Myocardial infarction due to coronary embolism after mechanical aortic valve replacement: a case report
Mukan Kagan Kus, Anil Karaagac, Burak Bozkurt, Ufuk Sadik Ceylan, Mehmet Kaplan

TL;DR
A young patient experienced a heart attack due to a blood clot from a mechanical aortic valve, which was successfully treated with intervention and medication.
Contribution
This case report highlights a rare complication of mechanical aortic valve replacement and its successful management.
Findings
The patient had acute myocardial infarction due to coronary embolism from a thrombus on the mechanical aortic valve.
Percutaneous coronary intervention and thrombolytic therapy successfully resolved the issue.
The patient recovered and was discharged with anticoagulant and antiaggregant therapy.
Abstract
Prosthetic valve thrombosis (PVT) in aortic valve and its complication coronary embolism is a very rare condition. Diagnosis and treatment process is challenging. We present a young patient with acute myocardial infarction who underwent mechanical aortic valve replacement (AVR) operation one month earlier. Percutaneous coronary intervention was performed and it was succesful. Transeasophageal ecocardiography (TEE) was performed. Thrombus was seen on the mechanical aortic valve and thrombolytic therapy was initiated. Control TEE was performed and there was no signs of thrombi. The patient was discharged healthfully with anticoagulant and antiaggregan.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
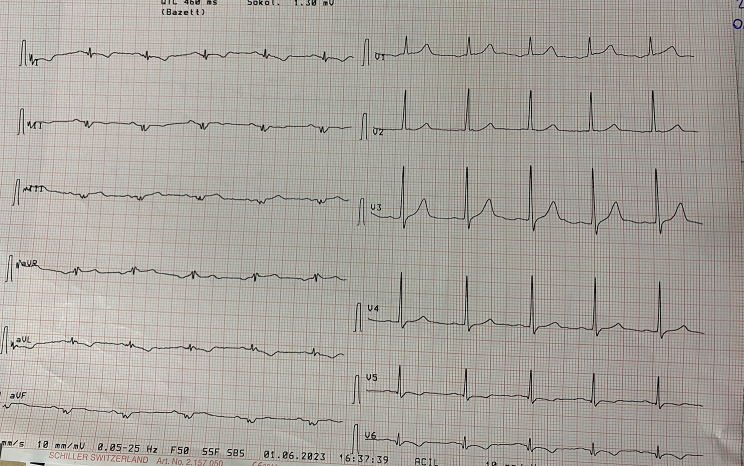 Figure 1
Figure 1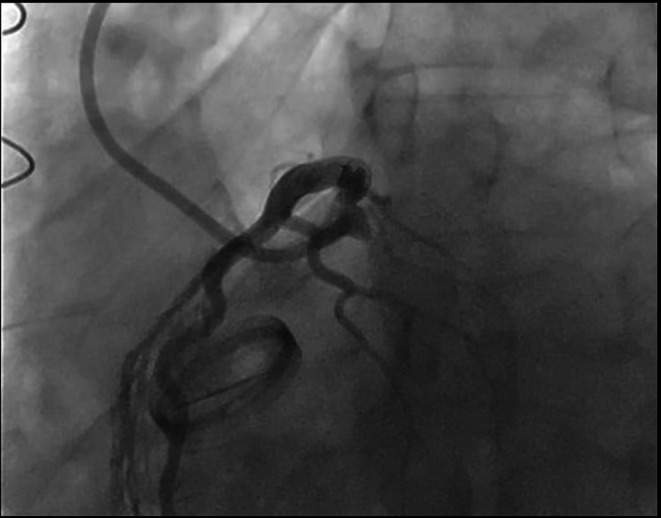 Figure 2
Figure 2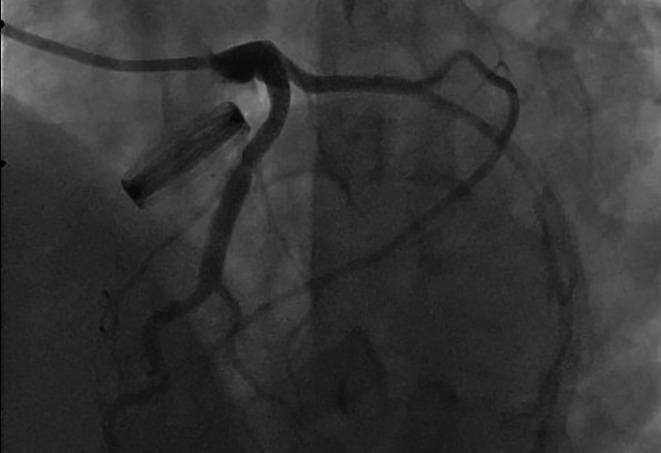 Figure 3
Figure 3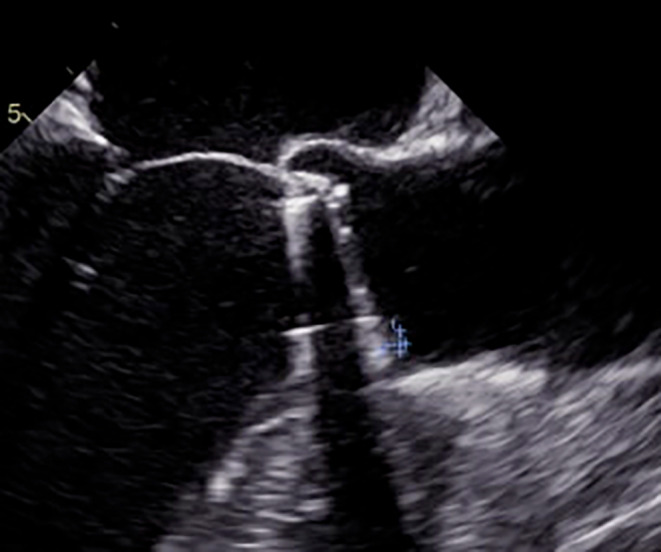 Figure 4
Figure 4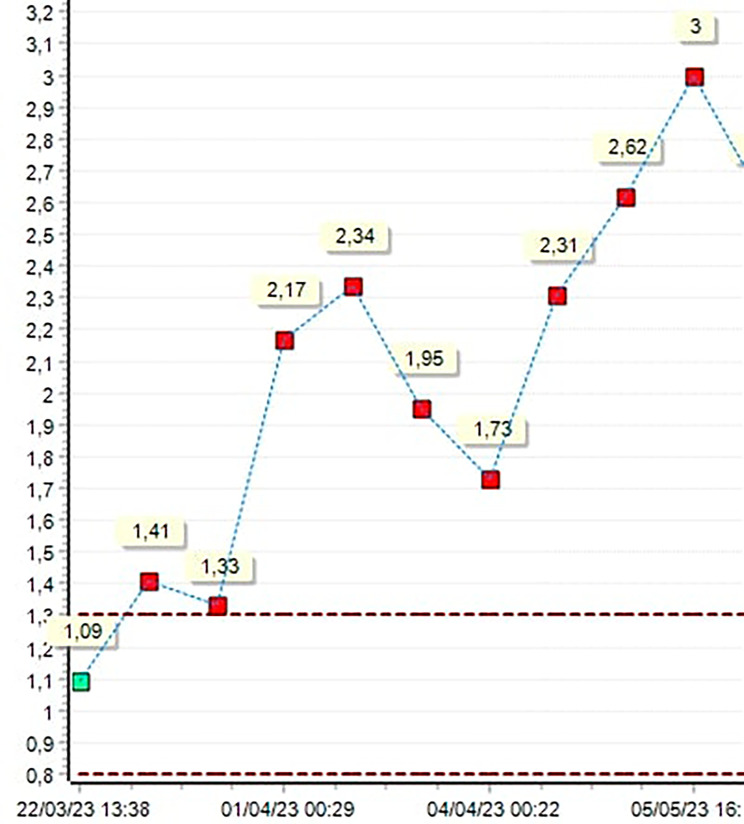 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Atrial Fibrillation Management and Outcomes
Introduction
Prosthetic valve thrombosis is rare but life-threatening complication and seen mostly in mitral valve (75%) [1]. Clinical presantations may vary depending on where the embolism occurs. It may be stroke, retinal emboli, mesenteric ischemia, leg ischemia, myocardial enfarctus(MI) and etc. Coronary embolism is a rare complication after aortic valve replacement. There are many causes of this phenomenon. Coronary embolism may result from calcific aortic root plaque embolism, prosthetic valve thrombosis, infective endocarditis, atrial fibrillation(AF) with ineffective international normalization ratio (INR) in valvular-AF patients, AF with inadequate use of anticoagulants in non-valvular AF patients, dilated cardiomyopathy and mural thrombi [2]. There are reported cases in literature that non-atherosclerotic coronary occlusion along with prosthetic valve thrombosis due to subtherapeutic warfarin therapy. We report a 39 years old male patient who underwent a prosthetic AVR one month earlier presented to acute myocardial infarction and was succesfully treated. He has effective INR value (3.0) in admission.
Case
A 39 years old male patient was complaining about dyspnea and palpitation with effort. Transthoracic ecocardiography showed severe aortic insufficiency with rheumatic trileaflet aortic valve. We perform an AVR operation (23 no Carbomedics) through median sternotomy, ascendan aorta, right atrium cannulation and aortic cross clamp. Aortic valve was trileaflet and elongated cusps with no calcification was seen in peroperative assesment. His angiogram was normal before cardiac operation. He was admitted to our emergency room with sudden onset chest pain one month after the procedure. Vital signs demonstrated body temperature 36.5 °C, heart rate 72/min, blood pressure 110/70 mmHg and respirations 20/min. ECG was normal sinus rhtym and has no remarkable ischemic evidence (Fig. 1). Echocardiography was performed, aortic valve was functional, ejection fraction was normal and there was no sign of aortic dissection. We perform a thoracal CT-scan, we suspect aortic dissection because of characteristic and severity of pain and it was normal. High sensitive troponin I level was significantly elevated so the patient was diagnosed with non-ST elevation myocardial infarction (NSTEMI). Coronary angiography was performed and it showed us total circumflex coronary artery (Cx) occlusion (Fig. 2).
Fig. 1ECG of first admission
Fig. 2. Total occlusion of Circumflex coronary artery (white arrow)
Coronary balloon angioplasty and stent implantation was performed (Fig. 3). After coronary intervention, the patient was transferred to intensive care unit and his hemodynamics were stable. TEE was planned for detecting thrombi, vegetation or pannus formation on the mechanical aortic valve. TEE demonstrated normal functional bileaflet mechanical aortic valve but there was a 3 × 3 mm hypoecogenic, mobile mass that look alike thrombi formation (Fig. 4). Intravenous thrombolytic therapy (alteplase infusion) was administered in intensive care unit. Control TEE performed 3 days after and it showed there was no thrombus formation like before.
Fig. 3. Stent implantation and succesful revascularization of Circumflex coronary artery
Fig. 4TEE image 3x3 mm thrombus on aortic valve (white arrow)
When we investigate the statistical datas of patient’s INR values along postoperative 1 month, there was two suptherapeutic values of INR (1.95 and 1.73 respectively) consecutive just for 2 days, on postoperative third and fourth days. The patient was receiving warfarin combined with low molecular weight heparin (LMWH) (therapeutic dose) on these days. INR was 2.31 on the fifth postoperative day and LMWH was stopped on that day (Fig. 5). The patient was discharged healthfully with dual antiaggregan (asetilsalisilic asid and clopidogrel) added to warfarin therapy.
Fig. 5INR values in one month after operation
Discussion
Mechanical heart valves are thrombogenic and their use requires that the patient receive anticoagulants [3, 4]. Prosthetic valve thrombosis (PVT) is defined as existence of any thrombus material, in the absence of infection, adhesive or near to the mechanical valve leaflets [1]. Clinical presentation varies from insidious dyspnea to cardiac arrest. It can make a way for catasthropic consequences via occluding blood flow through the left ventricular outflow for aortic valve, diastolic disfunction for mitral valve or embolism to any part of body. Coronary embolism should always be considered in the time of examinating patients with sudden onset chest pain who underwent mechanical valve replacement, especially AVR. It is an uncommon cause of acute myocardial infarction. Coronary embolism is a challenging condition to treat and there is no consensus on management so require individualized therapeutic approach [5]. Embolic material also has tendency of going into left coronary system, because of the preferential flow dynamics due to morphology of sinus valsalva [6].
Dürrleman et al. investigate 5430 patients undergone valve operations in their clinic for 20 years and 39 patients presented with PVT [1]. Previous reports shows that coronary embolism from mechanical aortic valve mostly related to subtherapeutic warfarin therapy [7]. There are reported cases related to patients who abruptly discontinued warfarin therapy, concomitant risk factors like oral contraceptive using or smoking. In our case there was none of these risk factors. Unusual and challenging point about our case is patient has effective INR value in admission.
PVT can be treated with anticoagulants, thrombolytics or surgery. Current guidelines suggest that small (< 10 mm) thrombus on prosthetic valves do not require surgical intervention. We saw that our thrombolytic treatment for 3 mm thrombus is enough. Antiagregant treatment added to warfarin therapy in discharge [8].
In this report we aimed contribution to literature about coronary embolism after mechanical valve replacement, share our first time experience and raise awareness that it can occur in safe therapeutic doses of anticoagulants.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dürrleman N Prosthetic valve thrombosis: twenty-year experience at the Montreal Heart Institute J Thorac Cardiovasc Surg 200412713889210.1016/j.jtcvs.2003.12.01315115997 · doi ↗ · pubmed ↗
- 2Kiernan TJ, Ann Marie O, Flynn, Kearney P. Coronary embolism causing myocardial infarction in a patient with mechanical aortic valve prosthesis. Int J Cardiol 112.2 2006;E 14–6.10.1016/j.ijcard.2006.01.03816814882 · doi ↗ · pubmed ↗
- 3Hammermeister KEA comparison of outcomes in men 11 years after heart-valve replacement with a mechanical valve or bioprosthesis N Engl J Med 199332812899610.1056/NEJM 1993050632818018469251 · doi ↗ · pubmed ↗
- 4Cannegieter SC Rosendaal FR Briet E Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses Circulation 1994896354110.1161/01.CIR.89.2.6358313552 · doi ↗ · pubmed ↗
- 5Shibata T et al. Prevalence, clinical features, and prognosis of acute myocardial infarction attributable to coronary artery embolism. Circulation 132.4 2015;241–250.10.1161/CIRCULATIONAHA.114.01513426216084 · doi ↗ · pubmed ↗
- 6PRIZELKATEROTHKOHUTCHINSGROVERMBULKLEYBERNADINEH Coronary artery embolism and myocardial infarction: a clinicopathologic study of 55 patients Ann Intern Med 19788821556110.7326/0003-4819-88-2-155626443 · doi ↗ · pubmed ↗
- 7Ananda RA Zhang Z Coronary embolism due to probable clinical bioprosthetic aortic valve thrombosis: a case report BMC Cardiovasc Disord 20232311810.1186/s 12872-023-03359-937365533 PMC 10294337 · doi ↗ · pubmed ↗
- 8Mahindru S Mechanical prosthetic valve thrombosis in current era: 5-year follow-up Indian J Thorac Cardiovasc Surg 202137140610.1007/s 12055-020-01041-933642711 PMC 7876196 · doi ↗ · pubmed ↗