Development and validation of mortality prediction models for heart transplantation using nutrition-related indicators: a single-center study from China
Shirui Qian, Bingxin Cao, Ping Li, Nianguo Dong

TL;DR
This study developed a model to predict mortality after heart transplantation using nutrition-related indicators to help identify high-risk patients.
Contribution
A novel mortality prediction model for heart transplant patients using nutrition-related indicators was developed and validated in a Chinese cohort.
Findings
The model included age, nutritional risk index, serum creatine, and triglyceride as key predictors.
The model showed improved discrimination and reclassification compared to simpler models using only age or nutritional risk index.
The model's AUC was 0.76 in the derivation cohort and 0.71 in the validation cohort.
Abstract
We sought to develop and validate a mortality prediction model for heart transplantation (HT) using nutrition-related indicators, which clinicians could use to identify patients at high risk of death after HT. The model was developed for and validated in adult participants in China who received HT between 1 January 2015 and 31 December 2020. 428 subjects were enrolled in the study and randomly divided into derivation and validation cohorts at a ratio of 7:3. The likelihood-ratio test based on Akaike information was used to select indicators and develop the prediction model. The performance of models was assessed and validated by area under the curve (AUC), C-index, calibration curves, net reclassification index, and integrated discrimination improvement. The mean (SD) age was 48.67 (12.33) years and mean (SD) nutritional risk index (NRI) was 100.47 (11.89) in the derivation cohort.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
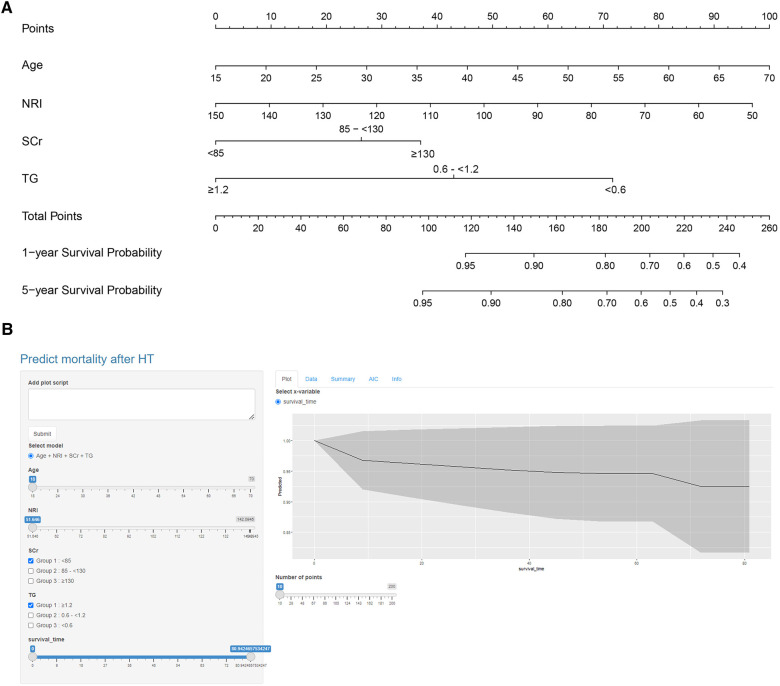 Figure 1
Figure 1| Variables | Derivation cohort ( | Validation cohort ( | |
|---|---|---|---|
| Recipients | |||
| Gender (male) | 240 (80.3%) | 102 (79.1%) | 0.777 |
| Age (years) | 48.67 ± 12.33 | 46.12 ± 11.99 | 0.076 |
| BMI (kg/m2) | 22.88 ± 4.04 | 23.31 ± 3.75 | 0.281 |
| Diagnosis | 0.096 | ||
| Ischemia cardiomyopathy | 181 (60.5%) | 91 (70.5%) | |
| Non-ischemia cardiomyopathy | 69 (23.1%) | 17 (13.2%) | |
| Congenital heart disease | 43 (14.4%) | 21 (16.3%) | |
| Other heart disease | 6 (2.0%) | 0 (0%) | |
| ABO blood type | 0.086 | ||
| A | 107 (35.8%) | 38 (29.5%) | |
| B | 72 (24.1%) | 43 (33.3%) | |
| O | 95 (31.8%) | 43 (33.3%) | |
| AB | 25 (8.4%) | 5 (3.9%) | |
| Hypertension | 51 (17.1%) | 18 (14.0%) | 0.464 |
| Diabetes mellitus | 49 (16.4%) | 15 (11.6%) | 0.184 |
| Hyperlipemia | 12 (4.0%) | 7 (5.4%) | 0.550 |
| Chronic liver disease | 23 (7.7%) | 9 (7.0%) | 0.796 |
| Chronic kidney disease | 20 (6.7%) | 6 (4.7%) | 0.418 |
| History of smoking | 119 (39.8%) | 58 (45.0%) | 0.320 |
| History of alcoholism | 69 (23.1%) | 35 (27.1%) | 0.369 |
| Cardiac surgery history (yes) | 79 (26.4%) | 32 (24.8%) | 0.726 |
| IABP | 5 (1.7%) | 2 (1.6%) | 0.927 |
| ECMO | 5 (1.7%) | 0 (0%) | 0.140 |
| Donors Characteristics | |||
| Donor gender (male) | 267 (89.3%) | 110 (85.6%) | 0.251 |
| Donor age (years) | 35.51 ± 11.64 | 35.04 ± 12.51 | 0.710 |
| Donor BMI (kg/m2) | 22.54 ± 3.14 | 22.71 ± 3.93 | 0.634 |
| Donor/recipient BMI | 1.01 ± 0.20 | 0.99 ± 0.22 | 0.441 |
| Donor/recipient age | 0.79 ± 0.37 | 0.81 ± 0.41 | 0.586 |
| Donor/recipient gender | 0.116 | ||
| Male/male | 221 (73.9%) | 87 (67.4%) | |
| Male/female | 46 (15.4%) | 17 (13.2%) | |
| Female/male | 19 (6.4%) | 15 (11.6%) | |
| Female/female | 13 (4.3%) | 10 (7.8%) | |
| Recipient/donor blood-type | 0.423 | ||
| Identical | 243 (81.3%) | 109 (84.5%) | |
| Different | 56 (18.7%) | 20 (15.5%) | |
| Cause of death | 0.173 | ||
| Brain Injury | 186 (64.8%) | 66 (53.7%) | |
| Cerebral hemorrhage | 85 (29.6%) | 50 (40.7%) | |
| Brain Tumor | 10 (3.5%) | 4 (3.3%) | |
| Others | 6 (2.1%) | 3 (2.4%) | |
| Cold ischemia time (min) | 333.83 ± 106.69 | 336.34 ± 114.71 | 0.827 |
| Aortic crossclamp time (min) | 32.05 ± 12.43 | 33.44 ± 19.90 | 0.380 |
| Cardiopulmonary bypass time (min) | 113.26 ± 37.28 | 123.67 ± 94.30 | 0.103 |
| Preoperative Blood Index | |||
| Hb (g/L) | 134.60 ± 22.16 | 134.02 ± 21.27 | 0.804 |
| RBC (1012/L) | 4.46 ± 0.72 | 4.47 ± 0.78 | 0.911 |
| HCT (%) | 40.67 ± 6.22 | 40.47 ± 6.15 | 0.763 |
| Bilirubin (µmol/L) | 28.27 ± 21.02 | 28.42 ± 27.63 | 0.947 |
| ALT (U/L) | 72.62 ± 315.98 | 46.75 ± 85.36 | 0.361 |
| AST (U/L) | 62.92 ± 274.84 | 38.86 ± 80.07 | 0.330 |
| SCr (µmol/L) | 98.82 ± 43.54 | 99.24 ± 65.57 | 0.937 |
| BUN (mmol/L) | 8.31 ± 3.97 | 7.66 ± 3.07 | 0.097 |
| UA (µmol/L) | 503.16 ± 176.06 | 474.07 ± 153.87 | 0.104 |
| TC (mmol/L) | 3.63 ± 1.00 | 3.62 ± 0.92 | 0.910 |
| BNP | 5,365.37 ± 6,173.90 | 4,861.12 ± 5,928.09 | 0.472 |
| LDL-C (mmol/L) | 2.23 ± 0.79 | 2.20 ± 0.75 | 0.714 |
| TG (mmol/L) | 1.17 ± 0.66 | 1.23 ± 0.69 | 0.344 |
| NRI (pg/ml) | 100.47 ± 11.89 | 102.75 ± 10.42 | 0.060 |
| Models, odds ratio (95% CI) | |||
|---|---|---|---|
| 1. Age, NRI, TG, SCr | 2. Age, NRI | 3. NRI | |
| Predictors | |||
| Age, per year increase | 1.04 (1.02–1.07) | 1.04 (1.02–1.07) | |
| NRI, per unit increase | 0.98 (0.96–0.99) | 0.97 (0.96–0.99) | 0.98 (0.96–0.99) |
| TG, mmol/L | |||
| ≥1.2 | 1 [Reference] | ||
| 0.6≤1.2 | 2.62 (1.26–5.44) | ||
| <0.6 | 4.99 (2.01–12.39) | ||
| SCr, µmol/L | |||
| <85 | 1 [Reference] | ||
| 85≤130 | 1.80 (1.02–3.18) | ||
| ≥130 | 2.29 (1.10–4.78) | ||
| Model performance measures | |||
| Akaike information criterion | 683.4 | 696.8 | 710.6 |
| C statistic | 0.72 (0.67–0.78) | 0.68 (0.62–0.74) | 0.59 (0.53–0.66) |
| Integrated discrimination improvement, % | 6.9 (1.8–15.1) | 14.7 (7.4–26.2) | |
| 0.005 | <0.001 | ||
| Net reclassification improvement, % | |||
| Continuous | 36.9 (17.0–51.6) | 46.6 (30.5–64.3) | |
| 0.007 | <0.001 | ||
| Categorical | 21.2 (−2.8–38.5) | 41.8 (9.9–58.8) | |
| 0.039 | <0.001 | ||
| Models, odds ratio (95% CI) | |||
|---|---|---|---|
| 1. Age, NRI, Scr, TG | 2. Age, NRI | 3. NRI | |
| Akaike information criterion | 252 | 253 | 258.1 |
| C statistic | 0.71 (0.62–0.81) | 0.67 (0.57–0.77) | 0.63 (0.53–0.73) |
| Integrated discrimination improvement, % | 4.3 (−0.4–15.3) | 13.2 (3.6–31.7) | |
| 0.085 | 0.003 | ||
| Net reclassification improvement, % | |||
| Continuous | 25.5 (−8.2–48.8) | 40.0 (10.3–65.0) | |
| 0.142 | 0.017 | ||
| Categorical | 20.6 (−9.1–56.7) | 60.7 (9.0–100.5) | |
| 0.22 | 0.008 | ||
- —National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Heart Failure Treatment and Management · Renal Transplantation Outcomes and Treatments
Introduction
1
Heart failure (HF) is a global pandemic. There are about 64.3 million HF patients worldwide and approximately 4.5 million in China (1, 2). Advanced end-stage HF has an unfavorable prognosis, and the ultimate therapeutic option is heart transplantation (HT) (3, 4). In 2021, about 738 HT were performed in China according to data from the China Heart Transplant Registration Network (5). In 2023, the number increased and our center performed 121 HT. The total number of HT reached 1,000 in April 2023. Due to the mismatch between organ supply and demand, there is a significantly higher waitlist than HT surgery rates (6, 7). This leads to longer waiting periods before HT, which may cause disease progression and poor nutritional status (2, 8, 9).
Malnutrition is common in HF, affecting up to 70% of HF patients (10). As HF progresses, it may appear as “cardiac cachexia” in extreme states. In this state, patients would develop protein-calorie malnutrition along with muscle wasting and peripheral edema (11). It leads to a poor life quality and an increase in mortality. However, less severe malnutrition is hard to recognize and the same as its effect on prognosis of HT. An easy and accessible mortality prediction model using nutrition-related indicators may reflect the effect of mild malnutrition on the prognosis of HT and predict mortality risk of HT patients. To our knowledge, there is no such clinical model yet.
Nutritional risk index (NRI) is an easily calculated index incorporating albumin and body size (12). For the past few years, NRI has proven its prognostic utility in HF patients, but there is little data, especially Chinese data, in HT (13–15). In this study, we verified the prognostic value of NRI in HT. Moreover, we used HT patients' data in China to derivate and validate risk prediction models for post-HT surgery death. We aimed at developing and validating a mortality prediction model for HT. This risk stratification approach can be used to identify patients at high risk of death after HT.
Method
2
Ethical statement
2.1
After donor brain death, all donor hearts were donated to the Red Cross Society in the terms of China's laws. The donor hearts transplanted to recipients were allocated by the China Organ Transplant Response System. The study conformed to the “Declaration of Istanbul on Organ Trafficking and Transplant Tourism” and the national program for deceased organ donation in China (national protocol for China category I) (16). This study was approved by the Ethics Committee of Wuhan Union Hospital. And the requirement of written informed consent was waived by the ethics committee since the study was retrospective. In addition, all clinical data was anonymized and de-identified.
Study population
2.2
We used the HT database from our center in which participants were followed up through telephone or outpatient visit. For those who could not attend the telephone interview for physical or cognitive reasons, we performed an interview with their relatives to reduce attrition bias. All participants received orthotopic heart transplantation between 1 January 2015 and 31 December 2020. We excluded people who underwent multiple organ transplantation or re-transplantation and those with missing data. Then we divided patients into the derivation and validation cohorts using a simple randomization method. First, a random number was generated for each participant with random seed 20,191,102. Then, the random numbers were sorted in order from smallest to largest. The first 70% of participants were divided into the derivation cohort; the remaining were placed into the validation cohort (Supplementary Figure S1).
Study outcomes
2.3
The primary outcome of the study was defined as all-cause postoperative death. Mortality data were obtained from the China Heart Transplant Registration Network until 26 May 2021, where all deaths of HT are required to be registered by law.
Candidate predictors
2.4
We identified nutrition-associated candidate predictors available prior to HT operation through published systematic reviews and univariate Cox proportional hazards regression. All the predictors were retrieved from electronic medical records. Laboratory examinations were conducted within 7 days prior to HT operation. NRI was calculated using the following formula: NRI = [1.519 × serum albumin (in g/dl)] + [41.7 × weight (in kg)/ideal body weight (in kg)] (13). We used the Lorentz formula to calculate ideal body weight (IBW) on the basis of patients' height and gender: IBW = height (in cm)−100−[height (in cm) – 150]/4 for men and IBW = height (in cm)−100−[height (in cm) – 150]/2.5 for women (17).
Model derivation
2.5
All nutrition-associated candidate predictors with a significance level of 0.1 in univariate Cox proportional hazards regression were included as potential variables in multivariate Cox proportional hazards regression models in the derivation cohort. To create prediction models that could be more efficiently used, we performed stepwise backward variable selection based on Akaike Information Criterion (AIC) in 1,000 bootstrapped samples with a significance level of 0.05 (18, 19). The bootstrapped samples were the same size as the derivation sample. Then, we fit a reduced model and compared the full prediction model with NRI and the reduced model.
Model performance
2.6
The overall goodness-of-fit of the models was compared between models using an AIC indicator. Model discrimination was evaluated through C statistic and integrated discrimination improvement (IDI). As for calibration, calibration curves were drawn graphically. We calculated categorical and continuous net reclassification index to compare the reclassification ability of clinical prediction models (20). For the categorical net reclassification index, the risk threshold was defined as less than 20%, 20% to less than 40%, and 40% or higher.
The area under the ROC curve (AUC) was calculated to validate the discrimination of NRI in overall mortality after HT surgery. Kaplan–Meier (KM) survival analysis was generated to compare survival rate in different groups and differences were examined using log-rank. Statistical significance was considered as a P-value of <0.05 (two-sided) for all contrasts. Statistical analysis was conducted using SPSS 27.0.1 and R 4.3.0.
Results
3
Characteristics of cohorts
3.1
A total of 428 HT patients were included in the study cohort (299 participants in the derivation cohort and 129 in the validation cohort). In the derivation cohort, 240 (80.3%) participants were male with mean (SD) age 48.67 (12.33) years. Most participants (181, 60.5%) were diagnosed with ischemic cardiomyopathy. About 79 (26.4%) underwent cardiac surgery beforehand. The mean (SD) NRI was 100.47 (11.89). By the end of follow up, a total of 66 (22.1%) participants died after HT (Table 1 and Supplementary Table S1).
Demographics in the validation cohort were similar to the derivation cohort. And 28 (21.7%) participants died by the end of follow up. Donors' characteristics were also available in the study and there were no statistical differences between the derivation cohort and validation cohort.
Prediction performance of nutritional risk Index
3.2
In the derivation cohort, the AUC of NRI for predicting overall postoperative death was 0.613, with a cut-off level of 103.79 (95% CI, 0.542–0.684, P = 0.005). Patients in the low NRI group had lower body mass index, hemoglobin, red blood cells, hematocrit, total cholesterol, low density lipoprotein, and lower triglyceride (TG) and higher levels of blood urea nitrogen and brain natriuretic peptide. These patients presented lower prevalence of hypertension and diabetes mellitus and higher prevalence of chronic liver disease (Supplementary Table S2). The result of the K–M survival curve showed that the high NRI group had better overall survival (OS) compared to the low NRI group (P < 0.01) (Supplementary Figure S2). The C statistic was 0.59 (95% CI, 0.53–0.66) in the derivation cohort and 0.63 (95% CI, 0.53–0.73) in the validation cohort (Tables 2, 3).
Nutrition-associated prediction model derivation
3.3
In the bootstrapped samples of the derivation cohort, multivariable Cox proportional hazards regression analysis showed that older age, lower NRI values, and higher serum creatinine (SCr) and TG values were relevant to a high risk of death after HT. After this, the four-variable model (model-1) was finally developed. The odds ratio of multivariable Cox proportional hazards regression for variables in the model can be seen in Table 2.
Prediction model performance in the derivation and validation cohort
3.4
The AUC of the four-variable model (model-1) for predicting overall postoperative death was 0.755 in the derivation cohort. (Supplementary Figure S3A) Compared with other models, model-1 had the highest C statistic and lowest AIC both in the derivation and validation cohorts. The C statistic of model-1 was 0.72 (95% CI, 0.67–0.78) in the derivation cohort and 0.71 (95% CI, 0.62–0.81) in the validation cohort. Discrimination based on IDI significantly improved in the four-variable model compared with model-2 without SCr and TG (6.9%; 95% CI, 1.8%–15.1%; P < 0.01) and with model-3, which only included variable NRI (14.7%; 95% CI, 7.4%–26.2%; P < 0.001) in the derivation cohort (Tables 2, 3). A similar IDI improvement was also observed in the validation cohort. Both continuous and categorical net reclassification index improved in the four-variable model compared with other models in the derivation and validation cohorts.
As the calibration curves show, the four-variable model was better calibrated than other models in the derivation cohort and was the same in the validation cohort (Supplementary Figure S4). Based on the predicted risk of 5-year post-HT death calculated through the four-variable model, 155 patients (51.8%) in the derivation cohort had less than 20%; 102 (34.1%) 20% to less than 40%; and 42 (14.0%) 40% or more risk of death (Supplementary Table S3). The K–M survival curve analysis demonstrated that participants in the group with a predicted risk of 5-year post-HT death less than 20% had better OS compared to that of 20% to less than 40% risk of postoperative death and 40% or more risk of death (P < 0.0001) (Supplementary Figure S3B). Then we presented the four-variable model as a nomogram (Figure 1A) and made it freely available online to help clinicians to calculate the risk of post-HT death (Figure 1B) (https://docqianofwuhanunionhospital.shinyapps.io/MortalityPredictionAfterHeartTransplantation/).
Nomogram of the four-variable model. (A) Nomogram was constructed based on the derivation cohort. The range of indicators in the nomogram was shown as follows: Age, 18–70 years old; NRI, 51.65–142.09; SCr, 36.1–531.5 µmol/L; TG, 0.25–4.79 mmol/L. (B) The dynamic nomogram is available online (https://docqianofwuhanunionhospital.shinyapps.io/MortalityPredictionAfterHeartTransplantation/).
Discussion
4
In this study, we first investigated the prediction efficiency of NRI on post-HT surgery death. The results showed that patients with higher NRI had lower OS post operation. Patients in the low NRI group had a higher prevalence of liver disease. As reported, malnutrition occurs in more than 50% of patients with chronic liver disease. Both adipose tissue and muscle tissue can be depleted; female patients more frequently develop a depletion in fat deposits while males more rapidly lose muscle tissue (21). Patients with low NRI had lower hemoglobin, fewer red blood cells, and higher blood urea nitrogen. The reason for that may be these patients had more severe primary disease, which would affect the nutritional status of the body.
Then, we developed a four-variable mortality prediction model using nutrition-related indicators. It can be used to estimate mortality risk 1-year and 5-year post-HT operation and is available online. This model included variables of age, NRI, SCr, and TG, which can be obtained readily in clinical practice, and showed the best performance for predicting postoperative death of HF patients in derivation and validation cohorts than reduced models based on age and NRI, or based on NRI alone. In clinical practice, it can be used easily to estimate individualized risk of death post HT operation. Death risk stratification according to this model could help guide prognostic assessment and medical care after admission.
As the results of the model discrimination and calibration showed, there was no deterioration in the validation cohort, which means the four-variable nutrition-associated mortality prediction model was not overfit. Generally speaking, a C statistic higher than 0.70 is a criterion to determine whether models are useful in clinical use (22). In this four-variable model, the C statistic was 0.72 (95% CI, 0.67–0.78) in the derivation cohort and 0.71 (95% CI, 0.62–0.81) in the validation cohort. Since both C statistics were higher than 0.70, this model was considered as having significance in clinical decision making. Compared to the reduced model and variable NRI alone, net reclassification improvement of the full model demonstrated that the four-variable nutrition-associated mortality prediction model could improve accuracy of predicting post-HT death and risk stratification of death.
Singh et al. reported a risk prediction model to predict in-hospital mortality post HT operation using six recipient variables in 2012 (23). The model was derived in HT participants in the United States and validated internally through bootstrapping method and externally in patients receiving HT from July 2009 to October 2010. The C statistics were 0.72 in the derivation cohort, 0.73 in the internal validation cohort, and 0.68 in the external validation cohort. In addition, Weiss et al. developed a risk score using 12 recipient variables in US recipients from 1997 to 2008. This score could be used to predict 1-year mortality post HT (C statistic, 0.65) (24). Both of these studies focused on early mortality after HT. The mortality risk prediction model using nutrition-related indicators in this study differs importantly by its focus on post-operation 5-year mortality and using a more recent China cohort (2015–2020). There is no other prediction model using Chinese HT data to our knowledge. Besides, the model in this study focused on the malnutrition effect on prognosis of patients who received HT. Hence, all the candidates and the ultimate variables of this model were nutrition-associated indexes.
The mortality prediction model developed in this study may have implications for clinical care and decision making. Obtaining individualized risk of death after HT may help inform decisions about pursuing a course of treatment. Clinicians could use this model to identify patients at high risk of postoperative death before HT surgery, which would help with targeted preventative therapy to reduce the mortality risk. Also, being able to identify patients at high risk of postoperative mortality before HT may allow for better planning of resource allocation. In clinical practice, it is quite challenging for clinicians to determine the therapy of HT, especially in complex HF patients, as there are alternative therapies like implantable ventricular assist devices (25, 26). The mortality risk prediction model may be useful in assessing whether patients could benefit from a transplant.
Limitations
5
This study has some limitations. First, several nutrition-associated variables like muscle mass, weight loss within 1 month, triceps' skinfold thickness, and so on were not included in this study since this was a retrospective study and such variables were not attainable in the HT database. Second, participants with retransplant were excluded from this study, so the prediction model may not be appropriate for those patients. Due to the complex condition and extra risk of retransplant patients, a more specific study should be performed for those patients. Finally, the model was developed using HT data from a single center in China and we did not perform external validation for this model, which may influence the efficacy of the model. This work should be verified in the future.
Conclusion
6
A multivariable prediction model using variables of age, NRI, SCr, and TG was developed in this study. It was able to predict mortality after HT operation and is available online for use. The utility of this prediction model in clinical practice requires further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392(10159):1789–858. 10.1016/S 0140-6736(18)32279-730496104 PMC 6227754 · doi ↗ · pubmed ↗
- 2Ma LY Chen WW Gao RL Liu LS Zhu ML Wang YJ China Cardiovascular diseases report 2018: an updated summary. J Geriatr Cardiol. (2020) 17(1):1–8. 10.11909/j.issn.1671-5411.2020.01.00132133031 PMC 7008101 · doi ↗ · pubmed ↗
- 3Yusen RD Edwards LB Dipchand AI Goldfarb SB Kucheryavaya AY Levvey BJ The registry of the international society for heart and lung transplantation: thirty-third adult lung and heart-lung transplant report-2016; focus theme: primary diagnostic indications for transplant. J Heart Lung Transplant. (2016) 35(10):1170–84. 10.1016/j.healun.2016.09.00127772669 · doi ↗ · pubmed ↗
- 4Mc Donagh TA Metra M Adamo M Gardner RS Baumbach ABöhm M 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42(36):3599–726. 10.1093/eurheartj/ehab 36834447992 · doi ↗ · pubmed ↗
- 5Wang Z Ma L Liu M Fan J Hu S, Writing Committee of the Report on Cardiovascular Health and Diseases in China. Summary of the 2022 report on cardiovascular health and diseases in China. Chin Med J. (2023) 136(24):2899–908. 10.1097/CM 9.000000000000292738018129 PMC 10752444 · doi ↗ · pubmed ↗
- 6Manara A Shemie SD Large S Healey A Baker A Badiwala M Maintaining the permanence principle for death during in situ normothermic regional perfusion for donation after circulatory death organ recovery: a United Kingdom and Canadian proposal. Am J Transplant. (2020) 20(8):2017–25. 10.1111/ajt.1577531922653 PMC 7540256 · doi ↗ · pubmed ↗
- 7Crespo-Leiro MG Costanzo MR Gustafsson F Khush KK Macdonald PS Potena L Heart transplantation: focus on donor recovery strategies, left ventricular assist devices, and novel therapies. Eur Heart J. (2022) 43(23):2237–46. 10.1093/eurheartj/ehac 20435441654 · doi ↗ · pubmed ↗
- 8Singhal AK Abrams JD Mohara J Hasz RD Nathan HM Fisher CA Potential suitability for transplantation of hearts from human non-heart-beating donors: data review from the gift of life donor program. J Heart Lung Transplant. (2005) 24(10):1657–64. 10.1016/j.healun.2004.11.04316210144 · doi ↗ · pubmed ↗