Characteristics and clinical outcomes of patients with kidney failure of unknown aetiology from ANZDATA registry
Lucy S. Wang, Venkat Vangaveti, Monica S. Y. Ng, Andrew J. Mallett, Mohamed E Elrggal, Mohamed E Elrggal, Mohamed E Elrggal, Mohamed E Elrggal

TL;DR
This study examines the characteristics and outcomes of patients with unknown causes of kidney failure in Australia and New Zealand, finding higher mortality risks compared to other kidney diseases.
Contribution
The study provides new insights into the clinical outcomes of patients with unknown etiology kidney failure in Australia and New Zealand.
Findings
Patients with unknown etiology kidney failure on dialysis had higher mortality rates compared to those with known causes.
Transplant recipients with unknown etiology kidney failure also showed increased mortality risk.
The likelihood of kidney transplantation was similar between patients with unknown and known causes of kidney failure.
Abstract
Kidney failure of unknown aetiology (uESKD) is also heavily location dependent varying between 27% in Egypt to 54% in Aguacalientes, Mexico. There is limited information about the characteristics of people with uESKD in Australia and New Zealand, as well as their clinical outcomes on kidney replacement therapy. Data on people commencing kidney replacement therapy 1989–2021 were received from the Australia and New Zealand Dialysis and Transplant (ANZDATA) registry. Primary exposure was cause of kidney failure–uESKD or non-uESKD (known-ESKD). Primary outcome was mortality. Secondary outcome was kidney transplantation. Dialysis and transplant cohorts were analysed separately. Cox Proportional Hazards Regression models were used to evaluate correlations between cause of kidney failure and mortality risk. Subgroup analyses were completed to compare mortality risk in people with uESKD to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
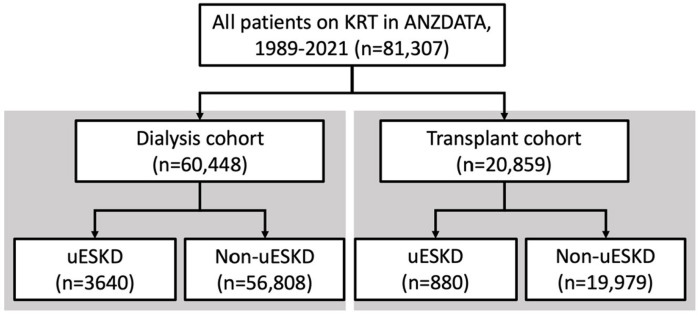 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Transplantation Outcomes and Treatments · Dialysis and Renal Disease Management · Organ Donation and Transplantation
Introduction
Kidney failure of unknown aetiology (uESKD) is also heavily location dependent varying between 27% in Egypt to 54% in Aguacalientes, Mexico [1–3]. uESKD is defined as kidney failure cases where there other causes of kidney diseases such as diabetes, hypertension, glomerular disease have been excluded as potential causes [1]. Inroads to identify causes of uESKD have been made with advances in genetic kidney diagnoses, however, 80% of initially uESKD remains without a causal diagnosis [4]. Therefore, there are no cause-specific treatment options, disease recurrence risks are unquantifiable and referral for transplant may be delayed due to uncertain recurrence risk. There is limited information about the characteristics of this group of patients; as well as their clinical outcomes after KRT initiation, including mortality risk and likelihood of kidney transplantation. Information about clinical outcomes of people with uESKD is essential to guide disease prognostication, patient counselling and KRT modality selection. This Australian and New Zealand Dialysis and Transplant (ANZDATA) registry analysis aimed to profile, at a population level, the characteristics, mortality risk and likelihood of kidney transplantation for people receiving KRT due to uESKD. We hypothesised that people with uESKD would have similar mortality risk and reduced likelihood of kidney transplantation compared to people with known-ESKD.
Materials and methods
Study population
This population-based cohort study included people over 18 years old who initiated kidney replacement therapy in Australia and New Zealand between 1 January 1989–31 December 2021. Demographic, comorbidity, kidney failure and outcome data were extracted from the Australia and New Zealand Dialysis and Transplant (ANZDATA) registry in de-identified format and accessed on 1^st^ April 2022. This access did not include access to information that could identify individual participants during or after data collection. The dialysis cohort included all adults who received dialysis as sole kidney replacement therapy modality (Fig 1). The transplant cohort included all adults who received a kidney transplant (Fig 1). Ethics approvals were received from ANZDATA executive (Request ID: 42579) and Metro North Human Research and Ethics Committee (Reference: LNR/2019/QRBW/58238). Written informed consent to the ANZDATA Registry was not required as a national quality assurance registry program. This study was reported per the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [5].
Flow chart demonstrating stratification of patient cohorts.
Variables
Primary exposure was kidney disease type classified as kidney failure of unknown aetiology (uESKD) or non-uESKD (known-ESKD) based on kidney failure cause codes in ANZDATA. Cases not caused by diabetic nephropathy, glomerular disease, hypertension or any other identifiable cause are classified as uESKD in ANZDATA. In ANZDATA, cause of kidney failure is denoted by treating kidney specialist based on clinical features and may not be biopsy- nor genetically- proven. Primary outcomes measures were mortality in the dialysis and transplant cohort; and kidney transplantation in all patients on KRT. Age and comorbidities were recorded at time of dialysis commencement for dialysis cohort and time of kidney transplant in transplant cohort. Age was classified by 10 year intervals. Comorbidities included diabetes, coronary artery disease and peripheral vascular disease which were denoted by treating kidney specialist. First KRT modality included haemodialysis, peritoneal dialysis and pre-emptive transplant. Dialysis and transplant era were classified in 10 year intervals.
Statistical analysis
Baseline variables were summarised using counts and percentages and assessed by χ2 tests of independence with Bonferroni correction for multiple testing (S1 and S2 Tables). Continuous variables were assessed with one way Analysis of Variance (ANOVA) with Bonferroni correction. Results were considered statistically significant if p<0.005.
Median follow-up time for dialysis and transplant cohorts was calculated using reverse Kaplan-Meier estimator. Univariable and multivariable Cox proportional hazards models were used to calculate the association between exposures and covariables with outcome variables (mortality, kidney transplantation). In the dialysis cohort analyses, covariates included gender, ethnicity, smoking status, body mass index (BMI) diabetes status, first dialysis modality and dialysis vintage. In the transplant cohort analyses; recipient gender, ethnicity, age, smoking status BMI, comorbidities, first KRT modality, human leukocyte antigen (HLA) mismatch and transplant era were included as covariates. In the kidney transplantation analyses, recipient gender, ethnicity, age, smoking status BMI, comorbidities, first KRT modality, HLA mismatch and transplant era were included as covariates. Hazard ratios (HRs) and 95% confident intervals (CIs) were calculated for each characteristic. Results were considered statistically significant if p<0.05.
In sensitivity analyses, Cox proportional hazard models were calculated for primary outcomes with non-ESKD were subclassified into diabetic nephropathy, glomerular disease, autosomal dominant polycystic kidney disease (ADPKD) and other kidney diseases (S1 Table). Diabetic nephropathy, glomerular disease and ADPKD were selected as each disease has known demographic features and outcomes. Hypertension was classified with other kidney diseases as it is unclear if hypertension is the cause of kidney failure or consequence an undiagnosed kidney disease [6]. Adjusted sub-distribution HRs (ASHRs) were generated using Fine and Gray’s proportional hazards models where mortality and kidney transplantation were competing risks [7]. Results were considered statistically significant if p<0.05.
Only complete cases were included in the analyses. All analyses were conducted in SPSS software (IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp).
Results
Participant demographics
Sixty thousand four hundred and forty-eight people on dialysis were included in the study with 3,640 people with uESKD, 24,513 people with diabetic nephropathy, 10,450 people with glomerular disease, 2,188 people with ADPKD and 19,657 with other kidney disease (Fig 1 and S2 Table). Twenty thousand eight hundred and fifty-nine people received kidney transplants– 880 recipients had uESKD, 2,458 recipients had diabetic nephropathy, 8,957 recipients had glomerular disease, 2,831 recipients had ADPKD and 5,733 recipients had other kidney disease (S3 Table). Median follow-up times for the dialysis and transplant cohorts were 10 years and 14 years respectively.
Mortality
In people on dialysis, 1 year, 3 year and 5 year mortality rates were 19.2%, 39.7% and 53.1% respectively (S2 Table). People on dialysis with uESKD had increased mortality risk compared to people with known-ESKD (AHR 1.10, 95% CI 1.06–1.16, Table 1) on multivariable analysis. On subgroup analysis, people with uESKD had similar mortality risk compared to other kidney diseases (S4 Table). Kidney transplant recipients had 1 year, 3 year and 5 year mortality rates of 0.6%, 2.4% and 4.7% respectively (S3 Table). Kidney transplant recipients with uESKD had increased mortality risk compared to those with known-ESKD (AHR 1.17, 95% CI 1.01–1.35, Table 2). On subgroup analysis, recipients with uESKD had similar mortality risk to those with other kidney diseases (S5 Table). Recipients with glomerular disease or ADPKD had reduced mortality risk while those with diabetic nephropathy had increased mortality risk.
Table 1: Unadjusted + adjusted hazard ratios + 95% CI for association between kidney disease and mortality in dialysis cohort.
Table 2: Unadjusted + adjusted hazard ratios and 95% CI for association between kidney disease status and mortality in transplant cohort.
Kidney transplantation
People with uESKD on KRT had similar likelihood of kidney transplantation compared to people with known-ESKD (Table 3). On subgroup analysis, uESKD had similar kidney transplantation compared to people with other kidney diseases (S6 Table). Death censored kidney transplantation was increased in people with uESKD compared to people with known-ESKD (AHR 1.24, 95% CI 1.18–1.29, S7 Table). Demographic features such as age between 40–59 years old, BMI between 25–29.9, peritoneal dialysis as first KRT modality and more recent KRT initiation were associated with increased likelihood of kidney transplant. People of female gender, age between 60–79 years old and current smoking status with comorbidities were associated with reduced likelihood of kidney transplant.
Table 3: Unadjusted + adjusted hazard ratios + 95% CI for association between kidney disease status and kidney transplantation.
Discussion
This study showed that people with uESKD have increased mortality risk but similar likelihood of kidney transplantation compared to people with known-ESKD. The prevalence of uESKD in people on dialysis and transplant was 6.0% and 4.2% respectively, which is lower than rates in United Kingdom (14.9%) [8], Europe (17.0%) [9], Brazil (24%) [10] and Mexico (54%) [3]. This difference in uESKD prevalence is likely multifactorial in the context of different occupational and environmental exposures; and access/utilisation of advanced diagnostic tests such as genetic testing. The high prevalence of uESKD in Mexico has been linked to intense work in strong heat, increased environmental degradation with exposure to heavy metals, widespread use of pesticides and reduced access to diagnostic testing to identify the cause of kidney failure [11].
People with uESKD on dialysis had increased mortality risk compared to people with known-ESKD. On subgroup analysis, uESKD had increased mortality risk compared to diabetic nephropathy, glomerular disease and ADPKD. Reasons for this finding is likely multifactorial–absence of cause-specific treatment for extra-kidney manifestations, older age at KRT initiation and socioeconomic factors. These results are different to those reported by Gutierrez-Peña et al. where people in Aguascalientes, Mexico, on KRT with uESKD had superior survival compared to those with known-ESKD on age-adjusted analyses [3]. In the aforementioned study, a significant proportion of known-ESKD participants had diabetic nephropathy which was associated with inferior mortality outcomes compared to people with other causes of kidney failure [3].
Kidney transplant recipients with uESKD have increased mortality risk compared to those known-ESKD. On subgroup analysis, uESKD performed similarly compared to other kidney diseases. Glomerular disease and ADPKD were associated with superior post-transplant mortality outcomes compared to those with other kidney diseases–likely contributing to the outcomes seen in the binary (uESKD vs. known-ESKD) exposure analyses. A previous ANZDATA analysis identified that transplant recipients with uESKD had similar mortality risk compared to recipients with commonly-recurring glomerular diseases [12]. Commonly-recurring glomerular diseases carry higher mortality risks associated with increased risk of graft failure and higher immunosuppression burden [12]. Graft failure data was not accessible to test this hypothesis. The finding that recipients with uESKD have similar mortality risk compared to other kidney diseases was also identified in an USRDS study of younger transplant recipients [13].
People on KRT with uESKD had similar likelihood of kidney transplantation compared to people with known-ESKD. On death-censored kidney transplantation, people with uESKD had higher kidney transplantation rates compared to people with known-ESKD suggesting that the increased mortality risk of people with uESKD may be contributing to the results seen in the headline analyses. All people on KRT were included in the kidney transplantation analyses, however an unknown proportion would have been deemed unsuitable for transplantation. As such, it was not possible to assess kidney transplantation solely in those who were suitable for transplantation. Subset analysis of patients suitable for transplantation will be possible in the future with the recent addition of “suitability for kidney transplant” in ANZDATA data collection.
In this study, uESKD performed similarly to other causes of kidney failure in subgroup analyses for demographics, mortality and kidney transplantation, suggesting that uESKD may overlap with conditions in the “other kidney disease” category. Chronic kidney disease of uncertain aetiology (CKDu) observed in low and middle income countries mainly occurs in agricultural communities affecting young males [14]. In our analyses, uESKD was associated with increased age which may be due to reduced appetite for higher risk diagnostic procedures such as kidney biopsies in older people with atrophic kidneys [15]. This disparity further signals that uESKD as recorded in ANZDATA is different to CKDu reported elsewhere and that uESKD is highly jurisdiction-dependent. Further study is required to elucidate the potential genetic, occupational, and environmental factors causing uESKD in Australia and New Zealand.
Limitations included the use of retrospective observational data, thereby confounded by measurement bias, and unmeasured factors not collected by ANZDATA. Primary kidney disease classifications in ANZDATA are based on clinician classification as the dominant cause, and are not always biopsy- or genetically-proven. Furthermore, advances in diagnostic approaches and disparities in access to such diagnostics can lead to inconsistencies in uESKD definition across regions and over time.
Conclusions
People with uESKD on KRT had increased mortality risks compared to known-ESKD. uESKD has similar likelihood of kidney transplantation compared to known-ESKD. On subgroup analysis, the uESKD group had similar demographic features compared to other kidney diseases and performed similarly on outcome measures, suggesting that uESKD may include people with “other kidney diseases”. Further studies are required to confirm this hypothesis and correlated uESKD recorded in ANZDATA to CKDu in other jurisdictions.
Supporting information
S1 TableBreakdown of kidney failure causes in other kidney disease group.(DOCX)
S2 TableCharacteristics and medical conditions of the dialysis cohort.(DOCX)
S3 TableCharacteristics and medical conditions of the transplant cohort.(DOCX)
S4 TableSubgroup analysis evaluating association between kidney disease status and mortality in dialysis cohort.(DOCX)
S5 TableSubgroup analysis evaluating association between kidney disease status and mortality in transplant cohort.(DOCX)
S6 TableSubgroup analysis evaluating association between kidney disease status and kidney transplantation in KRT cohort.(DOCX)
S7 TableDeath-censored kidney transplantation competing risk analysis.(DOCX)
S8 TableModified STROBE statement.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weaver VM, Fadrowski JJ, Jaar BG. Global dimensions of chronic kidney disease of unknown etiology (CK Du): a modern era environmental and/or occupational nephropathy? BMC Nephrology. 2015 2015/08/19;16(1):145. doi: 10.1186/s 12882-015-0105-6 26282933 PMC 4539684 · doi ↗ · pubmed ↗
- 2Gutierrez-Peña M, Zuñiga-Macias L, Marin-Garcia R, Ovalle-Robles I, García-Díaz AL, Macías-Guzmán MJ, et al. High prevalence of end-stage renal disease of unknown origin in Aguascalientes Mexico: role of the registry of chronic kidney disease and renal biopsy in its approach and future directions. Clinical Kidney Journal. 2021;14(4):1197–206. doi: 10.1093/ckj/sfaa 229 34094519 PMC 8173605 · doi ↗ · pubmed ↗
- 3Groopman EE, Marasa M, Cameron-Christie S, Petrovski S, Aggarwal VS, Milo-Rasouly H, et al. Diagnostic Utility of Exome Sequencing for Kidney Disease. New England Journal of Medicine. 2018 2019/01/10;380(2):142–51. doi: 10.1056/NEJ Moa 1806891 30586318 PMC 6510541 · doi ↗ · pubmed ↗
- 4von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008 Apr;61(4):344–9. doi: 10.1016/j.jclinepi.2007.11.008 18313558 · doi ↗ · pubmed ↗
- 5Ruzicka M, Hiremath S. Cause, Consequence or confounding? The kidney in hypertension. Journal of Human Hypertension. 2019 2019/09/01;33(9):639–40. doi: 10.1038/s 41371-019-0199-6 30992515 · doi ↗ · pubmed ↗
- 6Fine JP, Gray RJ. A Proportional Hazards Model for the Subdistribution of a Competing Risk. Journal of the American Statistical Association. 1999 1999/06/01;94(446):496–509.
- 7Böhlke M. Kidney failure of unknown cause: a call to admit our uncertainty. Brazilian Journal of Nephrology. 2023;00(00):00–00.10.1590/2175-8239-JBN-2022-0134 en PMC 1069715637229776 · doi ↗ · pubmed ↗
- 8Kierans C, Padilla-Altamira C. Anthropological perspectives on CK Dnt in Mexico: time for a paradigm shift on the social determinants of health. Frontiers in Nephrology. 2023 2023-June-12;3. doi: 10.3389/fneph.2023.1155687 37675371 PMC 10479662 · doi ↗ · pubmed ↗