Giant Lipoma of the Bauhin’s Valve
Cosmina Fugărețu, Catalin Misarca

TL;DR
A 46-year-old patient had a large benign lipoma at the ileocecal valve, which was successfully treated with surgery after being initially suspected as a malignant tumor.
Contribution
This case highlights the importance of considering large lipomas in the differential diagnosis of gastrointestinal bleeding and intestinal obstruction.
Findings
A 16/11/12 cm lipoma was found at the ileocecal valve after initial suspicion of a malignant tumor.
The patient recovered well after an extended right hemicolectomy.
Large lipomas should be considered in cases of digestive hemorrhage or obstruction.
Abstract
Lipomas are benign tumors that can affect the digestive tract, everywhere from the hypopharynx to the rectum. Lipomas affecting the large intestine are the second most common benign tumor, after colon adenoma. We present the case of a 46-year-old patient who was initially hospitalized in the Gastroenterology Clinic with a diagnosis of gastrointestinal bleeding. The colonoscopy raised the suspicion of a malignant tumor of the transverse colon, but the computed tomography scan showed the existence of a lipoma that measured 16/11/12 cm that occupied the ascending and transverse colon, though the CT examination could not determinate the origin of the lipoma. After restoring the hydro-electrolytic and fluid balance of the patient, surgery was performed and a huge lipoma of the ileocecal valve was discovered. Extended right hemicolectomy was performed, with good subsequent postoperative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
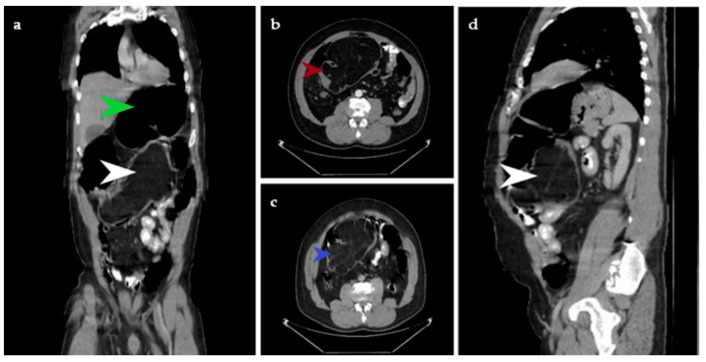 Figure 1
Figure 1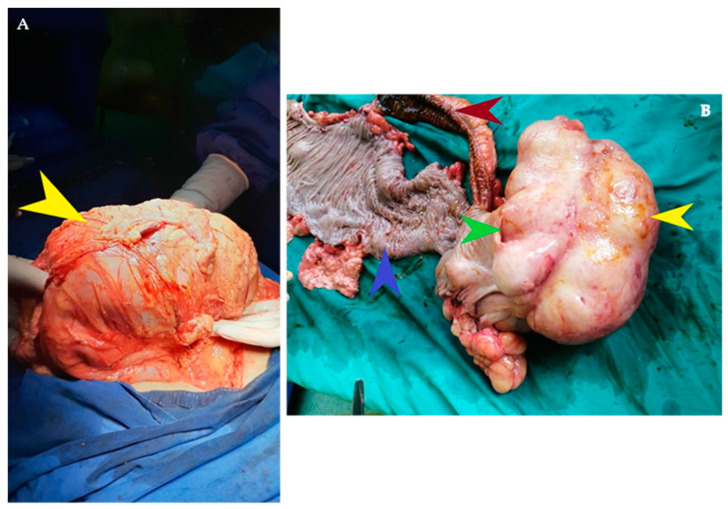 Figure 2
Figure 2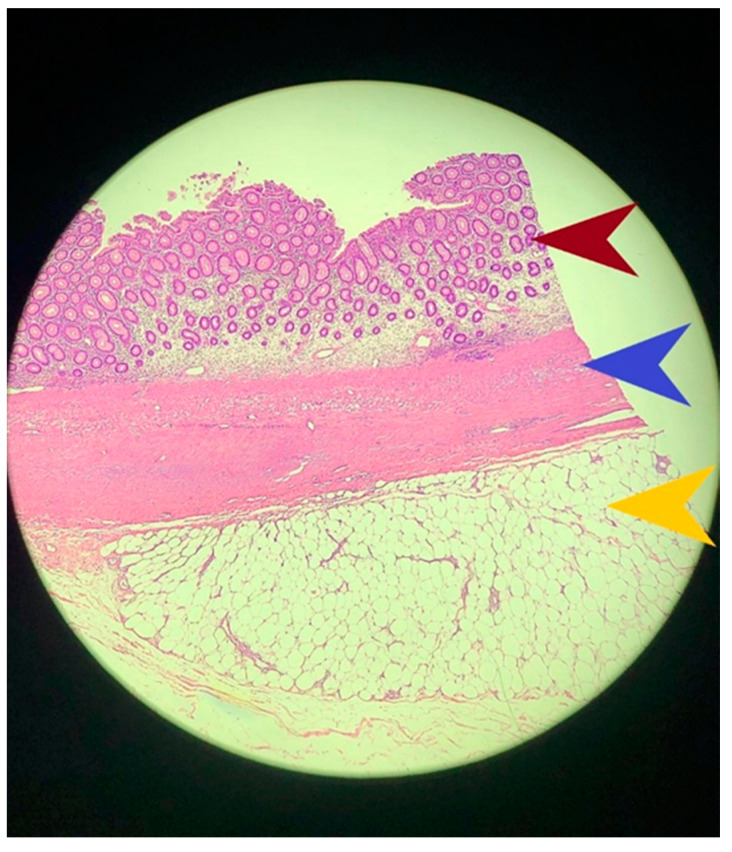 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment · Vascular Malformations and Hemangiomas
Lipomas are benign tumors which develop from adipose tissue. The intestinal localization of lipomas is rare, being found in a percentage of 0.2–4.4% of all digestive tumors [1]. Intestinal lipomas were first described by Baurer in 1757 [2]. In terms of their origin, about 90% come from the submucosa and 10% from the subserosa [3]. Although theoretically they can be found anywhere along the digestive tract, from the hypopharynx to the rectum, these tumors are more frequent in the large intestine, rarer in the small intestine and very rare in the esophagus and stomach. The most common clinical manifestations are intussusception, followed by gastrointestinal bleeding when the lining mucosa is ulcerated and intestinal obstruction in the case of large lipomas [4,5,6]. The symptoms are not specific and often these are not taken into account when a patient arrives in the Emergency Department and when being subsequently diagnosed endoscopically or by medical imaging; they are also discovered during surgery.
The paraclinical diagnosis is most often made by performing a colonoscopy that reveals a pediculated tumor formation due to intestinal peristalsis that causes the extrusion of the lipoma in the digestive tract, but can also be sessile. “Pillow sign” occurs when a surface indentation is observed upon pushing the lipoma with closed biopsy forceps during colonoscopy. “Naked fat sign” is the evacuation of fat at the biopsy site [7]. In this case, the colonoscopy examination suggested an ulcerated transverse colon tumor that cannot be passed with the endoscope and the correct diagnosis was revealed by the abdominal CT examination that detected a well-defined tumor with fatty densities of 40–120 HU and allowed the exact establishment of tumor size. Mention should also be made of ‘The squeeze sign’, which is caused by changes in the shape and size of the tumor as a result of intestinal peristalsis and is evident on contrast enhanced fluoroscopy [8]. This examination was not performed in this case. Also, the MRI examination provides the most information for preoperative assessment of the benign or malignant character of lipomatic tumors. Thus, the authors have succeeded in the correct preoperative classification of lipomatic tumors in more than 70% of cases [9].
Small intestinal lipomas, less than 2 cm in diameter, may benefit from endoscopic submucosal excision; for the other cases, limited or extended colon resection surgery is preferable when a malignant neoplastic pathology cannot be excluded [3].
In this case, surgical treatment was the only therapeutic alternative given the giant size of the lipomatous tumor. The laparoscopic approach, although desirable, was not possible due to the impossibility of manipulating the right colon occupied by the large tumor and because of the colonic hemorrhage and worry about an isolated large bowel obstruction. After mechanical preparation of the colon with Fortrans and the administration of prophylactic antibiotic therapy with generation II cephalosporins and Metronidazole, surgery was performed. Extended right hemicolectomy was performed with the ligation at the origin of the ileocolic vessels, right colic and middle colic artery, and the restoration of intestinal continuity was achieved by a latero-lateral ileocolic anastomosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vecchio R. Ferrara M. Mosca F. Ignoto A. Latteri F. Lipomas of the large bowel Eur. J. Surg. Acta Chir.19961629159198956963 · pubmed ↗
- 2Zhang H. Cong J.C. Chen C.S. Qiao L. Liu E.Q. Submucous colon lipoma: A case report and review of the literature World J. Gastroenterol.2005113167316910.3748/wjg.v 11.i 20.316715918213 PMC 4305863 · doi ↗ · pubmed ↗
- 3Cirino E. CalìV. Basile G. Muscari C. Caragliano P. Petino A. Invaginazione intestinale da lipoma del colon [Intestinal invagination caused by colonic lipoma]Minerva Chir.1996517177239082238 · pubmed ↗
- 4Suleiman J. Suleman M. Mremi A. Sadiq A. Mohamedali A. Machaku D. Lodhia J. Colon Lipoma Causing Colo-Colic Intussusception in an Adult: A Case Report from Tanzania Case Rep. Surg.20242024777725810.1155/2024/777725838223374 PMC 10787654 · doi ↗ · pubmed ↗
- 5Álvarez-Bautista F.E. Moctezuma-Velázquez P. Cisneros-Correa J.C. Aguilar-Frasco J.L. Vélez-Valle A. Vergara-Fernández O. Salgado-Nesme N. Colonic lipomas an uncommon cause of intussusception in adult patients: Report of three cases and literature review. [Lipomas de colon una causa poco común de intususcepción en pacientes adultos: Reporte de tres casos y revisión de la literature]Cir. Cir.2021899123493254010.24875/CIRU.21000047 · doi ↗ · pubmed ↗
- 6Reijnen H.A. Joosten H.J. de Boer H.H. Diagnosis and treatment of adult intussusception Am. J. Surg.1989158252810.1016/0002-9610(89)90309-72662787 · doi ↗ · pubmed ↗
- 7Zimmer V. Naked Fat Sign Is a Characteristic of Colonic Lipoma Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc.201917 A 2910.1016/j.cgh.2018.02.04629510213 · doi ↗ · pubmed ↗
- 8Marra B. Occlusione intestinale da lipoma del colon. A proposito di due casi [Intestinal occlusion due to a colonic lipoma. Apropos 2 cases]Minerva Chir.199348103510398290148 · pubmed ↗