Enterobacterales Biofilm-Specific Genes and Antimicrobial and Anti-Inflammatory Biomarkers in the Blood of Patients with Ischemic Heart Disease
Agne Giedraitiene, Vacis Tatarunas, Kornelija Kaminskaite, Ugne Meskauskaite, Svitlana Boieva, Yu Ajima, Ieva Ciapiene, Audrone Veikutiene, Vaidotas Zvikas, Nora Kupstyte-Kristapone, Valdas Jakstas, Dalia Luksiene, Abdonas Tamosiunas, Vaiva Lesauskaite

TL;DR
This study explores how bacteria like Enterobacterales may contribute to heart disease by analyzing their presence and effects in patients with ischemic heart disease.
Contribution
The study identifies specific bacterial genes and biomarkers linked to ischemic heart disease and atherosclerosis.
Findings
Bacterial 16S rDNA was detected in 31% of patients with ischemic heart disease.
Enterobacterales genes were more common in younger patients and those with type 2 diabetes.
Higher concentrations of LL-37 and 12S-HETE were found in patients with bacterial DNA and biofilm-specific genes.
Abstract
Background: Ischemic heart disease (IHD) is the most prevalent type of cardiovascular disease. The main cause of IHD is atherosclerosis, which is a multifactorial inflammatory disease of blood vessels. Studies show that bacteria might have a significant impact on the pathogenesis of atherosclerosis and plaque rupture. This study aimed to evaluate the complexity of interactions between bacteria and the human body concerning metabolites and bacterial genes in patients with ischemic heart disease. Methods: Bacterial 16S rDNA and wcaF, papC, and sdhC genes were detected in whole blood using a real-time PCR methodology. An enzyme-linked immunosorbent assay was used to measure the concentration of the LL-37 protein. An analysis of ARA in blood plasma was performed. Results: Bacterial 16S rDNA was detected in 31% of the study patients, and the genes wcaF and sdhC in 20%. Enterobacterales genes…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
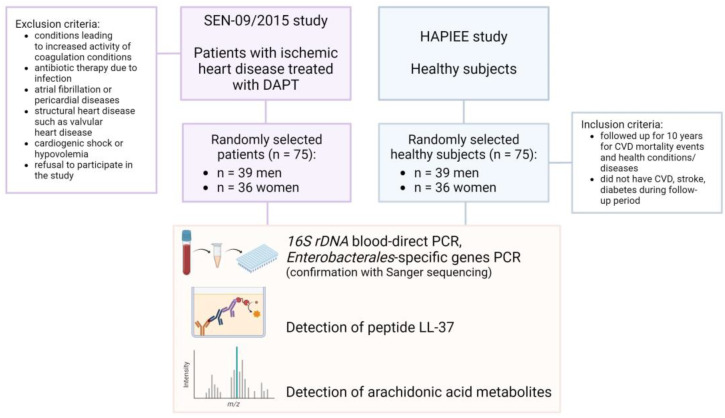 Figure 1
Figure 1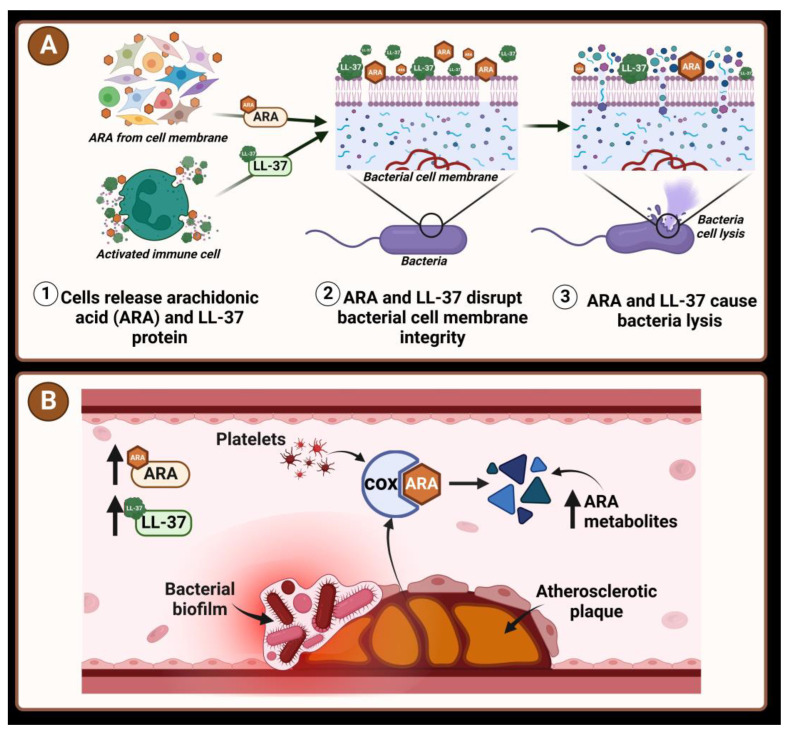 Figure 2
Figure 2- —Medical Academy
- —Lithuanian University of Health Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCultural and Social Studies in Latin America · Philosophical and Cultural Analysis · Cultural and Mythological Studies
1. Introduction
Cardiovascular diseases (CVD) remain the main cause of death in Western countries, and ischemic heart disease (IHD) is the most prevalent among CVD. It was estimated that around 126 million people, who make up approximately 1.7% of the world’s population, have IHD [1]. In Central and Eastern European countries, an increase in IHD morbidity, compared to Northern, Southern, and Western Europe, is observed [2]. The standardized rate of deaths from IHD of 5362 deaths per million inhabitants made Lithuania a leader with the highest mortality rate among the European Union (EU) Member States in 2017 [3].
The main cause of IHD is atherosclerosis. Atherosclerosis is an inflammatory lipoprotein-driven multifactorial disease causing atherosclerotic plaque development and coronary blood flow reduction. If a rupture or erosion of a plaque’s fibrous cap occurs in coronary arteries, it might result in unstable angina or myocardial infarction. The complexity of this condition has led to great concern in finding novel tools for the early diagnosis or prognosis of atherosclerosis and IHD [4,5,6,7].
One of the possible factors for an early diagnosis of IHD could be a biomarker of atherosclerosis progression, the genetic material of certain species of bacteria [8]. Numerous studies have shown that various bacteria and viruses have a direct impact on the vascular endothelium [9,10]. Pathogens are found in the atherosclerotic plaque, and they are harbored in the latent state [11]. A lipopolysaccharide of Escherichia coli (E. coli) was detected in atherosclerotic plaques, and possibly it is related to the damage and rupture of plaques via Toll-Like Receptor 4 (TLR4)-mediated oxidative stress [12]. Zdimal and Davies, 2022, demonstrated that if a biofilm is exposed to an elevated concentration of free iron, it may undergo dispersion contributing to the weakening of arterial tissues and destabilization of the atherosclerotic plaque [13].
The study demonstrated that bacteria might form a biofilm within human carotid arterial plaques [14]. Microbial cells within biofilms tolerate up to 100–1000 times higher concentrations of antibiotics and enhance bacterial survival in the human body, including the bloodstream [15,16]. More than 100 genes have been encountered encoding biofilm in E. coli [17,18]. The wcaF gene encodes an acetyltransferase associated with the polysaccharide colanic acid’s synthesis. Colanic acid is an extracellular polysaccharide needed for the formation of the complex three-dimensional structure of E. coli biofilms [19]. The P-fimbriae, encoded by the pap operon, is responsible for adhesion and is found in many UTI E. coli strains. The papC-encoded protein forms pores in the outer membrane of E. coli and is responsible for the transportation of protein pilin subunits [20]. The sdhC gene encodes one of the four subunits of the inner membrane protein succinate dehydrogenase, which is involved in the Krebs cycle [21]. All three genes wcaF, papC, and sdhC are located on the E. coli chromosome and encode proteins directly involved in biofilm formation.
The 16S rRNA gene is a part of the prokaryotic ribosome 30S subunit and it is coded in the genomes of all bacteria. The 16S rRNA gene sequencing has been used for the identification, classification, and quantitation of microbes for decades [22]. It may also allow the identification of new and non-cultured bacteria [23], as 16S rRNA is highly conserved and specific. It plays a central role in phylogenetic research, as it is sustained between different species of bacteria and archaea [24].
The detection of bacteria in the blood flow is usually associated with a low sensitivity in the presence of extremely low concentrations and time-consuming methodology [25]. The inhibition of PCR amplification and interference with the detection of fluorescence slow down bacterial detection and identification [26]. New enzymes used in the polymerase chain reaction, which have been developed during recent years, allow researchers to overcome these weak points of research and ensure the successful performance of the bacterial gene amplification directly from patient blood (without the extraction of DNA before amplification in classic PCR).
LL-37 is a cathelicidin-related antimicrobial peptide (CRAMP). It plays a crucial role in the immune response to bacterial infections and is actively involved in regulating inflammatory processes. CRAMP enhances the chemotactic responsiveness of bone marrow and progenitor cells [27]. A study shows that decreased LL-37 might be associated with myocardial infarction [28,29], while a high LL-37 level predicts lower major adverse cardiovascular events after ST-segment elevation myocardial infarction [30,31].
Stimulated immune cells may produce significant amounts of arachidonic acid metabolites such as 12-HETE, 15-HETE, PGE_2_, and LTB4. These compounds could be an early inflammatory signal for the initiation of the immune system [32].
Thus, this study aimed to assess the complexity of interactions between bacteria and the human body concerning metabolites and bacterial genes in patients with ischemic heart disease. Moreover, concentrations of the protein LL-37 and arachidonic acid (ARA) metabolites produced by a host in the immune response to ischemic heart disease were measured, and associations between all parameters were determined.
2. Materials and Methods
2.1. Study Population and Inclusion Criteria
The study included 75 randomly selected patients with ischemic heart disease (39 men and 36 women), and 75 healthy persons (39 men and 36 women) as a control group. All patients were hospitalized due to ischemic heart disease at the Department of Cardiology at the Hospital of Lithuanian University of Health Sciences Kaunas Clinics in Kaunas, Lithuania, from 2013 to 2017, and were treated with dual antiplatelet therapy (DAPT) of clopidogrel, or ticagrelor and aspirin. Hormone anti-inflammatory medications were not prescribed to the patients.
The exclusion criteria of patients were conditions leading to an increased activity of coagulation (malignant neoplasia and severe inflammation [C-reactive protein level > 100 mg/L] or patients who had undergone antibiotic therapy due to infection, patients diagnosed with atrial fibrillation or pericardial diseases, significant structural heart disease such as valvular heart disease), cardiogenic shock or hypovolemia, and the refusal of a patient to take part in this study.
The patient population’s clinical data and blood samples were collected during the SEN-09/2015 study [33,34].
The inclusion criteria for the control group: (1) Control subjects were followed up for 10 years for CVD mortality events and health conditions/diseases after inclusion in the international study Health, Alcohol and Psychosocial Factors in Eastern Europe (HAPIEE), conducted in Kaunas (Lithuania) [35]; (2) None of the participants had a cardiovascular disease, stroke, or diabetes during the follow-up period. The mean age of healthy subjects was 67.7 years (minimum age—45, maximum age—72).
The study design is presented in Figure 1.
2.2. Preparation of Blood Samples
Venous blood sampling of patients was carried out by a routine venipuncture procedure using plastic tubes containing 3.2% sodium citrate anticoagulant (BD Vacutainer, Franklin Lakes, NJ, USA). All blood samples were stored at −20 °C. It is known that PCR-inhibitory compounds in human blood can considerably reduce the sensitivity of the PCR assay [36]. The blood protein hemoglobin adversely affects DNA polymerase activity and inhibits amplification and fluorescence signaling; immunoglobulin G disrupts amplification of the first PCR cycles by binding to single-stranded DNA [37]. Red blood cells naturally fluoresce across multiple wavelengths, which span the emission and excitation spectra of many commonly used fluorescent reporters and dyes such as SYBR Green I, and Midori Green, making the endogenous fluorescence difficult to distinguish [38]. One microliter of whole blood was taken for the assay. The mixture of blood and a buffer, the composition of which was developed in our laboratory, were gently mixed and heated for 5 min at 98 °C, then centrifuged for 2 to 4 s (2700 rpm). The amplification and detection of bacterial genes were performed using a QuantStudio 3 Real-Time System instrument (Thermo Fisher Scientific, Waltham, MA, USA). A blood direct PCR (BD-PCR) using genomic DNA without its extraction was performed directly from 1 µL of treated whole blood using specific primers. A mix of primers was prepared to amplify bacterial 16S rDNA. Primer sequences (Table 1), the primer mixture (Table 2), and reaction parameters (Table 3) were adopted from Barghouthi S. A. et al., 2011 [39], And oligonucleotide primers used for the amplification of wcaF, papC, and sdhC were adopted from the following references [31,32,40] (Table 4). The reaction was performed in standard 96-well real-time PCR plates. Thermal cycling program parameters used in blood direct PCR are shown in Table 3 and Table 5. Amplicon size was verified in 2% agarose gel. Bacterial DNA from selected strains was used as a positive control.
2.3. Extraction of Bacterial DNA
A reference E. coli ATCC 25922 strain was used to prepare a bacterial suspension. A few colonies of one-day E. coli bacteria were mixed with 700 µL nuclease-free water, then the suspension was vortexed and centrifuged for 2–4 s (2700 rpm). Bacterial cell wall structures were disrupted mechanically, and high-fidelity DNA polymerase (Thermo Fisher Scientific, Vilnius, Lithuania) was used for the gene amplification; no further DNA purification was required.
2.4. Confirmation of Bacterial DNA with Sanger Sequencing
The purification of randomly selected PCR products for bacterial DNA sequencing from TBE-buffered agarose gel was performed using the Zymoclean™ Gel DNA Recovery Kit (Zymo Research, Irvin, CA, USA). DNA sequencing was conducted by using the Sanger sequencing method. The interpretation of sequencing chromatograms was carried out with Chromas (Technelysium, Brisbane, Queensland, Australia).
2.5. Detection of LL-37
The sandwich enzyme immunoassay (Enzyme-linked Immunosorbent Assay Kit “Human Antibacterial Peptide LL-37 ELISA Kit” (Cusabio Technology LLC, Houston, TX, USA) was used to measure LL-37 in human plasma. All reactions were performed following the manufacturer’s instructions. LL-37 was detected by measuring optical density at 450 nm using a microplate reader Stat Fax 4200 (Awareness Technologies, Palm City, FL, USA). The concentration of the LL-37 peptide was calculated using a standard calibration curve. The calibration curve was performed using Curve Expert 1.4 (Hyams Development, Huntsville, AL, USA).
2.6. Detection of ARA Metabolites in Blood Plasma
The concentrations of ARA metabolites in blood plasma were measured as described above [41]. The extraction and preparation of the samples for analysis were conducted at the Laboratory of Molecular Cardiology. The analysis of ARA metabolites in blood plasma was performed at the Institute of Pharmaceutical Technologies of the Lithuanian University of Health Sciences.
2.7. Statistical Analysis
Statistical analysis was performed with IBM SPSS Statistics V27 software (IBM Corp., Foster City, CA, USA). The Shapiro–Wilk test was used to check the normality of the variable’s distribution. Pearson’s χ^2^ or Fisher′s exact test was used for categorical variables. The results were considered statistically significant when p < 0.05.
3. Results
Bacterial 16S rDNA was detected in 31% (n = 23/75) and genes specific for Enterobacterales wcaF and sdhC but not the papC were detected in 20% (n = 15/75) of the whole-blood samples of the study patients. The highest percentage of Enterobacterales-specific genes detected in the analyzed samples was 13.3% of the gene wcaF (n = 10/75), followed by 8% of the gene sdhC (n = 6/75). One of the patients had both the wcaF and sdhC genes. The differences in gene prevalence by sex were not significant due to the small sample size (Table 6). The 16S rRNA gene, a molecular marker for the identification of bacterial species, was not detected in any of the control subjects. Further analysis of the healthy group was not performed.
3.1. Bacterial DNA Sequencing Results
Sanger sequencing was performed for the PCR product of a blood sample with the wcaF gene positive. Analysis of the resulting sequence in the BLAST program corresponded to Escherichia spp. bacterium by 93.8%. Sequencing of the PCR product of a blood sample with the sdhC gene detected by RT-PCR showed the sdhC gene encoded by bacteria of the genus Serratia or Escherichia (90.5% and 88.6%, respectively).
3.2. Enterobacterales Genes in Patient Blood
The distribution of Enterobacterales genes may vary according to the patient’s gender and age. Bacterial genes tended to be detected more frequently in the blood of men than women (p = 0.086) (Appendix A). Patients younger than 65 years old more frequently had bacterial genes detected in their blood than patients aged 65 years and older (p = 0.018). Additionally, bacterial genes were more frequently detected in patients with type 2 diabetes (p = 0.048) (Appendix A). The results with 16S rDNA were not significant.
3.3. Protein LL-37 Concentration and Bacterial Genes
The concentrations of LL-37 were higher in patient blood with 16S rDNA and biofilm-specific genes (Table 7).
3.4. Concentration of Arachidonic Acid Metabolites and Presence of Enterobacterales Genes in Blood Samples
Patients with Enterobacterales genes in their blood had a higher concentration of 12S-HETE and 5S-HETE than patients without bacterial genes (respectively, p = 0.046 and p = 0.077) (Table 8). The results with 16S rDNA were not significant.
3.5. LL-37 and Arachidonic acid Metabolites
A positive correlation of LL-37 was observed with 5S-HETE (r = 0.367, p = 0.015) when a trend was determined between LL-37 and 12S-HETE (r = 0.307, p = 0.048) in blood plasma.
4. Discussion
This study reports that bacterial 16S rDNA was detected in one-third of the venous blood samples of patients with IHD (30.5%). The presence of 16S rDNA was not significantly associated with IHD, diabetes, or the other factors or conditions analyzed in our study. The healthy population sample tested negative for bacterial 16S rDNA and biofilm-encoding genes. The presence of DNA, a marker of bacterial translocation and a potential biomarker, was reported by other studies in patients with cirrhosis [42], cardiovascular disease [43], type 2 diabetes [44], psoriatic arthritis [45], and atherosclerosis [46]. Bacteria might play a role in the development and progression of atherosclerosis by the formation of biofilms within arterial plaques and the rupture of unstable plaques [14,47]. A plaque’s rupture leads to a life-threatening atherothrombotic lesion, occlusion of the coronary artery, and myocardial ischemia. However, the mechanism of IHD pathogenesis which involves the formation of bacterial biofilms is still not fully understood. There is a big shortage of knowledge on how bacterial fragments accumulate in different parts of the host’s body. One of the possible ways is bacterial biofilm formation [48]. We determined that biofilm-specific genes were more prevalent among patients younger than 65 years old and patients with diabetes. Anhe et al., 2020, determined that plasma samples of individuals with diabetes were enriched with Enterobacterales [49]. Possibly, the increase in the bacterial count of some specific genera might be related to the use of antidiabetic drugs, as E. coli proliferation is increased due to insulin administration under in vitro conditions. Insulin may serve as a signal molecule for the formation of bacterial biofilms [50,51]. About 17% of the study patients had Enterobacterales genes in their blood: 13.3% had the gene wcaF, followed by 8% with the gene sdhC. One of the patients had both the wcaF and sdhC genes. The gene wcaF encodes an acetyltransferase associated with the polysaccharide colanic acid’s synthesis [19]. Prospective studies have shown that exopolysaccharides’ (alginate and colanic acid) synthesis is induced upon attachment of bacteria to the surface [52], but at the same time, the biofilm formation-associated gene wcaF might be regulated by the quorum sensing E. coli regulators B and C [40]. Thus, by regulating exopolysaccharides, the gene wcaF allows control of the E. coli biofilm formation [53]. Importantly, the P-fimbriae, encoded by the pap operon, is responsible for adhesion and is found in many UTI E. coli strains [20,54]. It is worth noting that the papC gene might be associated with amoxicillin resistance [20]. Moreover, the sdhC gene encodes one of the four inner membrane protein subunits of succinate dehydrogenase, which is involved in the Krebs cycle [21]. A lower prevalence of the papC gene was determined in ciprofloxacin-resistant uropathogenic E. coli than in their susceptible counterparts [55].
It is known that the bacterial cell wall components peptidoglycan and lipopolysaccharides (LPS) alter immune and glucose homeostasis in the host, and bacterial translocation possibly influences the host’s metabolism [56]. Also, the production of immune response signals (such as the synthesis of CRAMP peptides or arachidonic acid derivatives) takes place during the invasion of the host organism [32,57]. This research showed that patients with bacterial genes in blood plasma tend to have higher 12S-HETE and LL-37 concentrations than patients with no Enterobacterales genes detected. Certain host-derived metabolites of lipids could have antimicrobial activity via membrane interactions. It was determined that arachidonic acid (ARA) might reduce the virulence of certain strains of E. coli [58], be toxic to certain bacteria, and be able to kill Staphylococcus aureus [59]. The inhibition of the production of cyclooxygenase-derived compounds of ARA induces the accumulation of precursors, especially ARA [56]. The results of our study showed that the concentration of 12S-HETE, a derivative of ARA, was higher in patients with detected biofilm-forming genes than in patients with no bacterial genes. The bio-active molecular 12S-HETE participates in the host metabolism of glucose [60] and inflammation [61]. In addition, our results showed that the cathelicidin LL-37 concentration was higher in patients with 16S rDNA and biofilm-specific genes in their blood than in patients without these bacterial genes. The antimicrobial host defense peptide cathelicidin LL-37 is a part of the innate immune response in humans. It is expressed during infection and kills bacteria via membrane interactions [62]. Studies have shown that expression of LL-37 is increased up to six-fold in atherosclerotic lesions [63]. The peptide LL-37 is produced by cells of the immune system: neutrophils, monocytes, macrophages, and epithelial cells [64]. Hypothetical mechanisms of action of bacteria and the host metabolites in the pathogenesis of IHD are shown in Figure 2.
Assessing bacterial genes such as biofilm-encoding genes or 16S ribosomal-ribonucleic acid might be useful in diagnostics or the prediction of non-infectious diseases such as cardiovascular diseases. Rigorous referral pathways to perform molecular tests may result in significant savings [65]. Genetic screening for some specific genes and testing individuals in advance even if they are asymptomatic, but have a family history of cardiovascular diseases, might help to reduce healthcare costs, personalize treatment, and reduce the number of interventions. Overall, it might improve the patient’s quality of life and survivability [66]. To sum up, it is essential to consider introducing molecular methods for bacterial gene detection/determination in clinical practice that would allow clinicians to obtain more detailed information about the disease and more accurately diagnose it.
5. Conclusions
Bacterial biofilm-specific DNA was more prevalent in IHD patients younger than 65 years of age and in patients with diabetes. Concentrations of the human antimicrobial peptide LL-37 in blood were determined to be higher if patients had 16S rDNA and biofilm-specific genes. Additionally, the concentration of the ARA metabolite 5S-HETE correlated with the LL-37 protein concentration. Thus, the results of this study enhance our understanding that Enterobacterales bacteria may participate in the pathogenesis of atherosclerosis and IHD. The described biomarkers might be useful for the identification of patients who might be at risk of atherosclerotic plaque rupture and IHD. Nevertheless, further studies are needed to elucidate the specific role of the host and microorganism metabolites in the progression and development of atherosclerosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khan M.A. Hashim M.J. Mustafa H. Baniyas M.Y. Al Suwaidi S.K.B.M. Al Katheeri R. Alblooshi F.M.K. Almatrooshi M.E.A.H. Alzaabi M.E.H. Al Darmaki R.S. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study Cureus 202012 e 934910.7759/cureus.934932742886 PMC 7384703 · doi ↗ · pubmed ↗
- 2European Cardiovascular Disease Statistics 2017 Available online: https://ehnheart.org/cvd-statistics/cvd-statistics-2017.html(accessed on 15 March 2022)
- 3An Official Website of the European Union Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20200928-1(accessed on 23 April 2022)
- 4Ou J.S. Li H.M. Shi M.M. Ou Z.J. Ischemic Heart Disease Encyclopedia of Gerontology and Population Aging Gu D. Dupre M. Springer Cham, Switzerland 2020
- 5Pahwa R. Jialal I. Atherosclerosis. [Updated 8 August 2022]Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA January 2022 Available online: https://www.ncbi.nlm.nih.gov/books/NBK 507799/(accessed on 1 March 2022)
- 6Severino P. D’Amato A. Pucci M. Infusino F. Adamo F. Birtolo L.I. Netti L. Montefusco G. Chimenti C. Lavalle C. Ischemic Heart Disease Pathophysiology Paradigms Overview: From Plaque Activation to Microvascular Dysfunction Int. J. Mol. Sci.202021811810.3390/ijms 2121811833143256 PMC 7663258 · doi ↗ · pubmed ↗
- 7Buja L.M. Vander Heide R.S. Pathobiology of Ischemic Heart Disease: Past, Present and Future Cardiovasc. Pathol.20162521422010.1016/j.carpath.2016.01.00726897485 · doi ↗ · pubmed ↗
- 8Jonsson A. Bäckhed F. Role of gut microbiota in atherosclerosis Nat. Rev. Cardiol.201714798710.1038/nrcardio.2016.18327905479 · doi ↗ · pubmed ↗