Case Report: Case report: Rapidly progressing tooth wear dominated by intrinsic and extrinsic erosion
Shivaughn Marchan, Estévan Ollivierra, Alexa Diaz, Rochard Santo, Andrew Eder, Alex Milosevic

TL;DR
A 46-year-old man experienced rapid tooth wear mainly due to acid erosion from both internal and external sources, requiring combined dental and medical care.
Contribution
This case report highlights a rare and rapid instance of tooth wear dominated by intrinsic and extrinsic erosion with unique clinical features.
Findings
The patient's tooth wear was primarily due to intrinsic and extrinsic erosion, not abrasion or attrition.
The lack of compensation in opposing teeth simplified restorative dental management.
The case emphasizes the need for a multidisciplinary approach combining dental and medical treatment.
Abstract
Tooth wear is multi-factorial presenting as a combination of abrasion, attrition, and erosion. This case report represents a case of combined tooth wear in a 46-year-old Indo-Trinidadian male, with a predominant erosive component with both the clinical signs and features of intrinsic and extrinsic erosion. This patient case is unique since the wear predominated by dental erosion has occurred rapidly evidenced by the physical clinical appearance of a lack of compensation and the upper left premolars and molars relatively unaffected by the overall effects of tooth wear. This lack of compensation, where opposing teeth have not supra-erupted to maintain inter-arch stability, and the maintenance of occlusal vertical dimension on the left due to the non-worn posterior maxillary teeth, provides the benefit of simplifying subsequent restorative management. The medical and diet history…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4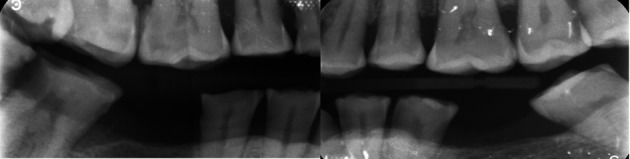 Figure 5
Figure 5- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Erosion and Treatment · Dental materials and restorations · Temporomandibular Joint Disorders
Introduction
Tooth wear or tooth surface loss is defined as the irreversible loss or degeneration of hard dental tissue caused by non-bacterial means. ^ 1 ^ 20% of tooth wear is multifactorial, presenting clinically as a combination of dental erosion, attrition, and abrasion. ^ 1 ^ Research on a Trinidadian population attending a dental teaching hospital concluded that 72% of the studied population suffered from mild, moderate, or severe wear, with 52% exhibiting mild wear. ^ 2 ^ Erosive wear, which causes a softening of tooth enamel by endogenous or exogenous acids can exacerbate and accelerate wear caused by attrition and abrasion with clinical signs of chipping or fracture of incisal edges or hard tissue loss at the cervical margins of teeth respectively. ^ 3 ^ Age and sex are determinants in the prevalence and severity of erosive tooth wear. ^ 4 ^ Erosion of dental tissue can be further diagnosed as intrinsic or extrinsic erosion depending on the source of acid causing tooth wear and the clinical pattern of wear. ^ 3 ^ Intrinsic wear, clinically evident as cupped-out occlusal lesions or affecting the palatal surface of upper anterior teeth, is normally associated with medical conditions such as gastroesophageal reflux disease (GERD), chronic vomiting associated with pregnancy, alcoholism, or eating disorders. ^ 3 ^ Conversely, extrinsic erosion affects facial or buccal surfaces and is commonly associated with exogenous acids found in the consumption of citrus fruits and a variety of beverages. ^ 5 ^ Additionally, a “swish and swallow” pattern of beverage consumption can exacerbate extrinsic erosion. ^ 6 ^
Case presentation
A 46-year-old Indo-Trinidadian male agriculturist, of South Asian descent, presented to a clinic of a dental teaching hospital with two main complaints of pain associated with tooth 8 and his enamel wearing away on several teeth, which started only three years previously ( Figure 1). The patient’s medical history uncovered frequent consumption of citrus fruits, particularly oranges and grapefruits where the anterior teeth would be embedded into a cut face of the peeled fruit as part of his job. Specifically, he was a budder and grafter of citrus plants at a government-run nursery and often tasted citrus fruit to determine the quality and taste profile of grafted citrus fruit. The patient’s history also revealed frequent consumption of a local delicacy of fresh pickled green fruit referred to as “chow”. The patient suspected undiagnosed GERD, which he referred to as heartburn, and was currently self-medicating with various dosages of omeprazole, between 20mg and 40mg daily, on an intermittent basis when the symptoms of heartburn presented. The patient admitted to social drinking on the weekends mainly with the consumption of Pilsner beer which he believed exacerbated his heartburn. When asked about vomiting after his beer consumption, he noted this happened only occasionally. On questioning, the patient confirmed no other teeth were painful or sensitive currently, but he has suffered from generalized sensitivity in the past. Tooth 8 was tender to vertical percussion and was tender on palpation of the root apex. Clinical examination revealed a stoma on the attached mucosa at the apex of this tooth. A periapical radiograph was taken using a paralleling technique. An intra-oral X-ray tube (Carestream. Kodak) using 65KVp and 20mAs was used to expose a size 2 periapical phosphor plate sensor (Carestream, Kodak). This periapical radiograph confirmed a periradicular radiolucency consistent with a pulpal diagnosis of necrosis and chronic periradicular periodontitis.
Right buccal view of the worn teeth showing lack of occlusal compensation.
Other non-tooth wear clinical findings/diagnoses
Physical clinical examination revealed teeth 19, 30, and 17 were previously extracted. Bitewing radiographs were also taken on the patient’s initial visit, using a Size 2 periapical phosphor plate sensor in a positioning device (XCP, Rinn). The X-ray beam produced by the intra-oral X-ray tube (Carestream, Kodak) was positioned through the posterior tooth contacts a 10-degree vertical angulation. Proximal caries was noted clinically and on bitewing radiographs of several teeth on both the upper and lower arches ( Figure 5). Gross deposits of generalized supra- and sub-gingival calculus were noted. Despite caries being present on both the right and left quadrants, larger carious lesions were noted on the right quadrants where the wear was more severe.
Clinical presentation of tooth wear lesions
On physical examination at the time of initial patient presentation, the surfaces of all remaining teeth, except the upper left molars and premolars, showed moderate to severe wear involving both enamel and dentine surfaces. Cupped-out erosive lesions were noted on the occlusal surface of mandibular and maxillary molars and the premolars ( Figure 2, Figure 4). Interestingly the premolars and molars on the upper left side showed only mild occlusal cupping ( Figure 2). Additionally, the palatal surfaces of teeth 6 and 11 showed evidence of intrinsic erosion ( Figure 2). There were moderate to severe erosive lesions involving the cervical to middle thirds of the facial surfaces of teeth 5,6,7,8, and 9 ( Figure 1). Tooth 8 had the deepest facial lesion involving the entire facial surface of the tooth. These upper teeth had lost coronal tooth height with fractures of the incisal edges. Following this same pattern, milder wear was noted on the facial aspect of teeth 10 and 11 with two to three striations noted horizontally across the facial surface ( Figure 3). The rate of wear seems to have progressed quickly with no occlusal compensation and an absence of any occlusal contacts between the maxillary and mandibular teeth in the anterior sextants and right quadrants. The inter-occlusal space provided an opportunity to simplify the restorative rehabilitation of the worn teeth. Teeth 26, 27, 28, and 29 showed tooth surface loss from the cervical third of these teeth towards the middle third, with tooth 29 having the entire facial surface of the tooth involved ( Figure 1). Cupping was noted on the incisal edges of the lower incisors ( Figure 4).
Maxillary view showing pronounced occlusal cupping on the right quadrants.
Anterior view of the worn teeth showing facial notching.
Mandibular view showing pronounced occlusal cupping on all remaining teeth and carious lesions on the lower right.
Bitewing radiographs confirming proximal caries.
Discussion
The patient exhibited wear of multifactorial etiology with clinical signs of attrition, abrasion, and erosion with a predominant erosive component. Of particular concern was a clinical pattern of tooth surface loss that indicated both intrinsic and extrinsic erosion occurring at an accelerated rate evidenced by a lack of compensation and necrosis of the pulp of tooth 8. The proposed mechanism of tooth loss from the incisal edges of the upper anterior teeth occurred because of tooth-to-tooth contact on incisal edges which may have been already thinned because of both facial and palatal wear. Tooth brushing of softened dental enamel continuously subjected to both endogenous and exogenous acids could result in abrasive-erosive type lesions noted on the buccal surfaces of the right side.
Caries is not a normal or prominent feature in the clinical presentation of tooth surface loss of a predominant erosive wear. ^ 7 ^ However, loss or slipping of proximal contacts, noted with rapid tooth wear could predispose patients to food packing, plaque trapping, and eventual caries formation. ^ 8 ^ This is the working hypothesis in this case where concomitant wear and caries were noted. Alternatively, a change in the composition and properties of the saliva could account for both the rapid erosive tooth wear noted and the concomitant caries experience. ^ 9 ^ The poor oral hygiene evidenced by the gross deposits of calculus could have been caused by long periods of dentine sensitivity. ^ 3 ^ Chronic dentine sensitivity may lead to less than optimum tooth brushing to prevent an exacerbation of sensitivity.
Presentation of severe clinical tooth surface loss together with the gleaned medical history must signal to the dental clinician a need for multi-disciplinary management of the patient. This patient requires investigation and management by a gastroenterologist since the severity of intrinsic erosion is directly related to contact time with endogenous gastric acid. ^ 10 ^ Medical practitioners may deduce the frequency and duration of GERD by assessing tooth surface loss. ^ 10 ^ Such investigation is warranted since a recent systematic review concluded there was a constant correlation between dental erosion and GERD. ^ 11 ^ Physicians, when suspecting GERD as a differential diagnosis must examine the condition of a patient’s dentition for the signs of dental erosion. ^ 12 ^
The patient also requires dietary counseling to reduce the frequency and peculiar habit of citrus consumption. Such counseling can be effective if a relationship between the patient’s presenting complaint of tooth wear and the clinical appearance and pattern of the wear is linked to the type of fruit consumed as well as the peculiar habit of consumption. ^ 5 ^ Citrus consumption is positively related to the development of erosive lesions. ^ 5 ^ ^,^ ^ 13 ^ In linking the clinical appearance of the worn teeth, in part, to the dietary consumption of citrus, counseling can be patient-specific and more likely to be adopted as a preventive strategy in curtailing further tooth surface loss. ^ 13 ^
Dental management
Following medical referral and the start of medical and dietary intervention, dental management would include basic periodontal therapy including scaling of teeth and stabilization of active carious teeth, and initiation of root canal treatment on tooth 8. Directly placed composite restorations are planned for the severely worn teeth conforming to the patient’s occlusion. ^ 14 ^ This restorative strategy can be used given the general maintenance of the patient’s occlusal vertical dimension and lack of compensation providing interocclusal space for sufficient bulk of restorative material while conforming to the existing occlusal scheme. ^ 3 ^ Regular reviews including radiographic, visual, and photographic assessments, following dental management, are important to monitor dentition for any further signs of wear and to facilitate ongoing assessment of restorations for repair or replacement. ^ 3 ^ ^,^ ^ 15 ^ Given that this patient presented with several active carious lesions, review at 4-6 monthly intervals is recommended at which time the dentition can be monitored for further signs of tooth wear.
Ethics and consent
Written informed consent for publication of their clinical details and clinical images and radiographs was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith B Knight J : A comparison of patterns of tooth wear with aetiological factors. Br. Dent. J. 157:16–19. Unit 2. 10.1038/sj.bdj.4805401 6588978 · doi ↗ · pubmed ↗
- 2Rafeek R Marchan S Eder A : Tooth surface loss in adult subjects attending a university dental clinic in Trinidad. Int. Dent. J. 2006;56(4):181–186. 10.1111/j.1875-595X.2006.tb 00092.x 16972391 · doi ↗ · pubmed ↗
- 3Eder A Faigenblum M : Tooth Wear: An Authoritative Reference For Dental Professionals and Students: Springer. Nature. 2022. 10.1007/978-3-030-86110-0 · doi ↗
- 4Stangvaltaite-Mouhat L PūrienėA Stankeviciene I : Erosive tooth wear among adults in Lithuania: a cross-sectional National Oral Health Study. Caries Res. 2020;54(3):283–291. 10.1159/000509872 32937621 · doi ↗ · pubmed ↗
- 5Bamise CT Dinyain VE Kolawole KA : Dental erosion due to lime consumption; review of literature and case report. East Afr. J. Public Health. 2009;6(2):141–143. 10.4314/eajph.v 6i 2.51733 20000018 · doi ↗ · pubmed ↗
- 6Fusain KS : Erosive potential of drinks consumed in Dubai (Doctoral Dissertation). 2019.
- 7Tschammler C Simon A Brockmann K : Erosive tooth wear and caries experience in children and adolescents with obesity. J. Dent. 2019;83:77–86. 10.1016/j.jdent.2019.02.005 30825568 · doi ↗ · pubmed ↗
- 8Kaidonis JA : Tooth wear: the view of the anthropologist. Clin. Oral Investig. 2008;12(Suppl 1):21–26. 10.1007/s 00784-007-0154-8 17938977 PMC 2563149 · doi ↗ · pubmed ↗