Mature Spinal Teratoma: A Case Report
Jorge Del Pino-Camposeco, Eliezer Villanueva-Castro, Obet Canela-Calderon, Juan Antonio Ponce-Gómez, Noe Alejandro Salazar Felix, Juan Nicasio Arriada-Mendicoa

TL;DR
A 76-year-old woman with a rare spinal teratoma underwent surgery, and the tumor was confirmed as a mature teratoma with no malignant components.
Contribution
This case report presents a rare instance of a mature spinal teratoma in an elderly patient and its successful surgical management.
Findings
The lesion was identified as a mature teratoma based on histopathological findings.
The patient experienced no neurological deficits post-surgery.
At six months post-surgery, the patient had persistent paresthesia but no motor weakness.
Abstract
We presented an unusual case of a teratoma in a 76-year-old female who began four years ago with paresthesias and hypoesthesias in the sacral and gluteal regions. She denied weakness or gait instability. The magnetic resonance imaging showed an intradural lesion within the cauda equina at levels L2-L3. We decided to perform a posterior midline approach to the lumbar region to expose L2-L3 levels. After doing the L2-L3 laminectomy and the durotomy, we found a solid lesion surrounded by nerve roots with heterogeneous content. Through the meticulous separation of the nerve roots surrounding the lesion, we punctioned it, observing the exit of melanocytic material. Histopathological findings showed germinal neoplasia without immature neuroepithelium or malignant component; therefore, the diagnosis of mature teratoma was made. The patient was discharged without any aggregate neurological…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1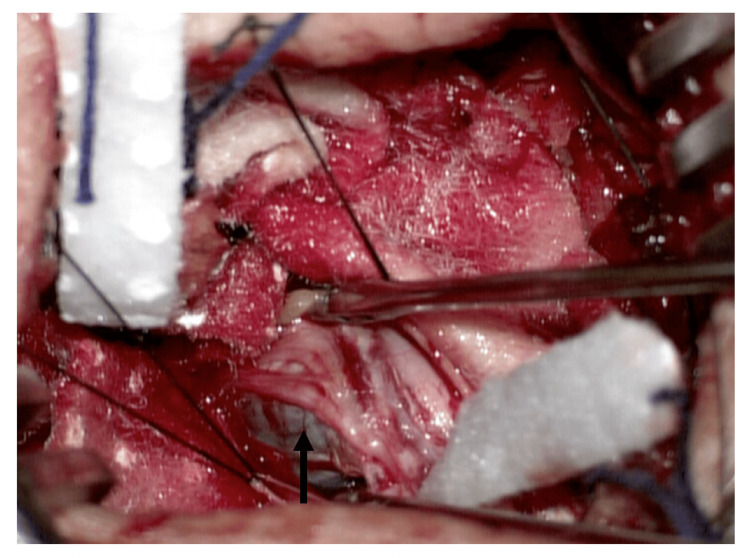 Figure 2
Figure 2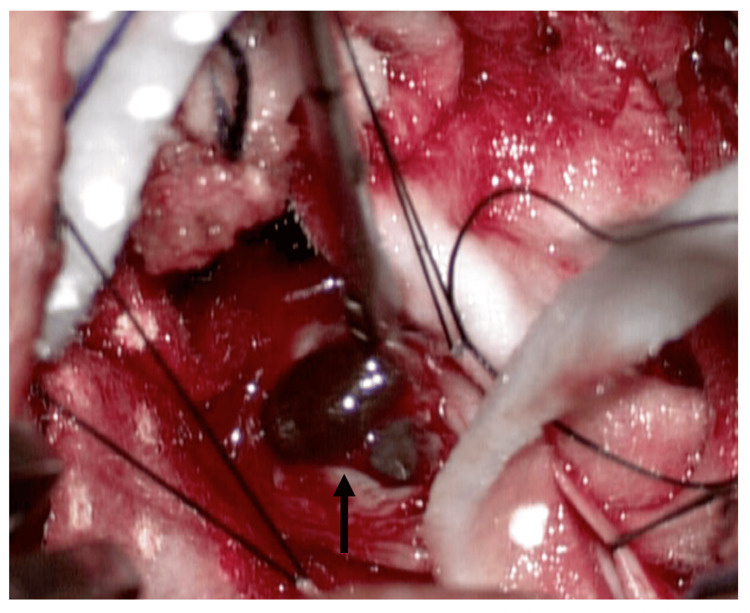 Figure 3
Figure 3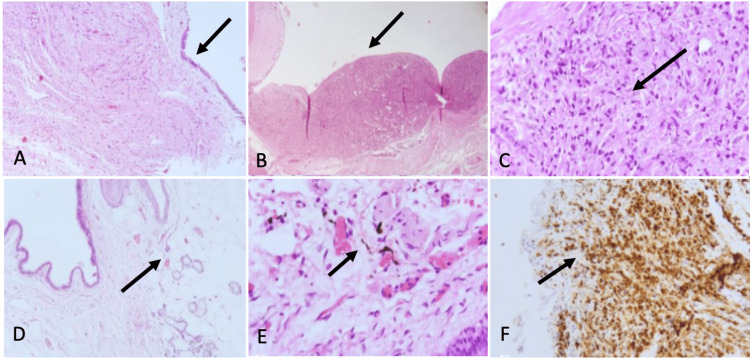 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Dysraphism and Malformations · Teratomas and Epidermoid Cysts · Head and Neck Surgical Oncology
Introduction
Central nervous system (CNS) teratomas are infrequent; in the majority of cases, they are intracranial, located in the pineal gland, posterior fossa, cerebral hemispheres, and suprasellar region [1]. True teratomas are classified as tumors generated from all three germ layers; teratomas are tumors of germ cell or dysembryogenic origin that arise from the ectopic development of two or more totipotent cell lines (ectoderm, mesoderm, and endoderm) [2,3]. Based on the degree of differentiation, teratomas are classified into three: malignant, immature, and mature. The origin of spinal cord teratoma is controversial; misdisplacement of multipotential germinal cells is the most accurate theory [4]. Teratomas can be found throughout the spine, with more prevalence in the thoracic and lumbar regions and most frequently in the conus medullaris [5]. Despite the fact that these tumors can appear in various locations, teratomas make up less than 1% of CNS tumors and are extremely rare in the spinal cord [6]. Since teratomas have an unpredictable natural progression, total surgical removal is often the main primary treatment [7]. Symptomatic recurrence in mature teratomas is uncommon, even in cases with subtotal resection, The recurrence rate has been reported at about 10%, predominantly seen in immature and malignant forms [8].
Case presentation
The case of a 76-year-old female patient with no significant personal pathological history is presented. Her condition began four years ago with paresthesias and hypoesthesias in the sacral and gluteal regions, irradiation to the right pelvic limb, and stress urinary incontinence. She denied weakness or gait instability. On the neurological examination, the patient was conscious, alert, and oriented in person, time, and place. Mental functions and the cranial nerves were preserved. Cerebellum without pathological findings. Strength was 5/5 in the upper limbs and 4+/5 in the lower limbs based on Daniel´s strength scale, proximal and distal. The sensation was intact to pinprick, vibration, and proprioception; she had hypoesthesia in L4 distribution in both lower limbs with a light touch. Muscle stretch reflexes were ++ in the upper and lower extremities. Bilateral flexor plantar response. Magnetic resonance was performed in T2, T1, and fat suppression sequences, which showed a Hypointense lesion inside the spinal canal without foraminal or paravertebral extension within the cauda equina at levels L2-L3 (Figure 1).
Preoperative imaging studiesA sagittal T2 sequence MRI shows a tumor in L2-L3 intervertebral space (yellow arrow).
Based on clinical and image findings, we concluded this lesion was a spinal intradural extramedullary tumor to rule out a neurofibroma or schwannoma. We decided to perform a posterior midline approach to the lumbar region to expose L2-L3 levels. After doing the L2-L3 laminectomy and the durotomy, we found a solid lesion surrounded by nerve roots with heterogeneous content (Figure 2). Through the meticulous separation of the nerve roots surrounding the lesion, we punctioned it, observing the exit of melanocytic material (Figure 3). After aspiration of all the contents, the residual lesion was separated from the nerve roots and completely resected. After three days of intrahospital recovery, the patient was discharged without any aggregate neurological deficit. At the six-month follow-up visit, the patient continued with paresthesia in the gluteal region without motor weakness and reported minimal gait improvement.
Transoperative image oneThe tumor was involved in the nerve roots of the cauda equina(black arrow).
Transoperative image twoThe tumor after separation of nerve roots and puncture with the exit of the melanocytic component (black arrow).
Histopathological findings
Germinal neoplasia is obtained through histological sections with the presence of cellular components from the three germ layers. A cystic area is observed covered by ciliated columnar epithelium; in some areas, it is pseudostratified with goblet cells. Basement membrane and fibrous or subepithelial tissue with variable degrees of cellularity, the presence of cerine glands, mature adipose tissue, and smooth muscle fibers are observed. Irregular and tortuous nerve tracts are observed, and some spindle cells show melanin pigment. Areas with mature brain tissue are identified. No immature neuroepithelium or malignant neoplasm is identified (Figure 4).
Histopathological findings(A) Panoramic view of a cyst delineated by epithelium. The cystic wall is made of fibrous and nervous tissue (H&E; 4X) (black arrow); (B) Nodular and disorganized proliferation of cells from ectodermal and mesodermal origin (H&E; 4X) (black arrow). (C) A nest composed of fusiform cells with hyperchromatic nuclei and some pigment inside the cytoplasm (H&E; 40x) (black arrow). (D) Cyst wall with ectodermal components, adipose tissue and glands (H&E; 4x) (black arrow). (E) The epithelium is columnar, pseudostratified with cilia, with respiratory phenotype. Some pigmented fusiform cells can be seen (H&E; 40X) (black arrow). (F) Cells of the nodular proliferation showed Melan A immunoreactivity (10X) (black arrow).
Discussion
Spinal teratomas are uncommon lesions. They account for only 0.2-0.5% of all spinal cord tumors [5,9]. The clinical presentation of adults is highly variable depending on the location of the tumor in the spine (cervical, thoracic, or lumbosacral) and whether the tumor is intramedullary, intradural, extramedullary, or extradural [5]. Mature intraspinal teratomas in adults are generally slow-growing, located generally between the lower thoracic region and the lower thoracic medullary conus [10]. The patient in our case only had a mild motor deficit that limited ambulation without pain, and the lesion was located at the beginning of the cauda equina in L2-L3.
Both mature and immature teratomas are generally benign, particularly when promptly treated. Mature teratomas contain components that are completely differentiated. Immature lesions usually contain fetal tissue. Malignant teratomas have the malignant component of the germ cell layer [5]. In the case presented, the histopathological findings showed areas with mature brain tissue. No immature neuroepithelium or malignant neoplasm was identified; therefore, the diagnosis of mature teratoma was made.
Teratomas are generally well encapsulated, have solid and cystic components, and show mixed signal intensities. Teratoma lesions have the following MRI image characteristics: well defined and they could have a thick wall circular or lobulated encapsulated cystic mass, hyperintense on T1 and T2 and hypointense images by the presence of adipose tissue on fat suppression sequences, calcifications, which mostly appear hypointense on all sequences, slight enhancement after contrast administration, sometimes associated with dysraphic congenital anomalies [11]. Recurrence depends on the histological features of the tumor; it is more frequently found in immature and malignant teratomas. However, symptomatic recurrence of mature teratomas is low, even in subtotal resections [2,5].
Conclusions
Due to the benign nature of these tumors and their generally satisfactory long-term results with minimal recurrence rate, total surgical excision is the main action; nevertheless, it is advisable to do long-term surveillance. Although there are certain image characteristics that can suggest the presence of a spinal teratoma, the intraoperative and histopathological examinations provide the definitive diagnosis. It is unclear how adjuvant treatments, such as chemotherapy and radiation therapy, should be used for residual tumors. As demonstrated in this case, the majority of these patients may experience a very positive neurologic recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Teratomas in central nervous system: a clinico-morphological study with review of literature Neurol India Agrawal M Uppin MS Patibandla MR 8418465820102115004610.4103/0028-3886.73740 · doi ↗ · pubmed ↗
- 2Adult intramedullary mature teratoma of the spinal cord: review of the literature illustrated with an unusual example Acta Neurochir (Wien) Ak H Ulu MO Sar M Albayram S Aydin S Uzan M 66366914820061652322310.1007/s 00701-006-0755-z · doi ↗ · pubmed ↗
- 3An infantile large and extensive intramedullary mature spinal teratoma Neurol Med Chir (Tokyo) Ishiguro S Nagashima T Yamamoto K Kanekawa K Yoshida M Kondoh T 3933965120112161377010.2176/nmc.51.393 · doi ↗ · pubmed ↗
- 4Dysontogenetic brain tumours--proposal for an improved classification Neuropathol Appl Neurobiol Walter GF Kleinert R 273287131987282142210.1111/j.1365-2990.1987.tb 00067.x · doi ↗ · pubmed ↗
- 5Intramedullary spinal teratoma presenting with urinary retention: case report and review of the literature Neurosurgery Poeze M Herpers MJ Tjandra B Freling G Beuls EA 3793854519991044908510.1097/00006123-199908000-00038 · doi ↗ · pubmed ↗
- 6Imaging characteristics of primary intracranial teratoma Acta Radiol Liu Z Lv X Wang W 8748815520142410391610.1177/0284185113507824 · doi ↗ · pubmed ↗
- 7A special case of intramedullary teratoma in an adult. Literature review Revista Médica del Hospital General de México Barahona EA Olvera JN Liquidano ME 237242812018 https://pdf.sciencedirectassets.com/308533/1-s 2.0-S 0185106318 X 00067/1-s 2.0-S 0185106316301020/main.pdf?X-Amz-Security-Token=I Qo Jb 3Jp Z 2lu X 2Vj E Jz%2F%2F%2F%2F%2F%2F%2F%2F%2F%2Fw Ea CX Vz LW Vhc 3Qt MSJGMEQCIG 1Ef WLG Gcdu CAX 6y 5p A 9brb DV Hqk 4AGI 9NN Sc N 4xgw 1Ai BXT 4E Gt%2B 6l WELS Dz Ykfw 8Jy 9Ta X Ztn FJ 6b 48N 2G Ant X Sqz B Qh VEA Ua DDA 1OT Aw Mz U 0Njg 2NSIM Nn 2vwy Fh 6j RUZ 5vo Kp AF
- 8Pediatric intramedullary teratomas Neuropediatrics Işik N Balak N Silav G Elmaci I 1961993920081916570610.1055/s-0028-1112116 · doi ↗ · pubmed ↗