Natural history of coronary inflammatory activity in spontaneous coronary artery dissection: insights from serial pericoronary adipose tissue analysis
Satoshi Kitahara, Yu Kataoka, Yusuke Fujino

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
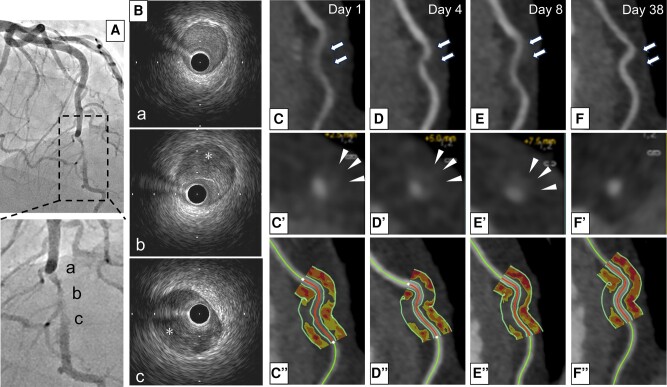 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Issues in Pregnancy · Cardiovascular Disease and Adiposity · Coronary Artery Anomalies
A 53-year-old woman was hospitalized due to ST-elevation myocardial infarction. Emergent coronary angiography revealed a severe stenotic lesion in her left anterior descending artery (Panel A and see Supplementary material online, Video 1). Intravascular ultrasound imaging revealed a narrowed true lumen compressed by intramural haematoma (Supplementary material online, Video 2 and Panel B, a–c). She was diagnosed with spontaneous coronary artery dissection (SCAD). Following the commencement of medical therapies (aspirin 100 mg, bisoprolol 1.25 mg), this lesion was serially evaluated by coronary computed tomography angiography. At Day 1, diffuse lumen narrowing and wall thickening were observed. Furthermore, this lesion exhibited a high pericoronary adipose tissue (PCAT) attenuation [−73 Hounsfield unit (HU)], suggesting an elevated coronary inflammatory activity (Panel C). These features still continued to exist at Days 4 (−75 HU) and 8 (−78 HU) (Panels D and E). However, at Day 38, in addition to the disappearance of diffuse narrowing and wall thickening, PCAT attenuation improved (−91 HU) (Panel F).
Recent studies reported the association of SCAD with an increased perivascular inflammation. In our case, in addition to diffuse narrowing and wall thickening, high PCAT attenuation remained to exist by Day 8, and then these features improved at Day 38. Our observations show natural history of SCAD-related disease activity under medical therapies. Of note, continuing coronary inflammatory activity was observed by Day 8. This indicates a residual inflammation in the acute/sub-acute phase, which may be a potential substrate causing recurrence of SCAD. Further studies are required to elucidate whether evaluation of coronary inflammation could stratify a risk of recurrence in patients with SCAD.
Supplementary Material
ytae115_Supplementary_Data