Common bile duct polyp: an infrequent cause of jaundice and biliary obstruction
Gerly E. Guzmán-Calderon, Carlos Huaraca, Brandon Bravo, Joseph Arzapalo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
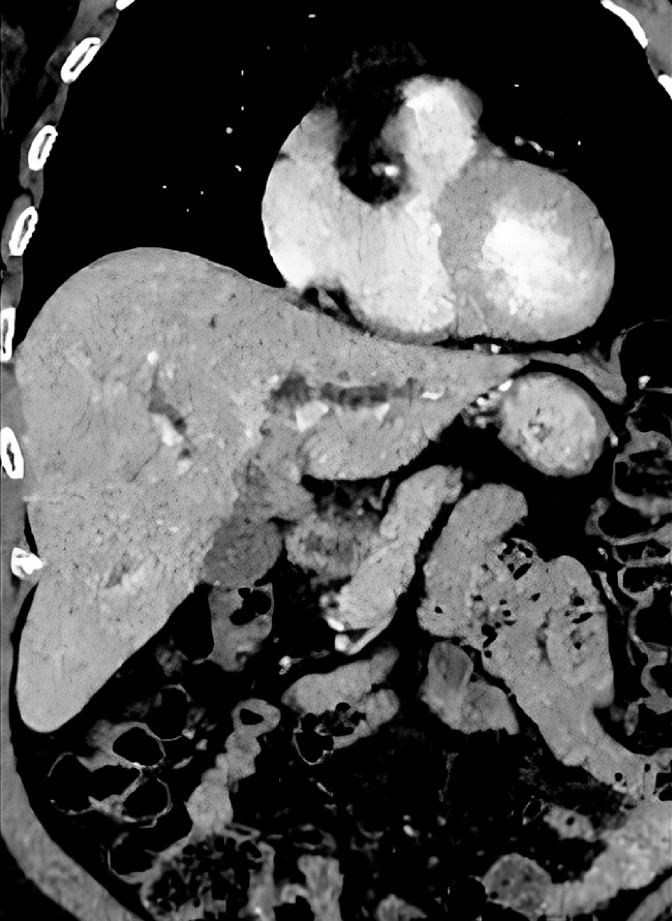 Fig. 1
Fig. 1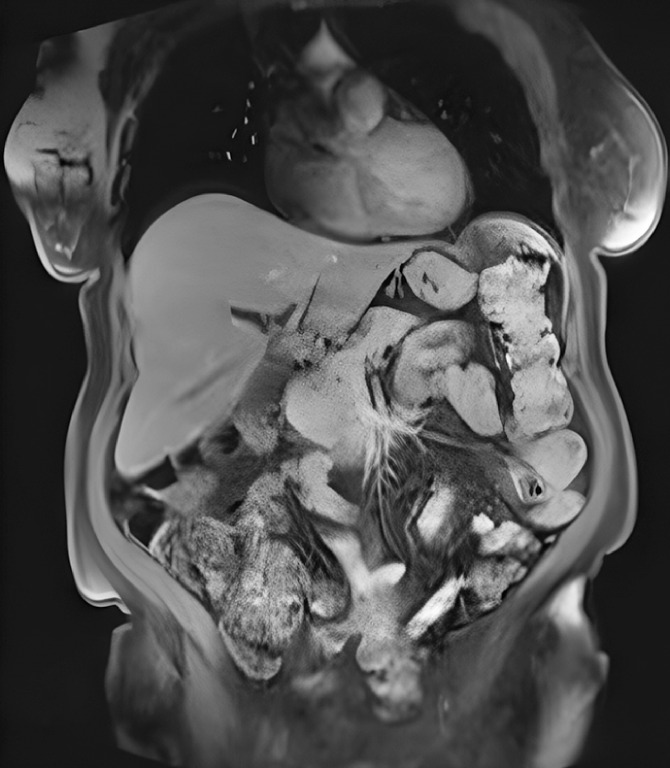 Fig. 2
Fig. 2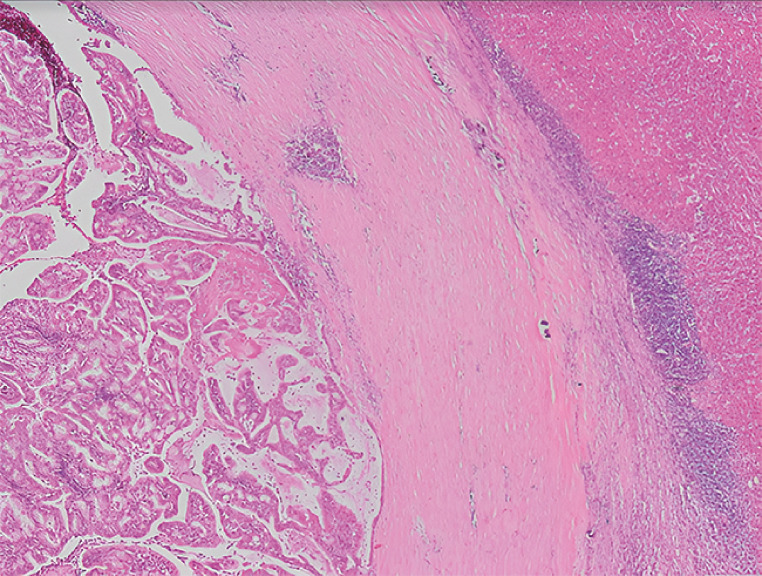 Fig. 3
Fig. 3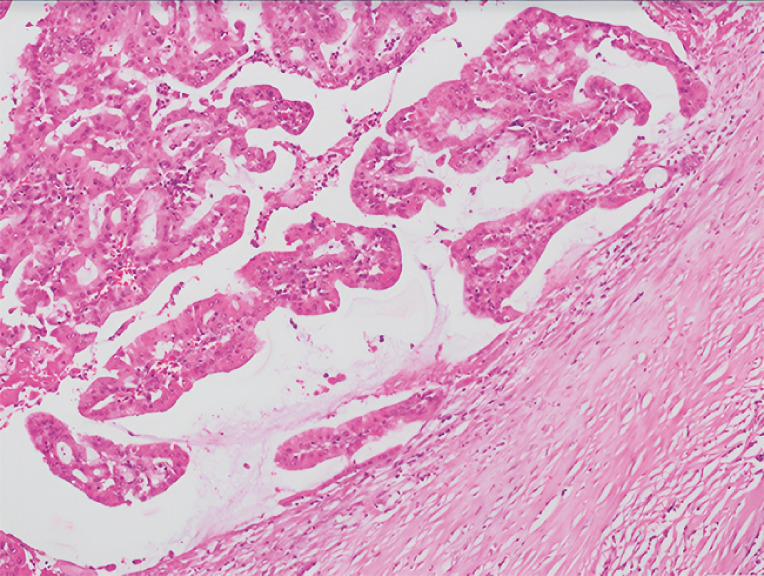 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Gallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments
The most common etiology of common bile duct (CBD) obstruction is bile duct stones; less common causes include biliary polyps and intraductal papillary neoplasm of the bile duct (IPNB). Initially described by Nakamura et al. 1 in 2010, IPNB is defined as a pedunculated mass with intraluminal growth exhibiting significant malignant potential that can subsequently lead to cholangiocarcinoma.
We present the case of a 75-year-old woman with a history of jaundice and mild abdominal pain. Computed tomography and magnetic resonance cholangiopancreatography showed circumferential thickening of the proximal CBD and left hepatic duct ( Fig. 1 , Fig. 2 ). Liver function tests confirmed a cholestatic pattern, with total bilirubin of 7.4 mg/dL, direct bilirubin of 5.3 mg/dL, alkaline phosphatase of 475 IU/L, and normal CA 19.9 level. Cholangioscopy revealed a single whitish papillary mass with a regular surface, located between the proximal CBD and left hepatic duct, obstructing approximately 80% of the biliary lumen ( Video 1 ). Multiple samples were obtained using SpyBite forceps (Boston Scientific, Marlborough, Massachusetts, USA). Histological analysis confirmed the presence of an IPND with high grade dysplasia ( Fig. 3 , Fig. 4 ). The patient underwent left hepatectomy. The surgical specimen demonstrated a 17-mm lesion with biliopancreatic epithelium, involvement of the left hepatic duct, and no evidence of invasive carcinoma ( Fig. 4 ).
Computed tomography showing circumferential thickening of the proximal common bile duct and left hepatic duct.
Magnetic resonance cholangiopancreatography showing circumferential thickening of the proximal common bile duct and left hepatic duct.
Histopathological image showing cubic monostratified papillary biliary epithelium and intraductal papillary neoplasia. Externally, a fibrous capsule delimits the liver tissue with an inflammatory infiltrate (hematoxylin and eosin, × 4).
Histopathological image showing a papillary neoplasia with a fibrovascular core, as well as areas of high grade dysplasia in the gastric and pancreatobiliary epithelium, without evidence of invasive carcinoma (hematoxylin and eosin, 10×).
Cholangioscopy showing a single, whitish papillary mass with a regular surface, located between the proximal common bile duct (CBD) and left hepatic duct.Video 1
Biliary polyps are classified as IPNBs. Given their potential to cause obstructive jaundice and cholangitis, as well as a high malignant potential, IPNBs must be treated surgically 2 3 . Our case underscores the value of performing cholangioscopy with targeted biopsies for the assessment and characterization of CBD tumors.
Endoscopy_UCTN_Code_TTT_1AR_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nakanuma Y Sato Y Harada K Pathological classification of intrahepatic cholangiocarcinoma based on a new concept World J Hepatol 20101241942710.4254/wjh.v 2.i 12.419PMC 301051121191517 · doi ↗ · pubmed ↗
- 2Nakaoka K Hashimoto S Kawabe NA rare case of inflammatory polyp in the common bile duct with cholangitis DEN Open 20223 e 14335898824 10.1002/deo 2.143PMC 9307733 · doi ↗ · pubmed ↗
- 3Nakanuma Y Sato Y Ikeda H Intrahepatic cholangiocarcinoma with predominant “ductal plate malformation” pattern: a new subtype Am J Surg Pathol 2012361629163523073321 10.1097/PAS.0b 013e 31826 e 0249 · doi ↗ · pubmed ↗