Tamoxifen- and Triptorelin-Induced Major Hypertriglyceridemia: A Case Report
Widad Moussaoui, Fatima Zahra Lahmamssi, Hayat Aynaou, Houda Salhi, Hanan El Ouahabi

TL;DR
A breast cancer patient developed severe high triglycerides after taking tamoxifen and triptorelin, showing the need for lipid monitoring during treatment.
Contribution
Reports a rare case of major hypertriglyceridemia caused by the combined use of tamoxifen and triptorelin in a breast cancer patient.
Findings
The patient had triglyceride levels of 56 g/L after three months of treatment with tamoxifen and triptorelin.
Stopping the drugs and starting fenofibrate and diet reduced triglycerides to 2 g/L within a month.
The case highlights the need to monitor lipid profiles when using these drugs to prevent complications.
Abstract
Tamoxifen, a selective estrogen receptor modulator (SERM), can have harmful side effects, such as hypertriglyceridemia, which can lead to acute pancreatitis. Meanwhile, triptorelin is an analog of natural GnRH (GnRHa), which may cause a small but significant increase in cholesterol and triglyceride (TG) levels. We describe below the case of a patient with breast cancer treated with Patey’s operation, chemo-radiotherapy, and then with tamoxifen and triptorelin. After an exposure period of three months, she presented major hypertriglyceridemia at 56 g/L, total cholesterol at 13 g/L, LDL-cholesterol (LDL-C) at 4 g/L, and HDL at 0.25 g/L. The patient’s treatment was stopped by her oncologist. One month after starting an adapted diet and fenofibrate, her TG levels were reduced to 2 g/L. We could confirm from these results that tamoxifen and triptorelin certainly modify lipid metabolism,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
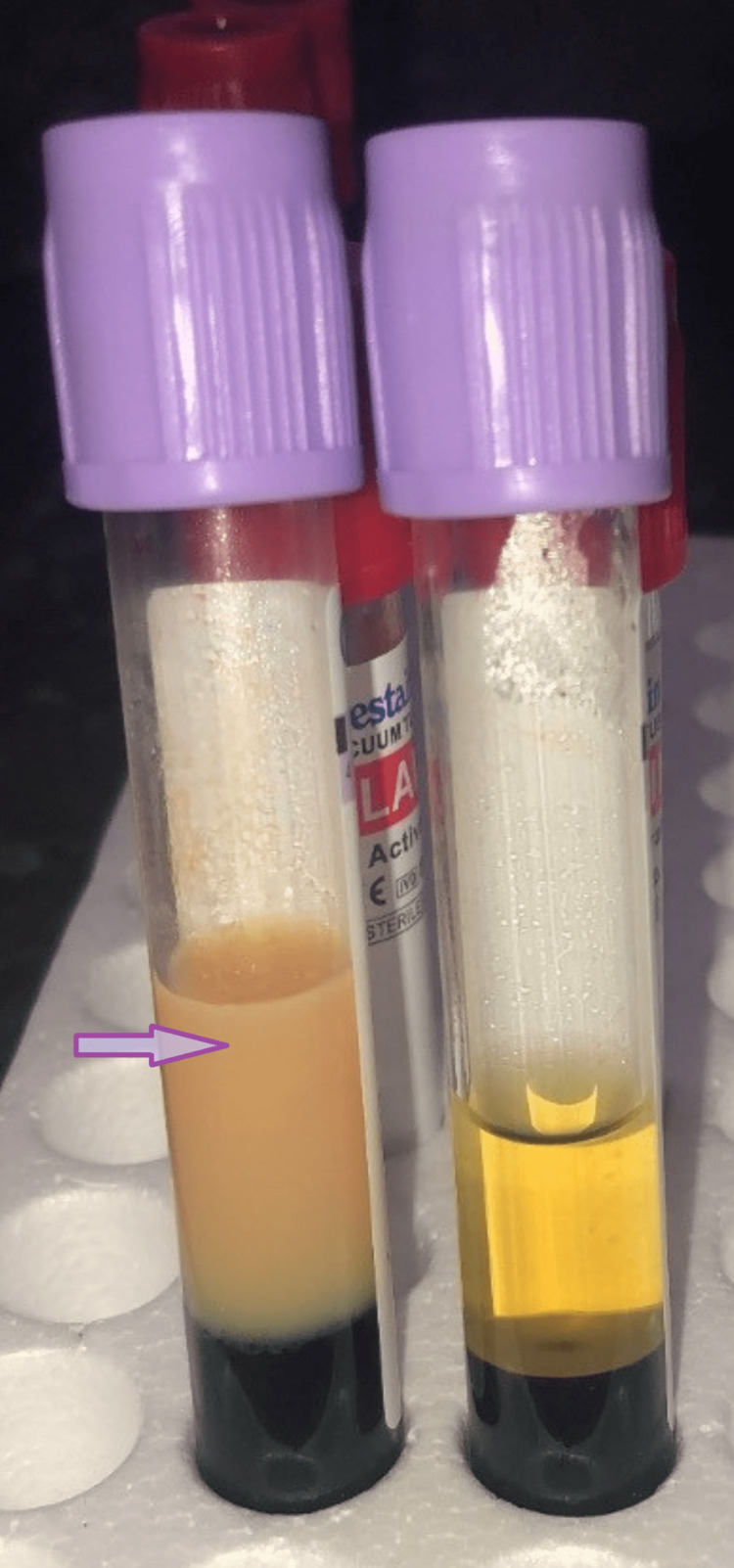 Figure 1
Figure 1 Figure 2
Figure 2| CT (g/L) (0.00-2.00) | TG (g/L) (<1.5) | HDL (g/L) (≥0.6) | LDL (g/L) (0.00-1.6) | CT/TG | TG/CT | |
| Oct 25, 2021: before surgery | 2.99 | 13 | 0.25 | 1.97 | 0.22 | 4.4 > 2.5; predominant hypertriglyceridemia |
| Aug 15, 2022: after one day of stopping SERMs | 13 | 56 | 0.25 | 4 | 0.23 | 4.3 > 2.5 |
| Aug 19, 2022: under fenofibrates | 7.05 | >47 | 0.28 | |||
| Aug 22, 2022 | 7.05 | >18.39 | 0.31 | |||
| Aug 24, 2022 | 7.05 | 14.2 | 0.37 | |||
| Aug 26, 2022 | 7.05 | 14 | 0.35 | |||
| Sep 26, 2022 | 1.75 | 2 | 0.37 | 0.98 |
| Tamoxifen | Triptorelin | |
| Time of occurrence of the event | Compatible time frame | Compatible time frame |
| De-challenge | Suggestive evolution | Suggestive evolution |
| Re-challenge | R0 | R0 |
| Chronological Score (C0-C3) | C2 | C2 |
| Semiotics | Semiology not suggestive of a pharmacological role | Semiology not suggestive of a pharmacological role |
| Non drug causes (confounders) | Etiological assessment | Etiological assessment |
| Laboratory investigations | L0 | L0 |
| Semiological Score (S1-S3) | S2 | S2 |
| Intrinsic Score (I0-I6) | C2S2 = I3 | C2S2 = I3 |
| Score | |
| Tamoxifen | Notable effect referenced in RCP and VIDAL: score B4 |
| Triptorelin | Notable effect referenced in RCP and VIDAL: score B4 |
| Author | Age (years) | History of dyslipidemia | Triglyceridemia (mg/dL) | Onset time (months) |
| Noguchi et al. [ | 34 | Unspecified | 3673 | 7 |
| Colls and George [ | 44 | Yes | 6984 | Unspecified |
| Elisaf et al. [ | 53 | Yes | 5200 | 8 |
| Artac et al. [ | 51 | Unspecified | 1344 | 12 |
| Lin et al. [ | 43 | Yes | 1040 | 24 |
| Alagozlu et al. [ | 46 | Yes | 900 | 12 |
| Sakhri et al. [ | 44 | Yes | 1180 | 12 |
| Brun et al. [ | 61 | Yes | 2790 | Unspecified |
| Isobe et al. [ | 47 | Unspecified | 1881 | 5 |
| Hozumi et al. [ | 49 | Unspecified | 1572 | 11 |
| Hozumi et al. [ | 54 | Unspecified | 1123 | 3 |
| Hozumi et al. [ | 49 | Unspecified | 2402 | 12 |
| Khabbal et al. [ | 44 | No | 1000 | 10 |
| Lipid | Before | After |
| Cholesterol (mmol/L) | 4.82 ± 0.14 | 5.31 ± 0.15** |
| Triglyceride (mmol/L) | 0.96 ± 0.06 | 1.11 ± 0.07* |
| HDL cholesterol (mmol/L) | 1.35 ± 0.05 | 1.41 ± 0.05 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Lipids, and Metabolism · Lipoproteins and Cardiovascular Health · Metabolism, Diabetes, and Cancer
Introduction
Hypertriglyceridemia is one of the most common lipid abnormalities that can cause acute pancreatitis. It usually occurs in patients with underlying disorders of lipoprotein metabolism and the presence of uncontrolled diabetes, alcohol misuse, or medication [1].
Tamoxifen and triptorelin are used in breast cancer therapy, with the disturbance of lipid balance as a possible side effect and bringing life-threatening complications, although it is rare.
We have encountered one case of asymptomatic major hypertriglyceridemia at 56 g/L in a patient with breast cancer, who was treated by Patey’s operation, chemo-radiotherapy, and then with tamoxifen and triptorelin. In this case report, we report the evolution of the lipid profile before and after the discontinuation of tamoxifen, the introduction of fenofibrate and an adapted diet, and the accountability of selective estrogen receptor modulators (SERMs) and triptorelin.
Case presentation
We report the case of a 43-year-old female patient presenting with a history of breast cancer, having undergone Patey’s operation, chemotherapy, and radiotherapy. She was put on SERMs (tamoxifen: 20 mg/day) and an analog of natural GnRH (Decapeptyl, triptorelin: one injection/week). Her sister had undocumented hypertriglyceridemia on hygienic and dietary measures (Mediterranean-style diet, physical activity, and weight loss). However, a strong heredity of type 2 diabetes was noted.
One year earlier, before the start of adjuvant hormonal treatment, her treating oncologist noted a lipid disturbance (CT: 2.99 g/L; TG: 13 g/L; HDL: 0.25 g/L; LDL: 1.97 g/L) during a systematic check-up. The patient was prescribed dietary measures and then tamoxifen in May 2022.
The follow-up examination conducted three months after the start of the hormonal treatment showed a significant disorder of lipid metabolism with major hypertriglyceridemia at 56 g/L (Table 1). As a consequence, tamoxifen therapy was discontinued by her oncologist.
Upon admission, the patient was in a healthy state and did not experience any abdominal or chest discomfort. The electrocardiogram (EKG) showed no irregularities, and the patient had a normal body weight with a body mass index (BMI) of 24.4 kg/m^2^. However, the patient did have an enlarged waist circumference (91 cm). The physical examination revealed the absence of goiter or acanthosis nigricans, as well as the absence of cutaneous, tendinous, or tuberous xanthomas on the elbows. There were no eruptive xanthomas observed on the buttocks, abdomen, and limbs, and no signs of xanthelasma or gerontoxon were present. Additionally, there were no indications of hypercortisolism.
We immediately conducted an emergency assessment, put the patient on a 72-hour liquid diet, and then on an adapted diet. In addition, we initiated treatment with fenofibrate (200 mg/day) with a progressive improvement of the lipid profile (Table 1). Lipasemia, hepatic, renal, and thyroid function tests and blood sugar levels were without abnormalities. Lipoprotein electrophoresis showed an absence of chylomicrons, alpha lipoproteins at 5.9% (15.1-39.9), pre-beta lipoproteins at 92.4% (2-31.2), and a negative 24-hour decantation test at 4° (Figures 1, 2). It is, therefore, probably a type IV hypertriglyceridemia.
Aspect of our patient’s serum (purple arrow) in comparison with a normal serum
A negative 24-hour decantation test
After one month of treatment with fenofibrate 200 mg/day and well-conducted hygienic and dietary measures, as well as the discontinuation of tamoxifen, the lipid profile was checked again (Table 1).
The results of pharmacovigilance (Tables 2, 3) incriminate equally and with the same score of imputability I3B4 (French imputability method) for the two treatments: tamoxifen and triptorelin, which stands for an expected adverse drug reaction, and advised the stop of the two drugs in consultation with the prescribing doctor.
Discussion
We faced the case of a 43-year-old woman under tamoxifen and triptorelin as a treatment for her breast cancer. She presented major hypertriglyceridemia at 56 g/L with no complications, such as acute pancreatitis, as a side effect after three months of therapy.
Tamoxifen, a SERM, is widely used for hormone therapy of estrogen receptor (ER)-positive breast cancer. It has tissue-specific agonist and antagonist properties [2]. It can disturb the lipid balance by increasing VLDL (very low-density lipoprotein) synthesis and inhibiting lipoprotein lipase (LPL) and hepatic triglyceride lipase (HTGL) synthesis. This disturbance is more pronounced in the presence of predisposing factors [3]. Previous reports have shown that estrogen impairs the metabolism and clearance of triglyceride (TG)-rich lipoproteins due to post-heparin lipolytic activity suppression [4,5]. Post-heparin lipolytic activity consists of two activities: HTGL and extrahepatic LPL.
Triptorelin, a synthetic hormone, is an analog of natural GnRH (GnRHa). It can be used in early breast cancer in pre-menopausal women, endometriosis, and also in men with advanced prostate cancer. It has been associated with a small but significant increase in cholesterol and TG levels.
Similar to our patient’s case, individuals with familial hypertriglyceridemia or familial combined hyperlipidemia have been reported to have very high serum TG levels, which can lead to serious consequences [6,7]. Contrasting with a moderate rise in TGs in normolipidemic patients before the start of SERMs.
Tamoxifen is more likely to increase TG levels in patients with predisposing factors, such as an elevated pre-prescription TG levels, diabetes, obesity, chronic renal failure, non-alcoholic fatty liver disease, alcohol abuse, concomitant use of certain medications, familial hypertriglyceridemia, and combined hyperlipidemia [8].
Screening for dyslipidemia prior to tamoxifen administration is therefore strongly recommended, and predisposed patients should have regular lipid monitoring [9]. If abnormally high levels are found, tamoxifen should be discontinued in consultation with the prescribing doctor to avoid the risk of severe acute pancreatitis.
In the case we reported, we observed an acute increase of TG after tamoxifen use in a patient who already had hypertriglyceridemia. In Table 4, we report some cases of hypertriglyceridemia under tamoxifen found in the literature.
However, a small but significant increase in cholesterol and TG levels was observed in one study after GnRHa treatment in women with endometriosis [18]. All values were within normal limits (Table 5).
**Table 5: Lipid profile before and after treatment with triptorelin n = number of women with endometriosis treated with triptorelin*p < 0.05; p < 0.001; n = 43
We promptly put the patient on a 72-hour liquid diet and then on an adapted diet. After eliminating the contraindications of fibrates, we initiated treatment with fenofibrate (200 mg/day), resulting in a progressive improvement of the lipid balance. Fenofibrates increase lipolysis and the elimination of atherogenic TG-rich particles from plasma by activating the LPL and reducing the apoprotein CIII production.
In the literature, several management options for hypertriglyceridemia have been described, ranging from a liquid diet, a hypolipidemic, hypocaloric, and a high protein diet to drug treatment with fibrates. Gemfibrozil is the most hypotriglyceridemic, followed by bezafibrate, fenofibrate, and ciprofibrate [19].
The combination of fibrates and statins is sometimes necessary and reduces cardiovascular risk [20], and it is appropriate in severe mixed dyslipidemia. Only the combination of statins with gemfibrozil is not recommended because of the risk of rhabdomyolysis [21].
The hypotriglyceridemic effect of Omega 3 has been proven, but it only occurs at high doses (2-4 g/day) [22] and leads to a 30-50% decrease in TGs. The disadvantage of Omega 3 “drugs” is their relatively high cost. Consumption of fatty fish is an alternative, but at a dose of one box per day, digestive tolerance is sometimes poor.
Volanesorsen is a new molecule that can be indicated in major hypertriglyceridemia with a very high risk of acute pancreatitis [23]. Approach and compass studies have been shown to lower TGs and suppress the recurrence of acute pancreatitis [24,25].
Plasmapheresis is reserved for salvage situations in cases of refractory major hypertriglyceridemia associated with threatening hypertriglyceridemic acute pancreatitis [26].
Conclusions
We could confirm from these results that tamoxifen and triptorelin certainly modify lipid metabolism, hence the interest in evaluating the benefit-risk balance before their administration and constantly monitoring the lipid profile during the treatment, in order to avoid any complications, such as acute pancreatitis, which is the most characteristic complication of major hypertriglyceridemia, myocardial infarction, or stroke.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hypertriglyceridemic pancreatitis: epidemiology, pathophysiology and clinical management United European Gastroenterol J de Pretis N Amodio A Frulloni L 64965562018 https://doi.org/10.1177/205064061875500210.1177/2050640618755002 PMC 606877630083325 · doi ↗ · pubmed ↗
- 2Severe acute pancreatitis due to tamoxifen-induced hypertriglyceridemia Breast J Yoneyama K Nakagawa M 7887892520193104448110.1111/tbj.13279 · doi ↗ · pubmed ↗
- 3Effect of tamoxifen on serum lipid metabolism J Clin Endocrinol Metab Hozumi Y Kawano M Saito T Miyata M 16331635831998 https://doi.org/10.1210/jcem.83.5.4753.958966910.1210/jcem.83.5.4753 · doi ↗ · pubmed ↗
- 4Effect of estrogen on post-heparin lipolytic activity. Selective decline in hepatic triglyceride lipase J Clin Invest Applebaum DM Goldberg AP PykälistöOJ Brunzell JD Hazzard WR 601608591977 https://doi.org/10.1172/JCI 108677.84525210.1172/JCI 108677 PMC 372263 · doi ↗ · pubmed ↗
- 5Estrogen suppresses transcription of lipoprotein lipase gene. Existence of a unique estrogen response element on the lipoprotein lipase promoter J Biol Chem Homma H Kurachi H Nishio Y 11404114112752000 https://doi.org/10.1074/jbc.275.15.11404.1075395610.1074/jbc.275.15.11404 · doi ↗ · pubmed ↗
- 6Severe lipemia induced by tamoxifen Cancer Brun LD GagnéC Rousseau C Moorjani S Lupien PJ 21232126571986369791110.1002/1097-0142(19860601)57:11<2123::aid-cncr 2820571106>3.0.co;2-2 · doi ↗ · pubmed ↗
- 7Severe hypertriglyceridaemia and hypercholesterolaemia associated with tamoxifen use Clin Oncol (R Coll Radiol) Colls BM George PM 270271101998976438310.1016/s 0936-6555(98)80019-8 · doi ↗ · pubmed ↗
- 8Dyslipidemia in patients with nonalcoholic fatty liver disease Semin Liver Dis Chatrath H Vuppalanchi R Chalasani N 22293220122241888510.1055/s-0032-1306423 PMC 3654545 · doi ↗ · pubmed ↗