Why did the UK public not adequately understand the symptoms of COVID-19? An analysis of UK Government statements from 3rd March 2020 to 21st February 2022
Erin Riley, Louise E Smith, G James Rubin, Lisa Woodland

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
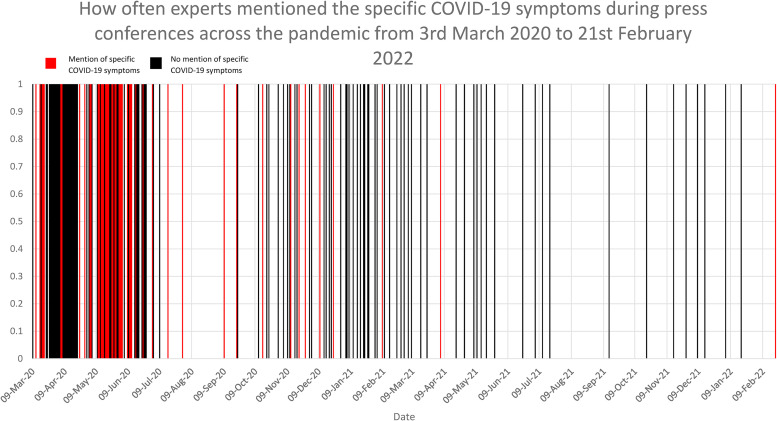 Figure 1
Figure 1- —National Institute for Health and Care Research Health Protection Research Unit (NIHR HPRU) in Emergency Preparedness and Response
- —Economic and Social Research Councilhttps://doi.org/10.13039/501100000269
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMisinformation and Its Impacts · COVID-19 epidemiological studies · COVID-19 Pandemic Impacts
Objectives
During the COVID-19 pandemic, people in the UK with a new continuous cough, high temperature or loss of smell/taste were urged to take steps including testing and self-isolating to prevent the spread of disease.^ 1 ^ The proportion of symptomatic people who engaged in these behaviours was low (42.5%).^ 2 ^ In part, this was driven by low recognition of symptoms that required testing or isolation (51.5%)^ 2 ^ and by perceptions that single or mild symptoms were unlikely to signify COVID-19.^3,4^ Low levels of knowledge may indicate that insufficient attention was paid to communicating these essential facts.
In this study, we assessed whether official spokespeople made speeches to the public about COVID-19 in which they reinforced specific symptoms that required public action.
Design
Content analysis of public speeches made by UK Government spokespeople about COVID-19 during all official press conferences (3^rd^ March 2020 to 21^st^ February 2022) was done.
Setting
We searched a public Government website that listed the transcripts and some video recordings of all televised conferences made by UK Government spokespeople about COVID-19,^ 5 ^ as well as YouTube if we knew of a press conference that was not listed. We identified a total of 171 press conferences.
Participants
It was common for between one and three people to speak at each press conference, with a total of 441 speeches. Five speeches were inaudible or unavailable so we could not analyse these. Therefore, we assessed 436 speeches made by 46 people including the UK Prime Minister, 19 ministers, 15 scientific advisors and 11 others. We excluded spokespeople who only spoke during the question-and-answer section of the press conference.
Main outcome measures
We assessed the frequency with which symptoms were mentioned in every press conference. We categorised discussion of symptoms as: specific mentions (e.g. ‘cough’ or ‘high temperature’ or ‘loss of smell or taste’ as opposed to non-specific mentions such as ‘the symptoms’) and mentions relating to the qualitative nature of the symptom (e.g. ‘even mild’ or ‘immediate’). As there were often multiple speakers at each press conference, we also separately assessed frequencies in each speech.
Results
Only 22.8% (n = 39/171) of press conferences mentioned the specific symptoms that required the public to act (Figure 1). Mention of specific symptoms mainly occurred at the beginning of the pandemic and rarely occurred 6 months after the first press conference (Figure 1). When analysing individual speeches, only 8.9% (n = 39/436) mentioned at least one specific symptom. Discussion of the qualitative nature of symptoms occurred in 12.3% (n = 21/171) of press conferences and 4.8% of speeches (n = 21/436).
How often experts mentioned the specific COVID-19 symptoms during press conferences across the pandemic from 3rd March 2020 to 21st February 2022.
Conclusions
Government spokespeople rarely described specific symptoms that the public needed to be aware of to seek a test or isolate when symptomatic. Although evidence suggests that the public used the qualitative nature of their symptoms as a guide to whether to take action, issues such as the severity, number or duration of symptoms that necessitated a test were rarely mentioned. In future outbreaks, every opportunity should be taken to convey these basic facts to the public to enable them to take action when symptomatic.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rubin GJ Smith LE Melendez-Torres G , et al. Improving adherence to ‘test, trace and isolate’. J R Soc Med 2020;113:335–338.32910870 10.1177/0141076820956824 PMC 7488807 · doi ↗ · pubmed ↗
- 2Smith LE , Potts HWW , Amlôt R , et al. Adherence to the test, trace, and isolate system in the UK: results from 37 nationally representative surveys. Br Med J 2021;372:n 608. DOI: 10.1136/bmj.n 608.PMC 801026833789843 · doi ↗ · pubmed ↗
- 3Mowbray F , Woodland L , Smith LE , et al. Is my cough a cold or COVID? A qualitative study of COVID-19 symptom recognition and attitudes toward testing in the UK. Front Public Health 2021;9:716421. DOI: 10.3389/fpubh.2021.716421.34485238 PMC 8416344 · doi ↗ · pubmed ↗
- 4Woodland L Mowbray F Smith LE , et al. What influences whether parents recognise COVID-19 symptoms, request a test and self-isolate: a qualitative study. PLOS ONE 2022;17:e 0263537.10.1371/journal.pone.0263537 PMC 886565335196349 · doi ↗ · pubmed ↗
- 5Prime Minister’s Office DS. Slides, datasets and transcripts to accompany coronavirus press conferences. 2020.