Type 2 Myocardial Infarction Caused by Orthostatic Hypotension With Post-transcatheter Aortic Valve Implantation: A Case Report
Hitomi Tsuchida, Shiho Amano, Chiaki Sano, Ryuichi Ohta

TL;DR
An elderly patient developed type 2 heart attack after a heart valve procedure, managed through rehydration and medication adjustments.
Contribution
Highlights the multifactorial nature of type 2 MI in elderly post-TAVI patients and emphasizes tailored management strategies.
Findings
Type 2 MI occurred due to hypotension, dehydration, and left ventricular hypertrophy after TAVI.
Rehydration and diuretic cessation stabilized the patient's condition and normalized troponin levels.
Post-TAVI patients require comprehensive care to balance myocardial oxygen supply and demand.
Abstract
This case report delineates the occurrence and management of type 2 myocardial infarction (MI) in an 89-year-old woman following transcatheter aortic valve implantation (TAVI). The patient, with a history of severe aortic stenosis, hypertension, dyslipidemia, and colorectal cancer, presented with nausea and significant hypotension. Initial assessments revealed elevated troponin levels, atrial fibrillation, and ST-segment depression, leading to a diagnosis of type 2 MI. This condition was attributed to the interplay between left ventricular hypertrophy, hypotension-induced dehydration, and increased myocardial oxygen demand. The patient with post-TAVI exhibited dynamic changes in cardiac hemodynamics, with improvements in left ventricular function but persistent hypertrophy and diastolic dysfunction. This state, combined with hypotension due to diuretic-induced dehydration and atrial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
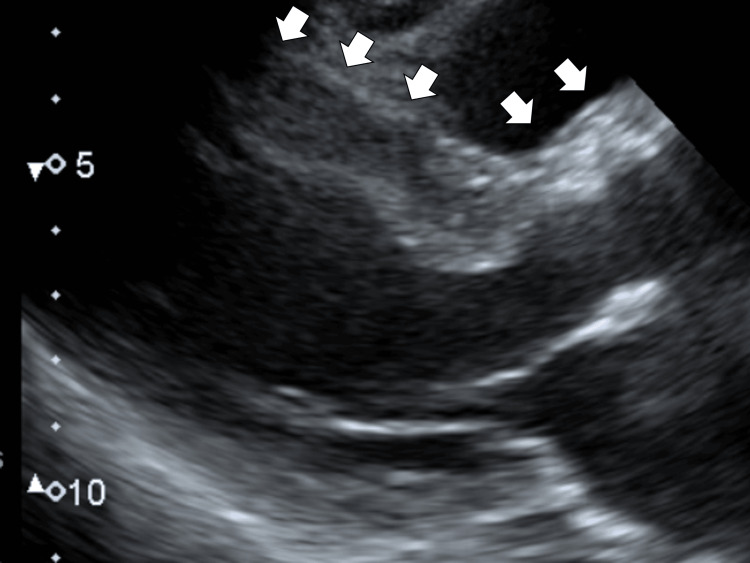 Figure 1
Figure 1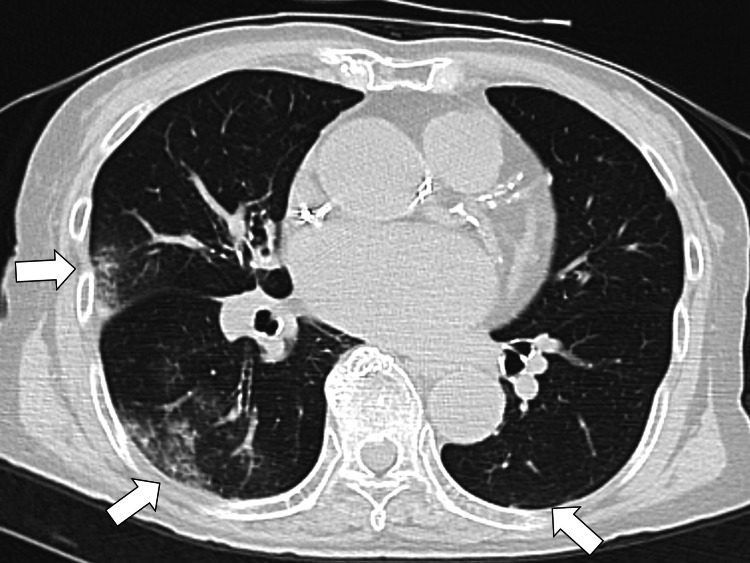 Figure 2
Figure 2| Parameter | Level | Reference |
| White blood cells | 9.3 | 3.5–9.1 × 103/μL |
| Neutrophils | 80.8 | 44.0–72.0% |
| Lymphocytes | 10.0 | 18.0–59.0% |
| Hemoglobin | 11.2 | 11.3–15.2 g/dL |
| Hematocrit | 33.5 | 33.4–44.9% |
| Mean corpuscular volume | 97.2 | 79.0–100.0 fl |
| Platelets | 16.6 | 13.0–36.9 × 104/μL |
| Total protein | 7.3 | 6.5–8.3 g/dL |
| Albumin | 3.9 | 3.8–5.3 g/dL |
| Total bilirubin | 0.6 | 0.2–1.2 mg/dL |
| Aspartate aminotransferase | 30 | 8–38 IU/L |
| Alanine aminotransferase | 12 | 4–43 IU/L |
| Lactate dehydrogenase | 326 | 121–245 U/L |
| Blood urea nitrogen | 32.7 | 8–20 mg/dL |
| Creatinine | 1.88 | 0.40–1.10 mg/dL |
| Serum Na | 143 | 135–150 mEq/L |
| Serum K | 4.9 | 3.5–5.3 mEq/L |
| Serum Cl | 108 | 98–110 mEq/L |
| CRP | 0.05 | <0.30 mg/dL |
| Troponin I | 1.064 | <0.02 ng/mL |
| Urine test | ||
| Leukocyte | 1+ | - |
| Protein | 1+ | - |
| Blood | 2+ | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Imaging and Diagnostics · Acute Myocardial Infarction Research
Introduction
In aging populations of developed countries, the number of type 2 myocardial infarctions has increased, necessitating varied case management. Myocardial infarctions (MI) are classified into five types, predominantly feature type 1, caused by coronary artery plaque changes, and type 2, resulting from an oxygen supply-demand mismatch in the myocardium [1]. Conditions like sepsis, anemia, arrhythmia, hypotension, and severe aortic stenosis can precipitate type 2 infarctions [2]. Severe aortic stenosis often leads to left ventricular hypertrophy, reducing myocardial capillary density and increasing oxygen demand [3]. This hypertrophy is implicated in myocardial ischemia in patients with non-obstructive coronary artery disease [4]. Type 2 MI usually presents mild symptoms, less noticeable electrocardiographic changes, and lower troponin levels than type 1 [5]. Diagnosis hinges on elevated cardiac troponin levels and an oxygen supply-demand imbalance unrelated to atherothrombosis [6]. Mortality risk post-event is comparable between types 1 and 2 [7]. Treatment depends on the underlying cause [5]. This case highlights a type 2 MI in an elderly woman with post-transcatheter aortic valve implantation (TAVI), attributed to left ventricular hypertrophy and hypotension-induced dehydration, underscoring the importance of tailored management for such patients.
Case presentation
Patient background
An 89-year-old woman was admitted to a rural community hospital due to pronounced symptoms of nausea and a significant decrease in blood pressure. On the day she visited the hospital, she experienced acute nausea and was unable to stand. Her systolic blood pressure was recorded at 90 mmHg, a notable drop from her usual 120 mmHg. As her symptoms persisted, she was urgently transferred to the emergency department.
Her medical history was notable for TAVI performed for severe aortic stenosis a year ago. Additionally, she had a history of heart failure, hypertension, dyslipidemia, and colorectal cancer, for which she had undergone surgery. Her current medications included sacubitril-valsartan sodium (150 mg), rosuvastatin calcium (2.5 mg), donepezil (5 mg), empagliflozin (10 mg), aspirin (100 mg), spironolactone (25 mg), bonoprazan (10 mg), and tolvaptan (7.5 mg).
Initial assessment
Upon physical examination, her vital signs were as follows: blood pressure at 92/45 mmHg, pulse rate at 130 beats/min, body temperature at 36.2°C, respiratory rate at 24 breaths/min, and an oxygen saturation of 99% on room air. The patient was coherent and alert. A cardiac examination revealed irregular heart sounds without any murmur and bilateral late crackles in the lungs without edema in the lower legs. However, the extremities were slightly cold. Laboratory findings indicated elevated cardiac markers, notably Troponin I (Table 1).
The electrocardiogram exhibited atrial fibrillation with an ST-segment depression in leads V4 and V5. Post the administration of 500 ml of extracellular fluid, her blood pressure improved to 101/61 mmHg and her heart rhythm normalized to sinus rhythm.
An echocardiographic evaluation revealed basal area hypokinesis but no significant asynergy. The left ventricular septum was thickened, measuring 13-14 mm (Figure 1).
Initial echocardiography showing left ventricular septum thickening without the narrowing aortic valve region (white arrows)
Diastolic dysfunction was evident with an E/e' of 26.6 ml/m^2^ in the ventricular septal wall (normal range: 2.6-17) and 17.7 ml/m^2^ in the lateral wall (normal range: 2.6-17). The left atrial volume index (LAVI) was 168 ml/m^2 ^(normal range: ≤28 mL/m^2^), and the tricuspid regurgitant velocity (TRV) was 3.0 m/s (normal range: ≤2.5 m/s). A chest X-ray and computed tomography showed bilateral lung congestion (Figure 2).
Chest computed tomography showing bilateral lung congestion (white arrows)
Diagnosis
The clinical presentation, alongside these findings, led to a diagnosis of type 2 myocardial infarction. This condition was attributed to reduced coronary return resulting from left ventricular hypertrophy, impaired left ventricular dilation, and hypotension due to dehydration. Contributing factors included increased oxygen demand due to atrial fibrillation and a reduced oxygen supply owing to hypotension, exacerbated by left ventricular outflow tract stenosis.
Treatment and outcome
On her second day of admission, diuretics, identified as a potential cause of her dehydration, were discontinued. Rehydration therapy was initiated, resulting in her blood pressure stabilizing at 117/54 mmHg. Troponin levels were initially elevated to 65.35 ng/ml and reduced to 45.35 ng/ml. Her blood pressure remained stable throughout her hospital stay, and her daily activities returned to pre-admission levels. Her troponin levels became normal, and she was discharged on the twenty-fifth day of her hospitalization.
Discussion
In this study, we report a case of a patient who underwent TAVI and subsequently exhibited elevated troponin levels. Notably, the patient's electrocardiography and echocardiography results did not indicate any apparent cardiovascular compromise, leading to the consideration of type 2 MI as a likely diagnosis. This case report delves into the causative factors of type 2 MI and the alterations in myocardial hemodynamics post-TAVI.
A discrepancy between heightened myocardial oxygen demand and a reduced oxygen supply characterizes type 2 MI. Factors influencing oxygen demand encompass systolic wall stress, myocardial contractility, and heart rate [8]. In the discussed case, augmented myocardial contractility, attributed to left ventricular hypertrophy and an increased heart rate due to atrial fibrillation were probable contributing factors [9]. Meanwhile, factors leading to diminished supply include compromised coronary vascular blood flow and oxygen delivery capabilities, which can be caused by coronary artery spasm, embolism, vascular endothelial dysfunction, hypotension, and anemia, as the same pathophysiology of aortic dissection [10-12].
For the patient in question, hypotension was a consequence of reduced fluid intake and circulating plasma, the latter being a result of intravascular dehydration induced by diuretic therapy for pre-existing congestive heart failure before TAVI. Additionally, a decline in cardiac output due to atrial fibrillation was observed. Furthermore, the constriction of the left ventricular outflow tract, explored in subsequent sections, may have also played a role in diminishing cardiac output and oxygen supply.
Post-TAVI cardiac alterations typically include relief of aortic valve stenosis, prompt normalization of afterload, and consequent improvements in left ventricular volume, remodeling, systolic and diastolic function, and ejection fraction [13]. However, a swift decrease in afterload may induce new dynamic intraventricular gradients and stenosis of the left ventricular outflow tract [13]. Predominant risk factors for these gradients include a small left ventricular end-diastolic diameter, elevated ejection fraction, significant valve pressure gradient, and limited left ventricular volume [14].
In the present case, the patient exhibited a higher ejection fraction due to reduced afterload and a small end-diastolic diameter (34 mm). Persistent left ventricular wall hypertrophy with a ventricular septal wall thickness of 14 mm was noted. Additionally, LAVI was 68.7 ml/m2, E/e' ratios were 26.6 (septum) and 17 (lateral), and TRV was 3.0 m/s. These findings indicated ventricular dilation defects and aligned with the aforementioned risk factors. Therefore, stenosis of the left ventricular outflow tract may have led to reduced cardiac output, culminating in a type 2 MI. Previous research has demonstrated that approximately 10% of patients experience at least one acute coronary syndrome episode within an average of 25 months post-TAVI, with type 2 MI being the most frequent, accounting for 35.9% of cases [15]. This prevalence further underscores the significance of the discussed condition as a contributing factor to type 2 MI in post-TAVI patients.
Conclusions
This case exemplifies the multifaceted etiology of type 2 myocardial infarctions. Type 2 MI can arise from various mechanisms but is particularly prevalent in patients with residual left ventricular hypertrophy and diastolic dysfunction post-TAVI. Therefore, vigilant management of additional factors that could elevate myocardial oxygen demand or curtail supply is imperative.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Type 2 myocardial infarction: a diagnostic and therapeutic challenge in contemporary cardiology Intern Emerg Med Merlo AC Bona RD Ameri P Porto I 3173241720223515721510.1007/s 11739-021-02920-8PMC 8853072 · doi ↗ · pubmed ↗
- 2Type II myocardial infarction: predisposing factors, precipitating elements, and outcomes Cureus Pillai B Trikkur S Farooque U 012202010.7759/cureus.9254 PMC 743069532821600 · doi ↗ · pubmed ↗
- 3Myocardial oxygen consumption during exercise in the presence of left ventricular hypertrophy secondary to supravalvular aortic stenosis J Am Coll Cardiol Bache RJ Dai XZ 11571164151990213818510.1016/0735-1097(90)90258-q · doi ↗ · pubmed ↗
- 4Left ventricular hypertrophy contributes to Myocardial Ischemia in Non-obstructive Coronary Artery Disease (the Micro CAD study)Int J Cardiol Eskerud I Gerdts E Larsen TH Lønnebakken MT 1628620193095252910.1016/j.ijcard.2019.03.059 · doi ↗ · pubmed ↗
- 5Type 2 MI and myocardial injury in the era of high-sensitivity troponin Eur Cardiol Rafiudeen R Barlis P White HD van Gaal W 017202210.15420/ecr.2021.42PMC 890013235284006 · doi ↗ · pubmed ↗
- 6Fourth universal definition of myocardial infarction (2018)J Am Coll Cardiol Thygesen K Alpert JS Jaffe AS Chaitman BR Bax JJ Morrow DA White HD 223122647220183015396710.1016/j.jacc.2018.08.1038 · doi ↗ · pubmed ↗
- 7Long-term outcomes in patients with type 2 myocardial infarction and myocardial injury Circulation Chapman AR Shah AS Lee KK 1236124513720182915042610.1161/CIRCULATIONAHA.117.031806 PMC 5882250 · doi ↗ · pubmed ↗
- 8Patient Characteristics and Clinical Outcomes of Type 1 Versus Type 2 Myocardial Infarction J Am Coll Cardiol Mc Carthy CP Kolte D Kennedy KF Vaduganathan M Wasfy JH Januzzi JL Jr 8488577720213360246610.1016/j.jacc.2020.12.034 · doi ↗ · pubmed ↗