Although a case report demonstrated that transplantation from COVID-19 donors is feasible [65], such strict measures are needed to ensure that the donor is healthy and free of any disease, especially COVID-19, at the time of transplantation. This is important to ensure the safety of the medical team, who closely take care of donors during pretransplant assessment and the donation process. Thus, SCT during the COVID-19 era requires careful consideration of the benefits and risks and patients should be closely monitored for COVID-19 symptoms and managed accordingly.
In terms of the management of COVID-19, hydroxychloroquine, an antimalarial drug, has been administered as an off-label drug. However, its efficacy in treating COVID-19 is controversial and several studies have shown conflicting results, which have drawn attention worldwide [66]. In our meta-analysis, 53% of the included patients received hydroxychloroquine during their COVID-19 treatment, which did not significantly impact mortality. This finding aligns with the results of a study of the effect of hydroxychloroquine versus a placebo in patients with COVID-19, which demonstrated no impact of hydroxychloroquine on the patients’ clinical status, including the mortality rate [67]. Also, according to a Cochrane Library review, treatment with hydroxychloroquine does not alter the need for ventilation in COVID-19 patients or affect their risk of death [68]. Moreover, hydroxychloroquine has been associated with several adverse effects, including cardiotoxicity, and its use in COVID-19 patients may exacerbate underlying cardiac conditions. Therefore, the use of hydroxychloroquine in the treatment of COVID-19 is not currently recommended [67,68].
Optimizing hospital admission of SCT recipients who developed COVID-19 is another critical clinical decision and requires weighing the risks and benefits. Hospital admission is necessary for severe cases of COVID-19 requiring oxygen support or mechanical ventilation. In this meta-analysis, 55.2% of the patients underwent hospital admission during management of COVID-19. Also, El Fakih et al. [69] reported that the admission rate for SCT recipients with COVID-19 was 53%. The decision to admit a COVID-19 patient to the hospital should be based on the severity of the symptoms and the risk factors for severe COVID-19, such as advanced age, the presence of comorbidities, and immunocompromised status. Moreover, hospital admission is necessary for close monitoring of COVID-19 patients at increased risk for serious complications, such as thromboembolism and acute respiratory distress syndrome, especially when they are immunocompromised.
After SCT, immunocompromised patients are at greater risk for a prolonged viral phase than immunocompetent patients are. Some SCT recipients shed infectious viral particles for months after exposure to COVID-19 [49]. The pathogenesis of COVID-19 is characterized by an initial viral phase and may be followed by a severe inflammatory phase. This hyperinflammatory state eventually results in an increased mortality rate [70]. Therefore, treatment of COVID-19 is mainly focused on the control of the initial viral phase and/or the hyperinflammatory response. Antiviral drugs have been used in the treatment of COVID-19 to reduce viral replication and improve clinical outcomes. For example, remdesivir (a nucleoside analog) is an antiviral drug approved by the U.S. Food and Drug Administration for the treatment of COVID-19 in hospitalized patients. A randomized controlled trial compared remdesivir with a placebo in hospitalized patients with COVID-19 and found that the median time to recovery was 10 days in the remdesivir arm and 15 days in the placebo arm [71]. This benefit was also observed in immunosuppressed cancer patients (8%) in that trial, in whom treatment with remdesivir accelerated recovery. The benefit of remdesivir is evident in patients who need low-flow oxygen delivery and those having COVID-19 symptoms for fewer than 10 days, which may be explained by the fact that it supports its effect mainly during the viral phase of COVID-19 infection [71]. Considering the potentially enhanced impact of antiviral treatments on the outcomes of immunocompromised patients, particularly those with prolonged viral phases, in addition to an overall good safety profile, SCT recipients may benefit the most from COVID-19 treatment with remdesivir. In this meta-analysis, 71.61% of the patients received antiviral treatment during their COVID-19 infections and remdesivir was the most used antiviral.
Furthermore, our meta-analysis demonstrated that 39.44% of the SCT recipients infected with COVID-19 received immunosuppressive drugs. Hence, most severe COVID-19 cases are consequences of hyperinflammatory status and the use of systemic immunosuppressive agents in such cases has been an area of intense investigation. Treatment with dexamethasone was found to improve the survival of hospitalized patients with moderate to severe COVID-19 requiring supplemental oxygen or mechanical ventilation [72]. In addition to dexamethasone, adjuvant use of tocilizumab has resulted in improved clinical outcomes, including survival, in COVID-19 patients regardless of the respiratory support needed. Treatment with tocilizumab has been demonstrated to additively decrease the need for mechanical ventilation and to decrease the mortality rate in those not needing invasive mechanical ventilation at the baseline [73].
Our meta-analysis had some limitations. First, the available studies were mostly observational, retrospective, and limited in sample size and heterogeneous in their reporting details and quality. Many of the variables we looked for were missing. This may introduce selection bias and limit the generalizability of our findings, for example, as it is very likely that patients hospitalized for COVID-19 are much more likely to be described in publications, as opposed to those diagnosed in the primary care setting. Second, the management of COVID-19 patients varies across institutions and countries, which may impact outcomes. Third, the COVID-19 pandemic is rapidly evolving and new information on the topic is constantly emerging. Third, we need to emphasize that collecting and analyzing the data for a systematic review, especially if it includes a meta-analysis, takes a while. Therefore, between the search strategy being performed and the final paper being published, time passes and new papers are being published. Lastly, one of the biggest fears after SCT is catching a COVID-19 infection immediately post-graft period where neutropenia is intense. Neutropenia has not been included in this analysis and we found only three studies where COVID-19 occurred within 100 days of transplantation. Furthermore, there is no way to know if the patients were still neutropenic. We studied all other available factors that may have contributed to higher mortality but we did not study neutropenia because such information was not available.
In summary, based on the current available data, the SCT recipients are at increased risk for severe COVID-19 and COVID-19-related mortality. The use of hydroxychloroquine in the treatment of COVID-19 is controversial and is not recommended owing to its limited efficacy and potential adverse effects and our study did not find evidence for its benefit. Hospital admission is necessary for severe cases of COVID-19 and the risk factors associated with mortality include advanced age, male sex, and an increased comorbidity burden. Antiviral drugs such as remdesivir have produced promising results in the treatment of COVID-19 in hospitalized patients.
5. Conclusions
The current literature is severely limited and detailed reporting as well as controlled prospective studies are needed to further understand the prognostication and optimal management of COVID-19 patients in the SCT setting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Samaha R. Kattan J. Hematopoietic stem cell transplantation dilemma during the COVID-19 era Future Oncol.2020161569157310.2217/fon-2020-041432458703 PMC 7255427 · doi ↗ · pubmed ↗
- 2Ardura M. Hartley D. Dandoy C. Lehmann L. Jaglowski S. Auletta J.J. Transplant-Associated Learning Network, Addressing the Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on Hematopoietic Cell Transplantation: Learning Networks as a Means for Sharing Best Practices Biol. Blood Marrow Transplant.202026 e 147e 16010.1016/j.bbmt.2020.04.01832339662 PMC 7194714 · doi ↗ · pubmed ↗
- 3Coronavirus Disease 2019 in Children—United States, February 12-April 2, 2020 MMWR Morb. Mortal. Wkly. Rep.20206942242610.15585/mmwr.mm 6914 e 432271728 PMC 7147903 · doi ↗ · pubmed ↗
- 4Balduzzi A. Brivio E. Rovelli A. Rizzari C. Gasperini S. Melzi M.L. Conter V. Biondi A. Lessons after the early management of the COVID-19 outbreak in a pediatric transplant and hemato-oncology center embedded within a COVID-19 dedicated hospital in Lombardia, Italy Estote parati. Bone Marrow Transpl. Transplant.2020551900190510.1038/s 41409-020-0895-4PMC 716753232313181 · doi ↗ · pubmed ↗
- 5Szer J. Weisdorf D. Querol S. Foeken L. Madrigal A. The impact of COVID-19 on the provision of donor hematopoietic stem cell products worldwide: Collateral damage Bone Marrow Transpl. Transplant.2020552043204410.1038/s 41409-020-0873-x PMC 709185032203269 · doi ↗ · pubmed ↗
- 6Gaur A.H. Bundy D.G. Werner E.J. Hord J.D. Miller M.R. Tang L. Lawlor J.P. Billett A.L. A Prospective, Holistic, Multicenter Approach to Tracking and Understanding Bloodstream Infections in Pediatric Hematology-Oncology Patients Infect. Control Hosp. Epidemiol.20173869069610.1017/ice.2017.5728399945 · doi ↗ · pubmed ↗
- 7Ljungman P. Mikulska M. de la Camara R. Basak G.W. Chabannon C. Corbacioglu S. Duarte R. Dolstra H. Lankester A.C. Mohty M. The challenge of COVID-19 and hematopoietic cell transplantation; EBMT recommendations for management of hematopoietic cell transplant recipients, their donors, and patients undergoing CAR T-cell therapy Bone Marrow Transpl. Transplant.2020552071207610.1038/s 41409-020-0919-032404975 PMC 7220575 · doi ↗ · pubmed ↗
- 8Wu C. Chen X. Cai Y. Xia J. Zhou X. Xu S. Huang H. Zhang L. Zhou X. Du C. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China JAMA Intern. Med.202018093494310.1001/jamainternmed.2020.099432167524 PMC 7070509 · doi ↗ · pubmed ↗