Characteristics and Outcomes of Patients Receiving a Second Rescue Valve During Transcatheter Aortic Valve Implantation
Henrik Bjursten, Sasha Koul, Pétur Pétursson, Jacob Odenstedt, Henrik Hagström, Jenny Backes, Niels Erik Nielsen, Andreas Rück, Jan Johansson, Stefan James, Magnus Settergren, Matthias Götberg, Troels Yndigen

TL;DR
This study examines the occurrence and outcomes of patients needing a second valve during a heart procedure called TAVI, finding that while short-term risks are high, long-term survival is similar to others.
Contribution
The study provides real-world data on the incidence and outcomes of second valve implantation during TAVI from a nationwide registry.
Findings
Rescue-AV occurred in 1.3% of TAVI patients.
30-day mortality was 15.2% for rescue-AV patients compared to 1.6% in the control group.
Survivors of the 30-day period had similar long-term survival rates to the control group.
Abstract
Transcatheter aortic valve implantation (TAVI) has become a safe procedure. However, complications occur, including uncommon complications such as valve malposition, which requires the implantation of an additional rescue valve (rescue-AV). The aim was to study the occurrence and outcomes of rescue-AV in a nationwide registry. The Swedish national TAVI registry was used as the primary data source, where all 6706 TAVI procedures from 2016 to 2021 were retrieved. Nontransfemoral access and planned valve-in-valve were excluded. In total, 79 patients were identified as having had a rescue-AV, and additional detailed data were collected for these patients. This dataset was analyzed for any characteristics that could predispose patients to a rescue-AV. The outcome of patients receiving rescue-AV also was studied. Of the 5948 patients in the study, 1.3% had a rescue-AV. There were few…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
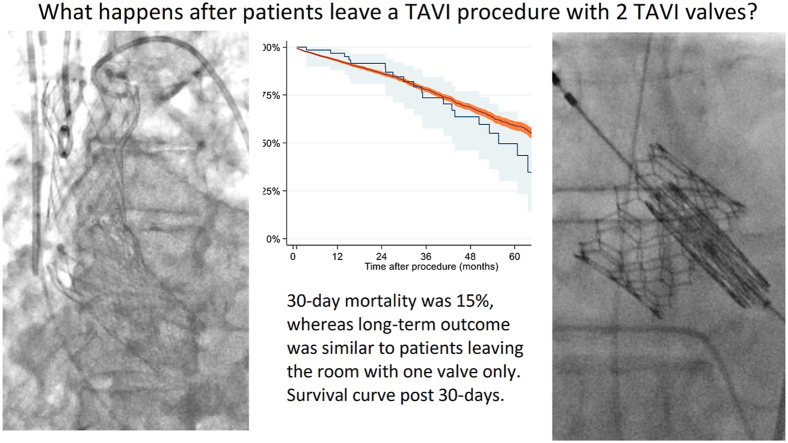 Figure 1
Figure 1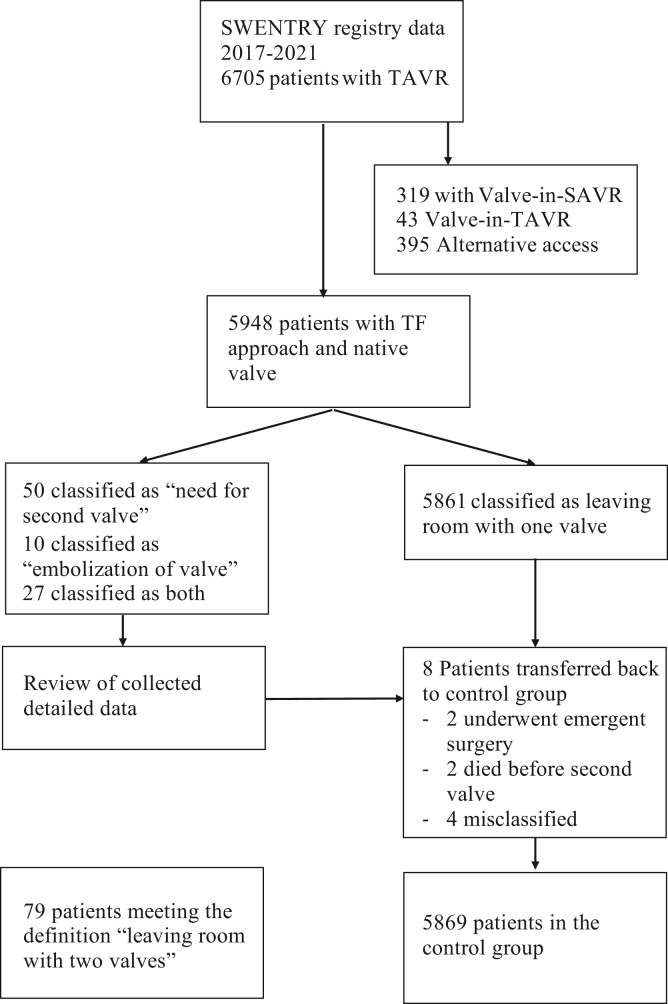 Figure 2
Figure 2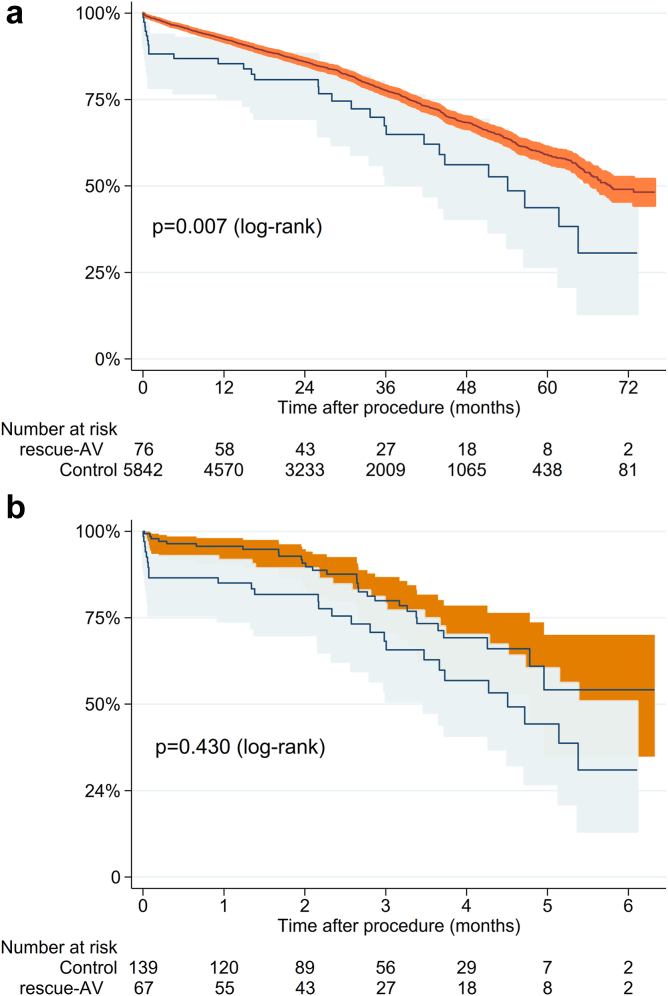 Figure 3
Figure 3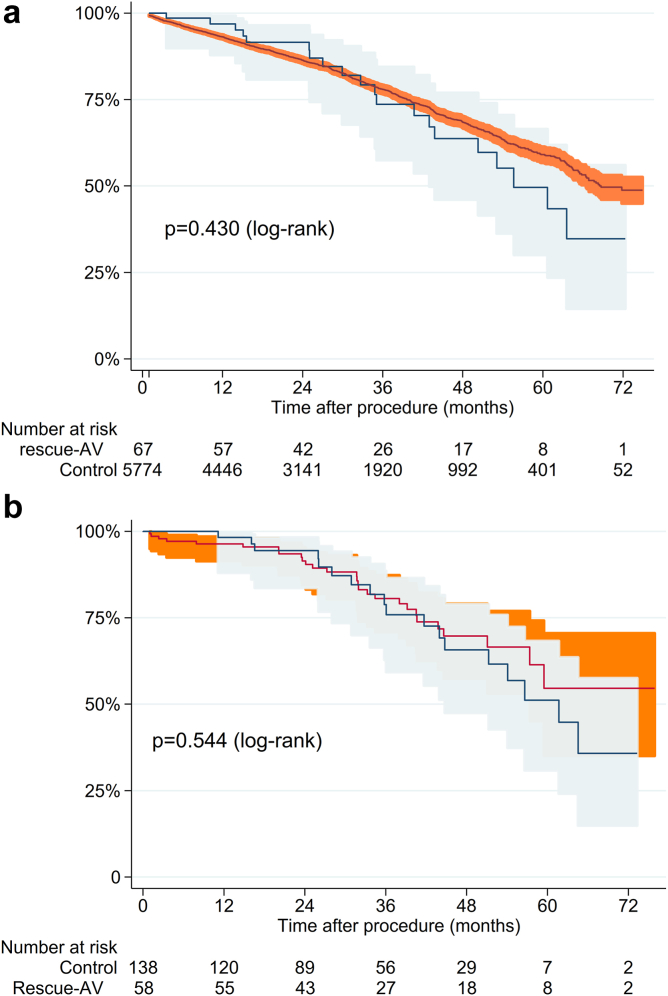 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
Introduction
Transcatheter aortic valve implantation (TAVI) has revolutionized the care of patients with aortic stenosis, and indications have expanded to patients who have traditionally been treated with surgical aortic valve replacement (SAVR).1, 2, 3 Recent studies have shown similar or improved short-term and medium-term outcomes for TAVI compared with SAVR.2^,^3
Still, TAVI is associated with uncommon complications not seen in surgery, such as femoral complications, coronary artery occlusion, and mechanical complications caused by the delivery system.4 In addition, the TAVI valve may not be delivered in the exact intended position or may even end up in an ectopic position after valve embolization.5^,^6
A recent study described the occurrence of TAVI valve embolization in a large cohort and showed a reasonable short-term outcome.6 These findings were confirmed in a subsequent smaller study.5 A less severe complication is valve malpositioning where the valve is still anchored in the aortic valve but positioned too high or too low. This condition may require a second valve to secure the first or to reduce paravalvular leakage.5^,^7 All these studies have a mix of first-generation and second-generation valves and report up to 1-year follow-up with an acceptable outcome.
Therefore, the present study aimed to investigate cases where the patient left the procedure with more than 1 valve, either due to valve embolization or malpositioning, in a cohort with a vast majority of second-generation valves. The study is a nationwide cohort study comprising all TAVIs performed in Sweden during a 6-year period. The main objective was to compare the characteristics and long-term outcomes of patients needing a rescue additional valve (rescue-AV) to a control group of TAVI patients during the same time period.
Methods
Study Design
This is a retrospective nationwide follow-up study of all patients who underwent TAVI in Sweden from January 2016 to December 2021. The initial data source was the National TAVI registry SWENTRY (SWEdish traNscatheter cardiac intervention regisTRY), which is part of the SWEDEHEART registry (Swedish Web-system for Enhancement and Development of Evidence-based Care in Heart Disease Evaluated According to Recommended Therapies). It contains information on all TAVI procedures performed in the country and has a high degree of accuracy and coverage.8, 9, 10 The registries are coupled to the Swedish Population Registry with a 100% catchment of mortality. During the study period, a total of 6706 patients received TAVI. The rescue-AV study group was defined as patients “leaving the procedure with more than one valve”. From this study group, 1 patient was excluded due to missing data, 362 patients were excluded because of planned Valve-in-Valve, and 395 patients were excluded due to nontransfemoral access (Figure 1). From this dataset, we selected patients who were marked as “Need for second valve” (50 patients), “valve embolization" (10 patients), or both (27 patients). We then contacted all 8 centers performing TAVI in Sweden and requested a review of these 87 patients and detailed information through a structured questionnaire. Eight of these 87 patients were then excluded from the rescue-AV study group (4 patients had the first valve retrieved before implantation of the second valve, 2 patients with embolized valve suffered instant death before receiving a second valve, and 2 patients with an embolized valve went to surgery); these patients were included in the control group instead. The control group consisted of all patients who underwent TAVI with only 1 valve via transfemoral access during the same period. The study was approved by the National Ethical Review Board in Sweden (registration numbers 2017/995 and EPN 2019/0584). The study is reported according to the STROBE guidelines.11Figure 1Flow chart of study design. Flow chart depicting study patient selection from SWENTRY registry.Abbreviation: SAVR, surgical aortic valve replacement; SWENTRY, SWEdish traNscatheter cardiac intervention regisTRY; TAVR, transcatheter aortic valve replacement; TF, transfemoral.
Statistical Analysis
Categorical data are presented as numbers (percent of the population), and continuous variables are presented as mean ± standard deviation. For comparisons between groups, the Chi-square test was used for categorical data and Student’s t-test for continuous data. Logistic regression was used to identify risk factors associated with rescue-AV. Propensity score matching was employed using the nearest neighbor method with a 1:2 matching on the following variables: age, gender, serum creatinine, hypertension, diabetes, peripheral vascular disease, NYHA class, aortic valve area (AVA), bicuspid valve (Supplemental Material). Kaplan–Meier curves were used to show survival over time, and survival between groups was tested using a Log-rank test. A separate analysis of survival past 30 days also was performed (Landmark analysis). Statistical testing was performed with Stata ver. 17 (StataCorp, College Station, TX, USA)
Results
Seventy-nine (1.3%) of 5948 patients had a rescue-AV according to the definition of this study (Figure 1). Demographics were similar between the study group (rescue-AV) and the control group. However, there was a significant difference in aortic valve area, where the control group had an aortic valve area (AVA) of 0.70 ± 0.19 cm^2^ and the rescue-AV group had an AVA of 0.63 ± 0.19 cm^2^ (p = 0.003, Table 1) and almost twice as many were labeled as urgent procedures (20.3 vs. 11.3%, p = 0.013, Table 1). Only a small fraction in both groups had a first-generation valve (0.5%). During the procedure, the rescue-AV group had almost twice the fluoroscopy time (1975 ± 1034 seconds vs. 1024 ± 617 seconds, p < 0.001). They also required almost double the amount of contrast (111.6 ± 62.2 ml vs. 60.7 ± 41.8 ml, p < 0.001, Table 2). In the rescue-AV group, 72% (57 of 79) had a self-expandable valve, whereas in the control group, 54% (3164 of 5869) had self-expandable valve (p < 0.001, Table 2).Table 1. DemographicsDemographicsAll (n = 5948)Control (n = 5869)Rescue-AV (n = 79)OR (95% CI)Age (years)81.1 ± 6.881.1 ± 6.781.5 ± 7.51.00 (0.98-1.04)Female gender2738 (46.0%)2702 (46.0%)36 (45.6%)0.98 (0.61-1.57)Height (cm)168.7 ± 9.5168.8 ± 9.5167.7 ± 9.10.99 (0.97-1.01)Weight (kg)76.6 ± 16.376.6 ± 16.275.1 ± 20.60.99 (0.98-1.00)Body mass index26.8 ± 5.026.8 ± 5.026.4 ± 5.70.98 (0.94-1.03)Serum creatinine (μmol/L)100.6 ± 59.3100.7 ± 59.696.1 ± 32.51.00 (0.99-1.00)Hypertension4591 (77.2%)4526 (77.1%)66 (82.3%)1.38 (0.76-2.67)Diabetes1531 (25.7%)1512 (25.8%)19 (24.1%)0.91 (0.51-1.55)Previous cardiac surgery693 (11.7%)682 (11.6%)11 (13.9%)1.23 (0.58-2.35)Recent myocardial infarction217 (3.6%)214 (3.6%)3 (3.8%)1.04 (0.21-3.20)Previous PCI1587 (26.7%)1572 (26.8%)15 (19.0%)0.64 (0.33-1-14)COPD948 (15.9%)935 (15.9%)13 (16.5%)1.03 (0.52-1.91)Previous stroke663 (11.1%)649 (11.1%)14 (17.7%)1.73 (0.89-3.14)Critical preoperative state129 (2.2%)126 (2.1%)3 (3.8%)1.79 (0.36-5.58)Peripheral vascular disease736 (12.4%)724 (12.3%)12 (15.2%)1.27 (0.62-2.39)Reduced mobility745 (12.5%)738 (12.6%)7 (8.9%)0.67 (0.26-1.47)Atrial fibrillation2180 (36.7%)2155 (36.7%)25 (31.6%)0.80 (0.47-1.30)Steroid treatment417 (7.0%)412 (7.0%)5 (6.3%)0.89 (0.28-2.19)History of malignancy606 (10.2%)594 (10.1%)12 (15.2%)1.59 (0.78-2.99)Pacemaker bearer609 (10.2%)599 (10.2%)10 (12.7%)1.27 (0.58-2.50)Urgency Elective procedure5224 (87.8%)5162 (88.0%)63 (78.5%)Ref Urgent procedure679 (11.4%)663 (11.3%)16 (20.3%)2.01 (1.15-3.50) Acute procedure1173 (19.7%)1167 (19.9%)6 (7.6%)1.90 (0.26-13.9)NYHA class NYHA I159 (2.6%)157 (2.7%)2 (2.5%)0.82 (0.20-3.42) NYHA II1173 (19.7%)1167 (19.8%)6 (7.6%)0.33 (0.14-0.78) NYHA III4029 (67,7%)3968 (67.6%)61 (77.2%)Ref NYHA IV581 (9.8%)571 (9.7%)10 (12.6%)1.14 (0.582.23)LVEF LVEF normal3899 (65.6%)3845 (65.5%)55 (68.4%)Ref LVEF slightly depressed799 (13.4%)794 (13.5%)5 (6.3%)0.45 (0.18-1.12) LVEF moderately depressed801 (13.5%)789 (13.4%)12 (15.2%)1.08 (0.58-2.03) LVEF severely depressed429 (7.2%)421 (7.2%)8 (10.1%)1.35 (0.64-2.86)Bicuspid Valve453 (7.7%)444 (7.6%)9 (12.1%)1.57 (0.68-3.18)Mean annular diameter24.6 ± 2.324.6 ± 2.324.6 ± 2.51.01 (0.91-1.11)Mean aortic gradient (mmHg)47.4 ± 14.147.4 ± 14.147.4 ± 14.61.00 (0.98-1.01)AVA (cm^2^)0.71 ± 0.170.71 ± 0.160.64 ± 0.150.09 (0.02-0.39)Comparison between control group (patients with 1 TAVI) and rescue-AV group (patients receiving more than 1 valve due to malpositioning or embolization).Abbreviations: AVA, aortic valve area; CI, confidence interval; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; OR, odds ratio.Table 2. Valve distributionValve ModelAll (5948)Control (5869)Rescue-AV (79)Abbott Navitor3838Abbott Portico21820513Boston Acurate neo99798710Boston Acurate neo24404373Boston Acurate TA11Boston Lotus77752Boston Lotus Edge4545Edwards Sapien 31600158713Edwards Sapien 3 Ultra9909837Edwards Sapien and Sapien XT44Medtronic CoreValve23185Medtronic Evolut PRO3493427Medtronic Evolut PRO Plus11Medtronic Evolut R1154113519Meril MyVal1111SEV3232317557BEV2716269422Valve distribution for the entire group, control group and rescue-AV (patients receiving more than 1 valve due to malpositioning or embolization).Boston Lotus is included in the BEV group. Distribution of SEV between groups yields a p-value p < 0.001.Abbreviations: BEV, balloon expanding valve; SEV, self-expanding valve.
At 30-day follow-up, the rescue-AV group had a higher mortality (15.2 vs. 1.6%, p < 0.001), a larger proportion of stroke (15.2 vs. 1.5%, p < 0.001) and minor stroke (1.3 vs. 0.1%, p = 0.01), more patients in need of circulatory support (2.5 vs. 0.1%, p < 0.001), more unplanned general anesthesia (3.8 vs. 0.9%, p = 0.01), a larger number of myocardial infarctions (1.3 vs. 0.2%, p = 0.02), more postprocedural infections (6.3 vs. 2.2%, p = 0.02), and more new renal replacement therapy (1.3 vs. 0.1%, p < 0.001). For the 70 patients in the rescue-AV group who had an echocardiographic assessment, there was a higher frequency of moderate paravalvular regurgitation (7.5 vs. 2.8%, p = 0.01) as well as severe paravalvular regurgitation (1.3 vs. 0.1%, p = 0.001). There were no differences in postoperative peak gradient or creatinine at discharge (Table 3).Table 3. Outcome dataIntraprocedural dataEntire cohortPropensity matched cohortControl (n = 5869)Rescue-AV (n = 79)p valueControl (n = 140)Rescue-AV (n = 70)p valueContrast (ml)60.7 ± 41.8112.3 ± 62.3<0.00161.3 ± 49.3113.3 ± 63.0<0.001Fluoroscopy time (min)17.1 ± 10.333.1 ± 17.2<0.00118.5 ± 11.029.7 ± 17.1<0.001Predilatation3477 (59.2%)52 (64.6%)0.344283 (59.3%)43 (61.4%)0.7650Postdilatation1414 (24.1%)24 (30.4%)0.195137 (26.4%)18 (25.7%)0.9116Outcome 30 dControl (n = 5869)Rescue-AV (n = 79)p valueControl (n = 140)Rescue-AV (n = 70)p valueDeath within 30 d95 (1.6%)12 (15.2%)<0.0012 (1.4%)12 (17.1%)<0.001Acute cardiac surgery9 (0.2%)0 (0.0%)0.72760 (0.0%)0 (0.0%)1.0000Circulatory support5 (0.1%)2 (2.5%)<0.0010 (0%)2 (2.9%)0.0447Unplanned general anesthesia52 (0.9%)3 (3.8%)0.00721 (0.7%)3 (4.3%)0.0742Bleeding180 (3.1%)6 (8.5%)0.01174 (2.9%)6 (9.7%)0.0419Major stroke79 (1.3%)12 (15.2%)<0.0012 (1.4%)11 (15.7%)<0.001Minor stroke8 (0.1%)1 (1.3%)0.01031 (0.7%)1 (1.4%)0.6153Myocardial infarction9 (0.2%)1 (1.3%)0.01650 (0%)1 (1.4%)0.1563Vascular complication86 (1.5%)3 (3.8%)0.09001 (0.7%)3 (4.3%)0.0742Infection needing treatment129 (2.2%)5 (6.3%)0.01401 (0.7%)5 (7.1%)0.0084New RRT4 (0.1%)1 (1.3%)<0.0010 (0%)1 (1.4%)0.1563New permanent pacemaker418 (7.1%)7 (8.9%)0.55129 (6.4%)7 (10%)0.1563Creatinine at discharge96.3 ± 63.389.0 ± 30.60.336584.7 ± 24.686.9 ± 29.30.5872AI grade<0.0010.4601 03144 (53.6%)35 (44.3%)0.101067 (47.9%)30 (42.9%) I2452 (41.8%)27 (34.2%)0.173462 (44.3%)25 (35.7%) II166 (2.8%)6 (7.6%)0.01209 (6.4%)5 (7.1%) III5 (0.1%)1 (1.3%)0.00100 (0%)0 (0%)Unknown102 (1.7%)10 (12.7%)<0.0012 (1.4%)10 (14.3%)Peak gradient (mmHg)18.6 ± 8.618.2 ± 7.40.727118.4 ± 7.816.6 ± 6.60.1899Mean gradient (mmHg)10.4 ± 5.29.8 ± 3.90.42109.8 ± 3.99.8 ± 4.00.9903Comparison of outcome between control groups (patients with 1 TAVI) and rescue-AV group (patients receiving more than 1 valve due to malpositioning or embolization) for both entire cohort and propensity score matched cohort.Abbreviations: AI, aortic insufficiency (no differentiation between central and paravalvular); RRT, renal replacement therapy.
Patients were followed for survival with a mean of 880 days (range 124-2309 days). The high 30-day mortality in the rescue-AV group affected the long-term survival negatively compared to the control group (p = 0.007, Figure 2). However, when a landmark analysis was performed looking at survival past 30 days, no significant difference was observed between the 2 groups (p = 0.430, Figure 3).Figure 2. Overall survival for the groups. Kaplan–Meier curve depicting survival for the rescue-AV (patients receiving more than 1 valve due to malpositioning or embolization) for the entire cohort (a) and propensity score cohort (b). Log-rank test showed a significant difference with p = 0.007 (entire cohort) and p = 0.027 (propensity score cohort).Figure 3. Landmark analysis after 30 days. Kaplan–Meier curve depicting survival for the rescue-AV group (patients receiving more than 1 valve due to malpositioning or embolization after 30 days) for entire cohort (a) and propensity score cohort (b). Log-rank test showed a nonsignificant difference with p = 0.430 (entire cohort) and p = 0.544 (propensity score cohort).
A propensity scored cohort was created, that managed to match 70 rescue-AV with 140 patients who left the room with 1 valve. In this analysis, rescue-AV had a 17.1% 30-day mortality compared to 1.4% for the control group (p < 0.001, Table 3). The rescue-AV cohort had more stroke (15.7 vs. 1.4%, p < 0.001), needed more circulatory support (2.9 vs. 0%, p = 0.05) and had more infections (7.1 vs. 0.7%, p = 0.008). Kaplan–Meier survival curves showed high initial mortality for the rescue-AV group, but the 30-day landmark analysis showed a similar long-term survival compared to the control group (Figure 3) among those who survived to 30 days.
The retrospective data capture for rescue-AV patients revealed that 11% had a bicuspid valve, 97% were in a stable hemodynamic situation before the procedure, 47% had their first valve in the annulus, 36% had embolized to the aorta, and 17% had embolized to the ventricle (Table 4). The majority (95%) received the second valve during the same procedure. Only 10% needed circulatory support after the procedure (3% had extracorporeal membrane oxygenator (ECMO) and 7% had inotropic support). The stroke rate was high, with 9% having had a major stroke and 8% having had a minor stroke.Table 4. Detailed outcomeCharacteristicAll (n = 79)Anchored in annulus (n = 50)Embolized valve (n = 29)Survived 30 d (n = 67)Died within 30 d (n = 12)p value30-d mortalityValve Morphology BAV Sievers 02 (3%)1 (2%)1 (3%)2 (17%)0.064∗ BAV Sievers 17 (9%)6 (12%)1 (3%)1 (8%) Tricuspid70 (89%)43 (86%)27 (93%)9 (75%)Hemodynamic condition Stable77 (97%)48 (96%)29 (100%)11 (92%) Low BP (SBP<100)1 (1%)1 (2%)0 (0%)0 (0%) Vasopressor1 (1%)1 (2%)0 (0%)1 (8%)First Valve Accurate12 (15%)8 (16%)4 (14%)0 (0%)0.320 Evolut34 (43%)23 (46%)11 (38%)5 (42%) Lotus4 (5%)4 (8%)0 (0%)0 (0%) Portico13 (16%)7 (14%)6 (21%)3 (25%) Sapien 316 (20%)8 (16%)8 (28%)4 (33%)Embolization of the first valve No embolization50 (63%)50 (100%)0 (0%)7 (58%)0.312† To the aorta25 (32%)0 (0%)25 (86%)4 (33%) To the ventricle4 (5%)0 (0%)4 (14%)1 (8%)Second valve Evolut36 (46%)25 (50%)11 (38%)5 (45%) Lotus2 (3%)2 (4%)0 (0%)0 (0%) Portico12 (15%)7 (14%)5 (17%)3 (27%) Sapien 328 (35%)16 (32%)12 (41%)3 (27%) Unknown1 (1%)0 (0%)1 (3%)Placement of the first valve at the end of the procedure Anchored well in the annulus37 (47%)37 (74%)0 (0%)4 (33%)0.629 Ascending aorta with some anchoring13 (16%)13 (26%)0 (0%)3 (25%) Ascending aorta with no anchoring18 (23%)0 (0%)18 (62%)4 (33%) Descending aorta7 (9%)0 (0%)7 (24%)1 (8%) Left ventricle4 (5%)0 (0%)4 (14%)0 (0%)Circulatory support after the procedure ECMO2 (3%)1 (2%)1 (3%)2 (17%) Inotropic support6 (7%)5 (10%)1 (3%)3 (25%) No71 (90%)44 (88%)27 (93%)7 (58%)Cardiac surgery No76 (96%)48 (96%)28 (97%)9 (75%) Emergent (same day)2 (3%)2 (4%)0 (0%)2 (17%) Nonmergent (within a month)1 (1%)0 (0%)1 (3%)1 (8%)Discharge dataStroke Major stroke7 (9%)1 (2%)6 (21%)5 (56%) Minor stroke6 (8%)1 (2%)5 (17%)0 (0%) No61 (82%)43 (96%)18 (62%)4 (44%)AI grade 037 (51%)21 (46%)16 (59%)33 (50%) I29 (40%)18 (39%)11 (41%)26 (39%) II7 (10%)7 (15%)0 (0%)7 (11%) III0 (0%)0 (0%)LVEF at discharge >50%55 (70%)32 (64%)23 (79%)51 (76%) 30%-45%15 (19%)10 (20%)5 (18%)12 (18%) 15%-30%4 (5%)4 (8%)0 (0%)4 (6%) Unknown5 (6%)4 (8%)1 (3%)MI grade 028 (38%)13 (29%)15 (54%)25 (38%) I37 (51%)24 (53%)13 (46%)33 (50%) II8 (11%)8 (18%)0 (0%)8 (12%) III0 (0%)0 (0%)0 (0%)0 (0%)30-d mortality16.2%20.8%0 (0%)12 (100%)Comparison of characteristics for patients with rescue-AV (patients needing more than 1 valve due to malposition or embolization of the first valve). P-value denotes testing within a group to study if any characteristics significantly affects 30-day mortality.Abbreviations: AI, aortic insufficiency; BP, blood pressure; ECMO, extracorporeal membrane oxygenator; LVEF, left ventricle ejection fraction; MI, mitral insufficiency; SBP, systolic blood pressure.∗Comparison between Bicuspid and tricuspid.†comparison between embolized/ectopic valve and valve in the annulus for the first valve.
Patients who had an embolized valve had a 30-day mortality of 17% (5 of 29), and patients who had the first valve anchored in the annulus had a 30-day mortality of 14% (7 of 50, p = 0.823, Table 4).
The characteristics that were associated with high 30-day mortality were bicuspid Sievers 0 (100% mortality), vasopressor before procedure (100% mortality), ECMO or inotropic support after the procedure (100 and 75% mortality, respectively), cardiac surgery after the procedure (100% mortality), and major stroke (71% mortality).
For the patients who survived the 30-day mark, 11% had moderate PVL, and no one had severe PVL (Table 4). Mitral insufficiency and left ventricular ejection fraction were as expected in this patient category (Table 4).
Discussion
This retrospective study investigates the characteristics and survival of patients leaving their TAVI procedure with 2 valves due to a malpositioned or embolized first valve. A nationwide all-comers cohort spanning 6 years was used, and we found an incidence of 1.3% rescue-AV. The group that received a rescue-AV had a high 30-day mortality (15.2%), but after 30 days the survival curves were comparable with the control group.
One interesting finding of this study was that the rescue-AV group and control group were well-balanced in terms of demographics. The only difference found was that the rescue-AV group had a somewhat smaller AVA, while the mean aortic gradient did not differ. They also had twice the number of urgent procedures as compared to the control group. The apparent interpretation of this finding is that valve malpositioning is not directly related to patient factors, with the caveat that we did not examine the anatomy and calcium distribution in the annulus and left ventricular outflow tract. Previous studies have found that a horizontal aorta, aortic regurgitation, conical left ventricular outflow tract, bicuspid valve and, tall sinotubulur junction are predictors for valve malposition.5, 6, 7^,^12 We did not study the anatomy of the aortic root besides cuspidality and mean annular diameter, where we found no difference between the rescue-AV and control group. The occurrence of valve malpositioning is probably most dependent on factors during the procedure, such as failure to deploy at the correct annular level or pacing failure.6
We found a 1.3% prevalence of patients leaving the cath lab with more than 1 valve and a 15% 30-day mortality among these patients. Early reports from first-generation valves in the PARTNER I Trial showed a 2.5% frequency for rescue-AV and 1% rate of valve embolization.13^,^14 Kim et al6 studied the occurrence of valve embolization in a multicenter study and found a prevalence of 0.9% with an 18% 30-day mortality. Frumkin et al also studied valve embolization selectively and found an incidence of 1.4%.5 A recent study on an American TAVI cohort found a 2% incidence of needing a second valve with a 9.6% 30-day mortality. However, many received a second valve for a PVL indication, and only a small number in that study had an embolized valve.7 In the present study, 41% of the rescue-AV had an embolized first valve, which equates to a 0.5% incidence of valve embolization. All 3 previous studies found that self-expandable valves had a higher frequency of malpositioning, which is in agreement with the findings in our study. The previous studies reported a high frequency of first-generation valves while ours reported a low frequency of first-generation valves. If we analyze only the valves that are currently on the market today, we still find a 1.3% incidence of rescue-AV (Table 2). Still, more modern platforms, together with increasing operator experience, should explain the lower frequency in the present study.
One of the key findings of this study is the bimodal outcome for patients with a rescue-AV. While 30-day survival was worse than the control group, survival after the 30-day landmark was comparable to the control group, both before and after propensity score matching. Many of the early deaths were associated with other complications, such as the need for acute surgery, ECMO, or major stroke. The postprocedural echocardiogram of the survivors had a somewhat higher degree of grade I aortic insufficiency, but they were otherwise representative of a general TAVI cohort. The clinical interpretation of this finding is that if the patient had no further complications after the procedure, having had more than 1 TAVI valve implanted has little or no impact on the prognosis after 30 days until the end of follow-up (mean 880 days). To our knowledge, this report presents the longest follow-up of patients with rescue-AV.
Limitations
This is a registry-based retrospective study that has inherent weaknesses and strengths. First, as it is registry-based, the quality of the data entry will affect results. Also, we are limited to the data that was entered, and other undocumented variables could have led to a different result. To compensate for these shortcomings, we performed a structured validation of the patients who were classified as having either 2 valves or ectopic valves. This made us reclassify 8 patients. Compared to previous reports, the use of registry data was unable to identify the cause of the first valve malpositioning. A real-world, all-comers, nationwide dataset with robust follow-up for survival is, on the other hand, a very useful tool for describing the current status of a treatment as it is not disadvantaged by the attrition seen in randomized controlled studies or limited registries.
Conclusion
This study describes the characteristics and outcomes of patients requiring a second TAVI due to the initial TAVI valve being malpositioned or embolized. The frequency of this complication was 1.3% and was associated with a 15.2% 30-day mortality. For the patients who survived the first 30 days, subsequent outcomes were comparable to patients receiving 1 TAVI valve only.
Ethics Statement
The study was performed in accordance with the Declaration of Helsinki.
Funding
This work was supported by a regional government research fund under the agreement between the Swedish government and the county councils (ALF-agreement) and grants from the 10.13039/501100003793Swedish Heart-Lung Foundation. The study was approved by the National Ethical Review Board in Sweden (registration numbers 2017/995 and EPN 2019/0584).
Impact on Daily Practice
In the rare occurrence of having to implant a second TAVI valve during the same procedure, the treating doctor wants to know how the patient will fare after the procedure. We can conclude that if there is a second serious complication, then there is a high risk for a bad short-term outcome. But if the patient survives and does well during the hospital stay, the prognosis is good.
Disclosure Statement
HB: Consultancy and grants from Boston Scientific. AR: Consultancy and grants from Boston Scientific and Edwards Lifesciences. SJ: Consultancy from Medtronic. MS: Consultancy and advisory boards for Boston Scientific, Edwards Lifesciences, Abbott Vascular, and WL Gore. MG: Consultancy and grants from Boston Scientific. The other authors had no conflicts to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leon M.B.Smith C.R.Mack M.J.Transcatheter or surgical aortic-valve replacement in intermediate-risk patients N Engl J Med 374172016160916202704032410.1056/NEJ Moa 1514616 · doi ↗ · pubmed ↗
- 2Mack M.J.Leon M.B.Thourani V.H.Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients N Engl J Med 380182019169517053088305810.1056/NEJ Moa 1814052 · doi ↗ · pubmed ↗
- 3Popma J.J.Deeb G.M.Yakubov S.J.Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients N Engl J Med 380182019170617153088305310.1056/NEJ Moa 1816885 · doi ↗ · pubmed ↗
- 4Myers P.O.Dayan V.Szeto W.Y.Joint surgical associations (EACTS, LACES, ASCVTS, AATS, and STS) position statement regarding the VARC-3 definitions for aortic valve clinical research Ann Thorac Surg 11362022176717693530719210.1016/j.athoracsur.2021.12.004 · doi ↗ · pubmed ↗
- 5Frumkin D.Pietron M.Kind A.Valve embolization during transcatheter aortic valve implantation: incidence, risk factors and follow-up by computed tomography Front Cardiovasc Med 9202292874010.3389/fcvm.2022.928740 PMC 935566835935663 · doi ↗ · pubmed ↗
- 6Kim W.K.Schafer U.Tchetche D.Incidence and outcome of peri-procedural transcatheter heart valve embolization and migration: the TRAVEL registry (Transcathete R He Art Valve Embo Lization and Migration)Eur Heart J 40382019315631653123008110.1093/eurheartj/ehz 429 · doi ↗ · pubmed ↗
- 7Landes U.Witberg G.Sathananthan J.Incidence, causes, and outcomes associated with urgent implantation of a supplementary valve during transcatheter aortic valve replacement JAMA Cardiol 6820219369443400923610.1001/jamacardio.2021.1145 PMC 8135057 · doi ↗ · pubmed ↗
- 8Antman E.M.Improving care at the population and individual level: lessons from SWEDEHEART Eur Heart J 39422018377737793023969710.1093/eurheartj/ehy 519 · doi ↗ · pubmed ↗