Unveiling a Unique Case of Scimitar Syndrome: Clinical Significance and Multidisciplinary Management Challenges in Pakistan
Gulalay Shamal, Anam Israr Khan, Ahsan Ali, Neha James, Moula Ghulam

TL;DR
This case report describes a rare instance of Scimitar syndrome in Pakistan, highlighting its diagnosis, management challenges, and the importance of personalized treatment strategies.
Contribution
The paper presents a unique case of Scimitar syndrome in Pakistan with a focus on conservative management and multidisciplinary care.
Findings
A 26-year-old female was diagnosed with Scimitar syndrome through radiological assessments.
Conservative management was chosen over surgery, emphasizing patient preferences and clinical course.
Radiological techniques like CTPA and MRI are crucial for diagnosis and monitoring.
Abstract
Scimitar syndrome, a rare congenital cardiac anomaly, involves abnormal pulmonary vein drainage into systemic veins, leading to distinct imaging features resembling a curved-blade sword. This case report presents a unique instance of scimitar syndrome in Pakistan, emphasizing its clinical importance and the challenges of management. A 26-year-old female with a history of recurrent pulmonary infections and respiratory symptoms since childhood was diagnosed with scimitar syndrome. Radiological assessments, including chest X-rays, computed tomography pulmonary angiograms (CTPA), and transthoracic echocardiography, confirmed the presence of a curved vessel originating from the right hemidiaphragm and connecting with the inferior vena cava (IVC). The patient and her medical team opted for conservative management, involving multidisciplinary care, tailored treatment for infections, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
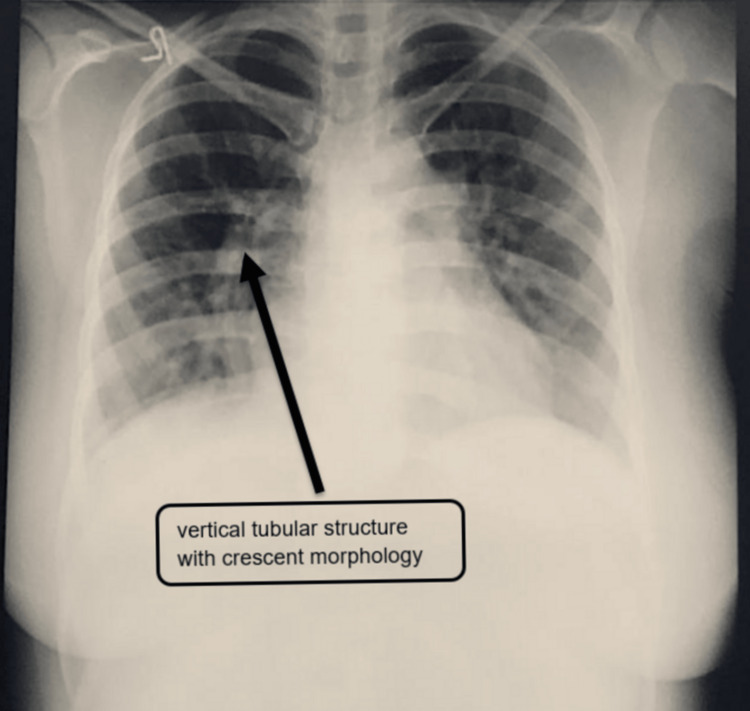 Figure 1
Figure 1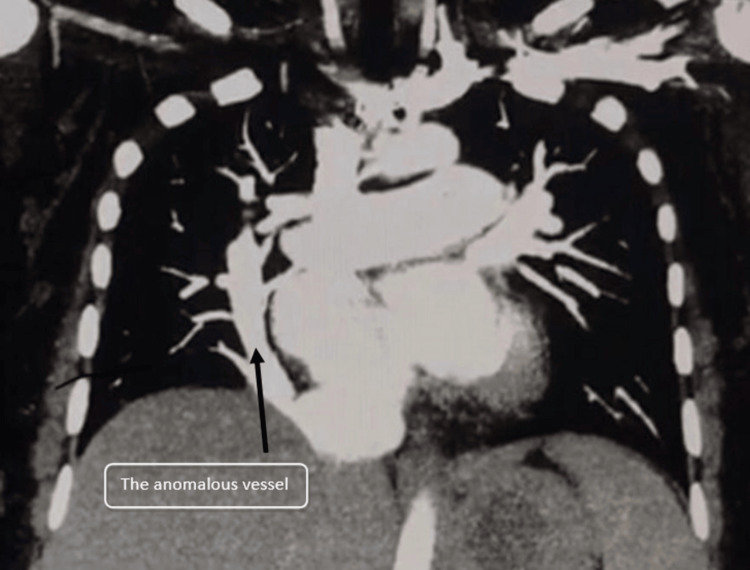 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Tracheal and airway disorders · Congenital Heart Disease Studies
Introduction
Scimitar syndrome, also referred to as congenital venolobar syndrome, Halasz syndrome, mirror-image lung syndrome, hypogenetic lung syndrome, and vena cava bronchovascular syndrome, is an uncommon congenital cardiac condition. Its unique anatomical feature, resembling a curved-blade sword known as a "scimitar," gives it its name [1,2]. Although it affects only a small fraction of live births, approximately 1-3 per 100,000, it presents as a partial anomalous pulmonary venous return, causing a left-to-right shunt [3]. However, due to the potential lack of symptoms, the true incidence might be higher. Although the precise mechanism causing scimitar syndrome is not yet known, it is likely caused by an embryological mistake in the basic development of the lung bud in early embryogenesis [4].
Symptoms of scimitar syndrome encompass cyanosis, respiratory distress, tachypnea, recurrent pneumonia, and heart failure. It can be categorized into infantile and adult forms, with the former being associated with higher mortality due to severe clinical manifestations, including pulmonary hypertension and congestive heart failure [1,5]. Managing these cases necessitates a multidisciplinary approach [6]. Treatment involves redirecting systemic arteries through catheterization and surgical corrections such as tunnel baffling or re-implanting pulmonary venous drainage into the left atrium [3,7].
This case report spotlights a unique presentation of scimitar syndrome in a 26-year-old female, underscoring its clinical importance and emphasizing the need for heightened awareness among healthcare providers. Notably, this is the first documented instance of this syndrome in Pakistan, underscoring the limited prior reports within the country. By disseminating our findings, we aim to enrich the medical literature, advance comprehension of this rare condition, and ultimately facilitate more precise diagnoses and enhanced management approaches for similar cases.
Case presentation
A 26-year-old female patient presented with a history of recurrent pulmonary infections, fever, shortness of breath, cough, and wheezing since childhood. She had been previously diagnosed and treated for asthma, but her symptoms persisted despite treatment. The patient had been married for 12 years but had no children, and she had a history of two abortions in the past. The patient's marital history and reproductive health were also significant, with a history of two abortions and no successful pregnancies. The patient's clinical history included a long-standing pattern of respiratory symptoms, which had been attributed to asthma. However, despite appropriate treatment, her symptoms continued to worsen over the years. She reported recurrent episodes of pulmonary infections, often accompanied by fever, cough, and wheezing. The initial suspicion was raised by a chest X-ray that revealed an unusual vertical tubular structure with a crescent morphology in the right hemithorax, which can be seen in Figure 1. This was the first chest X-ray the patient ever received.
A chest X-ray shows a vertical tubular structure with crescent morphology.
The chest X-ray revealed a distinctive vertically oriented tubular structure with crescent-like morphology within the right hemithorax. This discovery triggered suspicions of an underlying structural anomaly. In the subsequent steps, a computed tomography pulmonary angiogram (CTPA) was conducted to comprehensively understand the anomaly. The CTPA unveiled a peculiar vessel measuring approximately 2.1 cm that originated from the medial aspect of the right hemidiaphragm, which was a significant anomaly. This vessel was observed to connect with the inferior vena cava (IVC) just before its convergence with the right atrium. Notably, there was no noticeable loss of lung volume on either side, which strongly indicated the presence of a scimitar syndrome with partial anomalous pulmonary venous return, in line with the findings from the CT scan, as is visible in Figure 2.
A CTPA with a peculiar vessel originating from the medial aspect of the right hemidiaphragm.CTPA: computed tomography pulmonary angiography
Based on the radiological findings and clinical presentation, a diagnosis of scimitar syndrome with partial anomalous pulmonary venous return was established. This rare congenital heart anomaly involves the abnormal drainage of pulmonary veins into systemic veins, often resulting in a crescent-like shadow on imaging. Given the recurrent pulmonary infections and compromised pulmonary function, the option of surgical intervention was discussed with the patient.
The patient was extensively counseled about the condition, potential surgical approaches, and the associated risks and benefits. However, after thorough consideration, the patient and her medical team pursued a conservative management approach, emphasizing medical treatment, lifestyle modifications, and regular monitoring. The patient's medical management involved a multidisciplinary team, including pulmonologists, cardiologists, and other specialists as needed. She received tailored treatment for her recurrent pulmonary infections as well as ongoing management of her respiratory symptoms. Periodic imaging and clinical assessments were conducted to monitor the condition's progression and the patient's overall health.
Throughout follow-up, the patient's symptoms showed variable responses to medical management. While some exacerbations were managed effectively, there were instances where her respiratory symptoms required more intensive interventions. Despite these challenges, the patient remained committed to her conservative management approach, and her medical team continued to provide comprehensive care.
Discussion
Scimitar syndrome, an uncommon congenital heart anomaly, involves abnormal drainage of pulmonary veins into systemic veins, resulting in distinctive crescent-like shadows in imaging. The patient's recurring pulmonary infections and compromised lung function prompted discussions regarding the feasibility of surgical intervention. However, following thorough counseling, both the patient and the medical team opted for a conservative management approach.
Gudjonsson et al. conducted a study exploring the clinical characteristics of scimitar syndrome patients. Their findings revealed a diverse range of clinical presentations in these patients, underscoring the need for individualized management strategies to achieve optimal outcomes [8]. Meanwhile, a study by Chowdhury et al. investigated the long-term impact of surgical intervention for scimitar syndrome, demonstrating its potential to alleviate clinical symptoms and enhance overall quality of life [9]. Notably, surgical correction is warranted for cases of scimitar syndrome, particularly when accompanied by atrial septal defects (ASD), pulmonary hypertension, or anomalous vein stenosis [10].
Numerous other studies have explored management strategies for scimitar syndrome. Alghamdi et al. reported that surgical intervention remains the preferred treatment strategy, especially for symptomatic patients [11]. In contrast, Dupuis et al. revealed that conservative management can effectively treat asymptomatic patients with scimitar syndrome [12].
Detecting venous anomalies within the thorax can be achieved through various approaches, including thoracic surgery, autopsy, and diagnostic procedures like chest radiography, angiography, echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI). Notably, CT and MRI are highly effective in confirming irregularities in thoracic blood vessels. Contrast-enhanced computed tomography angiography (CTA) or magnetic resonance angiography (MRA) using contrast agents have gained recognition as versatile and non-invasive alternatives to traditional angiography [13,14]. Furthermore, advanced characterization of the anomalous right bronchial tree can be achieved through three-dimensional (3D) reconstructions of the tracheobronchial tree facilitated by spiral CT scans [13].
Conclusions
This case report highlights a remarkable instance of scimitar syndrome in a 26-year-old female, shedding light on its clinical significance and underscoring the need for heightened awareness among healthcare professionals. Notably, this case represents the rarely documented occurrence of scimitar syndrome in Pakistan, emphasizing the scarcity of prior reports within the country. By disseminating these findings, the aim is to contribute to the medical literature, enhance the understanding of this rare condition, and ultimately facilitate more accurate diagnoses and improved management strategies for similar cases. The patient's complex clinical history, the unique radiological findings, and the decision-making process regarding conservative management provide valuable insights into the challenges and considerations associated with treating this condition. As such, this report serves as a valuable addition to the medical community's understanding of scimitar syndrome and its multidisciplinary management approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Scimitar Syndrome 8 2024 Diaz-Frias J Widrich J Treasure Island (FL): Stat Pearls Publishing Stat Pearls [Internet]2023 http://www.ncbi.nlm.nih.gov/books/NBK 546602/31536209 · pubmed ↗
- 2Scimitar syndrome associated with arterial pulmonary hypertension. Report a case and literature review Curr Probl Cardiol Robledo GC Yamile Jurado Hernández M Gomez Gonzales A Alejandro Gomez Lucas S 1008554720223399403310.1016/j.cpcardiol.2021.100855 · doi ↗ · pubmed ↗
- 3Scimitar syndrome in children and adults: natural history, outcomes, and risk analysis Ann Thorac Surg Wang H Kalfa D Rosenbaum MS 59259810520182905430510.1016/j.athoracsur.2017.06.061 · doi ↗ · pubmed ↗
- 4Scimitar syndrome: the curved Turkish sabre Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu Ciçek S Arslan AH Ugurlucan M Yildiz Y Ay S 56611720142472571810.1053/j.pcsu.2014.01.003 · doi ↗ · pubmed ↗
- 5Scimitar syndrome: incidence, treatment, and prognosis Eur J Pediatr Wang CC Wu ET Chen SJ 15516016720081734509610.1007/s 00431-007-0441-z · doi ↗ · pubmed ↗
- 6Images in cardiovascular medicine. Scimitar syndrome: added value by isotropic flow-sensitive four-dimensional magnetic resonance imaging with PC-VIPR (phase-contrast vastly undersampled isotropic projection reconstruction)Circulation 8 2024 Frydrychowicz A Landgraf B Wieben O François CJ 061212010 https://pubmed.ncbi.nlm.nih.gov/20547935/10.1161/CIRCULATIONAHA.109.931857 PMC 1187217520547935 · doi ↗ · pubmed ↗
- 7Treatment and prognosis of scimitar syndrome: a retrospective analysis in a single center of East China Front Cardiovasc Med Wang K Xu X Liu T Gao W Guo Y 973796920223609313810.3389/fcvm.2022.973796 PMC 9449312 · doi ↗ · pubmed ↗
- 8Scimitar syndrome Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu Gudjonsson U Brown JW 566220061663854910.1053/j.pcsu.2006.02.011 · doi ↗ · pubmed ↗