Investigating the Association Between Extended Participation in Collision Sports and Fluid Biomarkers Among Masters Athletes
Lauren P. Giesler, William T. O'Brien, Georgia F. Symons, Sabrina Salberg, Gershon Spitz, Robb Wesselingh, Terence J. O'Brien, Richelle Mychasiuk, Sandy R. Shultz, Stuart J. McDonald

TL;DR
This study found no significant differences in brain injury or inflammation biomarkers between amateur athletes with long collision sport histories and those without.
Contribution
Preliminary evidence that biomarkers may not change in asymptomatic amateur athletes with long collision sport participation.
Findings
No significant differences in plasma biomarkers like GFAP, NfL, and UCH-L1 between collision and non-collision athletes.
Salivary inflammation and telomere-related markers were similar between the two groups.
Symptom frequency and severity were not significantly different between groups.
Abstract
Traumatic brain injuries (TBIs) and concussions are prevalent in collision sports, and there is evidence that levels of exposure to such sports may increase the risk of neurological abnormalities. Elevated levels of fluid-based biomarkers have been observed after concussions or among athletes with a history of participating in collision sports, and certain biomarkers exhibit sensitivity toward neurodegeneration. This study investigated a cohort of 28 male amateur athletes competing in “Masters” competitions for persons >35 years of age. The primary objective of this study was to compare the levels of blood and saliva biomarkers associated with brain injury, inflammation, aging, and neurodegeneration between athletes with an extensive history of collision sport participation (i.e., median = 27 years; interquartile range = 18–44, minimum = 8) and those with no history. Plasma proteins…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
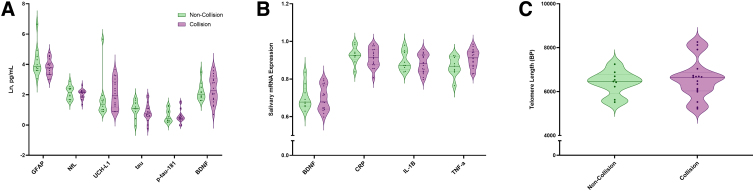 FIG. 1
FIG. 1| Non-collision ( | Collision (n = 18) | ||
|---|---|---|---|
| Age | 52.0 (47.8–56.1) | 54.0 (48.7–60.3) | 0.601 |
| BMI | 26.0 (24.7–27.7) | 26.7 (25.3–28.1) | 0.471 |
| Years of sport participation | 40.0 (23.5–45.5) | 41.0 (20.0–46.0) | 0.918 |
| Years of collision sport participation | 0.0 (0.0–0.0) | 27.0 (17.8–44.3) |
|
| Age commenced sport | 7.0 (5.5–16.3) | 8.0 (6.0–9.0) | 0.173 |
| Age commenced collision sport | N/A | 9.5 (9.0–13.0) | |
| Consecutive years playing collision sport before study |
| ||
| N/A-Miss | 100 (100.0%) | 3 (16.7%) | |
| 0–5 years | 0 (0.0%) | 3 (16.7%) | |
| 6–10 years | 0 (0.0%) | 1 (5.6%) | |
| >10 years | 0 (0.0%) | 11 (61.1%) | |
| History of concussion | 0.092 | ||
| N/A-Miss | 1 (10.0%) | 0 (0.0%) | |
| Yes | 4 (40.0%) | 14 (77.8%) | |
| No | 5 (50.0%) | 4 (22.2%) | |
| No. of past concussions | 0.0 (0.0–1.0) | 2.5 (0.8–7.0) |
|
| Medical Dx | 0.0 (0.0–0.0) | 0.0 (0.0–2.3) | 0.244 |
| Self-report | 1.0 (1.0–1.8) | 3.0 (1.8–6.8) | 0.195 |
| History of LOC | 0.123 | ||
| N/A-Miss | 6 (60.0%) | 4 (22.2%) | |
| Yes | 2 (20.0%) | 9 (50.0%) | |
| No | 2 (20.0%) | 5 (27.8%) | |
| No. of LOCs | 0.0 (0.0–1.5) | 1.0 (0.0–1.3) | 0.477 |
| Years since last concussion | 15.0 (3.5–30.3) | 6.0 (2.0–21.5) | 0.540 |
| Hypertension | 0.927 | ||
| Yes | 1 (10.0%) | 2 (11.1%) | |
| No | 9 (90.0%) | 16 (88.9%) | |
| Diabetes mellitus | 0.662 | ||
| Yes | 1 (10.0%) | 1 (5.6%) | |
| No | 9 (90.0%) | 17 (94.4%) | |
| Heart conditions | 0.410 | ||
| Yes | 3 (30.0%) | 3 (16.7%) | |
| No | 7 (70.0%) | 15 (83.3%) | |
| Lung conditions | 0.236 | ||
| Yes | 2 (20.0%) | 1 (5.6%) | |
| No | 8 (80.0%) | 17 (94.4%) | |
| Thyroid disease | 0.172 | ||
| Yes | 1 (10.0%) | 0 (0.0%) | |
| No | 9 (90.0%) | 18 (100%) | |
| Renal insufficiency | 0.172 | ||
| Yes | 1 (10.0%) | 0 (0.0%) | |
| No | 9 (90.0%) | 18 (100%) | |
| Stroke | 0.448 | ||
| Yes | 0 (0.0%) | 1 (5.6%) | |
| No | 10 (100.0%) | 17 (94.4%) | |
| Headache/migraine | 0.507 | ||
| Yes | 4 (40.0%) | 5 (27.8%) | |
| No | 6 (60.0%) | 13 (72.2%) | |
| Seizure/epilepsy | 0.662 | ||
| Yes | 1 (10.0%) | 1 (5.6%) | |
| No | 9 (90.0%) | 17 (94.4%) | |
| Cancer | 0.629 | ||
| Yes | 1 (10.0%) | 3 (16.7%) | |
| No | 9 (90.0%) | 15 (83.3%) | |
| Arthritis | 0.373 | ||
| N/A-Miss | 0 (0.0%) | 1 (10.0%) | |
| Yes | 1 (10.0%) | 5 (27.8%) | |
| No | 9 (90.0%) | 12 (66.7%) | |
| Psychiatric illness |
| ||
| Yes | 0 (0.0%) | 6 (33.3%) | |
| No | 10 (100.0%) | 12 (66.7%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury Research · S100 Proteins and Annexins · Traumatic Brain Injury and Neurovascular Disturbances
Introduction
Repetitive traumatic brain injuries (TBIs) and concussions are common in collision sports, such as the football codes, and combat and equestrian sports.^1–3^ Considerable research has focused on the potential effects of concussion and TBI exposure in current or retired athletes with lengthy careers at the college or professional sports level.^4,5^ However, collision sports are also commonly participated in at the community level, and, in some cases, athletes continue to partake in these sports into middle age. In Australia, for example, “Masters” competitions for persons >35 years of age are common for collision sports, including Australian football. Although the health benefits of sport participation are numerous, it is important to understand how prolonged amateur/community collision sport participation into older years may influence neurological health. Previous research has extensively focused on professionals, retired professionals, and young athletes, leaving the Masters cohort notably under-represented.
Fluid biomarkers can potentially serve as indirect indicators of neurological injury or disease.^6^ Proteins such as glial fibrillary acidic protein (GFAP), neurofilament light (NfL), ubiquitin C-terminal hydrolase L1 (UCH-L1), tau, and tau phosphorylated at threonine 181 (p-tau-181) have been shown to be elevated in blood after TBIs^7,8^ or in persons with age-related neurodegeneration or neurodegenerative disease.^9^ Evidence suggests that fluid biomarkers associated with inflammation may be elevated in collision sports athletes,^10,11^ and chronic neuroinflammation has been implicated in cognitive decline and neurodegeneration.^12^ Brain-derived neurotrophic factor (BDNF) is a neurotrophin with important roles in the development and maintenance of the central nervous system, with alterations in BDNF messenger RNA (mRNA) and protein levels found in studies of brain injury and neurodegenerative disease.^13,14^ In addition, shortened saliva telomere length has been associated with aging processes and neurodegeneration,^15^ as well collision sport participation in cohorts of younger athletes.^16^ Therefore, panels consisting of these promising biomarker candidates hold the potential to offer insights into the neurological well-being of older, highly active athletes who have been extensively involved in collision sports.
This pilot study aims to compare blood and salivary biomarkers between older Australian football Masters athletes with an extensive history of collision sport participation compared with non-collision sport field hockey Masters athletes.
Methods
Participants
A total of 32 male Masters athletes were recruited for this study through convenience sampling, including 19 active collision sport (i.e., Australian football) athletes from an amateur Australian football club, and 13 active non-collision sport (i.e. field hockey) athletes from a field hockey club. Inclusion criteria for the collision sport cohort were: 1) age >35 years; 2) significant history of collision sport participation, defined here as >8 years. Non-collision controls were >35 years of age, had participated in non-collision sport for >8 years, and had no history of collision sport participation. For sporting history classification, collision sport participation was defined as any participation in Australian football, gridiron, rugby, ice hockey, lacrosse, or combat sport. Sports outside of this classification were ruled to be non-collision. This research was approved by the Alfred Health Human Research Ethics Committee (#187/18).
Clinical questionnaires
Participants completed questionnaires pertaining to demographics, and medical, sporting, and drug and alcohol history. The Sport Concussion Assessment Tool–5th Edition (SCAT5) was used to quantify concussion-related symptoms.
Blood analysis
Venous blood was collected into ethylenediaminetetraacetic acid tubes, with plasma isolated after centrifugation at 1100g and stored at −80°C. A Simoa HD-X Analyzer was used to quantify GFAP, NfL, UCH-L1, and tau (Neurology 4-plex B), pTau-181 (pTau-181 V2 Advantage), and BDNF (BDNF Discovery kit) as per the manufacturer's instructions. Assays were performed in a temperature-controlled laboratory by an experimenter blinded to the clinical information. All samples were tested in duplicate and measured above the lower limit of quantification for GFAP (9.38 pg/mL), NfL (0.500 pg/mL), tau (0.125 pg/mL), p-tau-181 (0.085 pg/mL), and BDNF (0.029 pg/mL). For UCH-L1, 10 of 28 samples were below the lower limit of detection and thus assigned this value: 2.43 pg/mL. The average interplate coefficient of variation of samples for GFAP, NfL, UCH-L1, tau, p-tau-181, and BDNF was 9%, 7%, 46%, 6%, 6%, and 5%, respectively.
Saliva analysis
Saliva samples, collected using Oragene DNA (OG-500) kits per the manufacturer's instructions for future RNA and DNA isolation, underwent RNA extraction with the Allprep DNA/RNA Mini Kit. RNA concentration and quality were assessed using the Nanodrop 2000. Two micrograms of RNA were reverse transcribed into complementary DNA (cDNA) using qScript™ XLT cDNA SuperMix. For qRT-PCR, 10 ng of cDNA, 1X SYBR Green FastMix ROX, and 0.5-μM forward and reverse primers were used, with all samples run in duplicate on a 96-well plate using the CFX Connect-Real-Time PCR Detection system. Analysis utilized the 2^(-ΔΔCT) method, normalized against housekeeping genes Cyca and Ywhaz, following Pfaffl^17^ and Bonefeld.^18^
For telomeres, DNA extraction utilized the QIAamp DNA Mini Kit per the manufacturer's instructions, with DNA concentration and quality evaluated by the Nanodrop 2000. DNA was diluted to 20 ng/μL with TE buffer for downstream quantitative real-time polymerase chain reaction (qRT-PCR). Samples were run in duplicate on the CFX Connect-Real-Time PCR Detection system with 1X SYBR Green FastMix ROX and appropriate primers, totaling 20 μL per well. Relative telomere quantification involved comparing the telomere to single-copy 36B4 gene ratio (T/S), calculated as approximately [2Ct(telomere)/2Ct(36B4)]−1 = −2−ΔCt. Telomere length was determined using the linear regression equation: y = 1910.5x + 4157, with y representing telomere length and x corresponding to −2−ΔCt.^19^ Primer sequences and cycling parameters for qRT-PCR analysis are available upon request.
Statistical analysis
Statistical analyses were conducted in R software (version 4.0.3; R Foundation for Statistical Analysis, Vienna, Austria). All analyses were two-tailed, with a significance level of p < 0.05. Demographic variables were compared using unpaired t-tests. Nominal variables were evaluated using Pearson's chi-squared (χ^2^) test. Biomarker data underwent natural logarithm transformation before analysis. To investigate the relationship between sport group and fluid biomarkers, we performed multiple linear regression analysis controlling for age and body mass index (BMI).
Results
Demographic information
Four participants initially recruited to the study were excluded from all analyses; 1 collision athlete had not played collision sport for >8 years, and 3 non-collision athletes reported a significant history of collision sport participation (i.e., ≥20 years). Two additional participants were unable to complete the saliva collection, but remained in the study for all other analyses. Demographics, sporting, and medical histories of each group are detailed in Table 1. Primary differences in cohorts included were that collision athletes had more years of collision sport participation compared to the non-collision sport group (p < 0.001). There were no differences in participant age, years of sport participation, participant age at the commencement of sport, or years since most recent concussion between groups. However, the collision sport group reported having sustained more concussions than those in the non-collision sport group (p = 0.040).
Symptomatology
There were no differences in self-reported symptom number (p = 0.347) or self-reported symptom severity (p = 0.324) on the SCAT5 between groups.
Plasma biomarkers
As shown in Figure 1A, there were no effects of collision sport participation for plasma levels of GFAP (estimate = −0.43, confidence interval [CI] = −1.02 to 0.17, p = 0.153), NfL (estimate = −0.09, CI = −0.34 to 0.17, p = 0.482), UCH-L1 (estimate = 0.29, CI = −0.67 to 1.25, p = 0.541), tau (estimate = −0.20, CI = −0.66 to 0.25, p = 0.368), p-tau-181 (estimate = −0.05, CI = −0.39 to 0.30, p = 0.782), and BDNF (estimate = 0.07, CI = −0.54 to 0.67, p = 0.817).
Fluid biomarkers in collision and non-collision sport Masters athletes. (A) No differences in plasma concentrations of GFAP, NfL, UCH-L1, tau, p-tau-181, or BDNF were observed between collision and non-collision Masters athletes. (B) No differences in saliva biomarkers BDNF, CRP, IL-1β, or TNF-α were observed between collision and non-collision Masters athletes. (C) No differences in telomere length were observed between collision and non-collision Masters athletes. BDNF, brain-derived neurotrophic factor; CRP, C-reactive protein; GFAP, glial fibrillary acidic protein; IL-1β, interleukin-1 beta; NfL, neurofilament light; p-tau-181, tau phosphorylated at threonine 181; TNF-α, tumor necrosis factor-alpha; UCH-L1, ubiquitin C-terminal hydrolase L1.
Salivary messenger RNA
For BDNF (estimate = −0.01, CI = −0.08 to 0.07, p = 0.873), C-reactive protein (CRP; estimate = −0.02, CI = −0.06 to 0.03, p = 0.488), interleukin-1 beta (IL-1 ; estimate = −0.01, CI = −0.06 to 0.04, p = 0.593), and tumor necrosis factor alpha (TNF- ; estimate = 0.05, CI = 0.00–0.10, p = 0.062), no effects of collision sport were found (Fig. 1B).
Telomere length
For telomere length (Fig. 1C), no effect of collision sport was observed (estimate = 0.02, CI = −0.09 to 0.13, p = 0.708).
Discussion
This pilot study found that an extended history of amateur collision sport participation into middle age did not have a significant effect on plasma biomarker levels of neuronal (i.e., UCH-L1), axonal (i.e., tau, p-tau-181, and NfL), or astroglial pathology (i.e., GFAP). Moreover, we found no differences in measures of plasma BDNF or salivary mRNA and telomere measures. Our results are consistent with Major and colleagues, in which no association was found between remote history of concussion and serum biomarker levels (i.e., GFAP, UCH-L1, NfL, tau, and p-tau-181) in younger adult amateur Australian football players.^19^ Similarly, Swann and colleagues recently found no elevation in plasma GFAP, NfL, and tau in former athletes with an extensive history of concussion.^20^ However, our previous studies have demonstrated some significant findings regarding young adult Australian football players. Specifically, we observed elevated serum protein levels of tau and p-tau, as well as shorter telomere length, in comparison to non-collision sport controls.^16^ Further, we have previously found that male players with a history of concussion exhibited higher levels of serum IL-1 compared with male players without a concussion history, and a positive correlation between IL-18 levels and the number of years of collision sport participation.^10^
Although the sample size in the current study is relatively small, and biomarkers, biofluid type, and platforms used to analyze are not identical to the previous studies, the preliminary findings suggest a lack of biomarker changes in Masters Australian football players with an extensive history of collision sport participation.
Aside from athlete age and biomarker differences, there may be other notable distinctions between the current cohorts of Masters studies and previous research conducted on younger Australian football players participating in “Senior” adult football. First, Senior male football players in the aforementioned studies reported more recent concussion exposure (median ∼2.5 years) compared to the Masters collision sport athletes in this study (6 years). Second, there are some differences in the way in which Australian football is played between the young adult and Masters competitions, with a “stronger emphasis on eliminating all forms of rough contact” in Masters football.^21^ Player movement (e.g., speed) and behavioral attitudes (e.g., aggression) are likely different between levels, potentially influencing the magnitude and frequency of TBIs.^22^ Third, Masters football is played less frequently (i.e., fortnightly) than Senior football (weekly). Considered together, TBI exposure is likely reduced in Masters Australian football and may explain some discrepancies in findings to that in younger players.
Although Masters Australian football may involve reduced impact exposure compared to Senior football played by younger adults, it is worth noting that the majority of the current cohort also had a significant history of participation in this form of the game earlier in life. Comparable levels of well-studied plasma biomarkers, such as GFAP, NfL, and p-tau-181, between collision sports athletes and non-collision controls,^20^ as well as their consistency with existing literature on healthy adults,^23–25^ likely indicate a lack of significant active neurodegeneration in these athletes. However, it is important to recognize that fluid biomarkers provide an indirect “snapshot” of current neurodegeneration, and advanced neuroimaging techniques, such as diffusion tensor imaging, can offer direct indications of compromised microstructural integrity resulting from past damage or degeneration. Future studies should explore potential variations in brain microstructure between different cohorts of collision sport athletes and non-collision controls. Additionally, longitudinal biomarker evaluation and cognitive testing may yield valuable insights into the potential effects of extended collision sports participation.
In conclusion, this study presents preliminary evidence suggesting that a panel of fluid biomarkers associated with brain damage, neurodegeneration, and inflammation may not exhibit significant elevation in active older Australian football Masters athletes who have a history of extensive and ongoing participation in collision sports.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Orchard J, Seward H, Orchard MJ. 2012 AFL injury report. Australian Football League: Docklands, Australia; 2013.
- 2Bernick C, Hansen T, Ng W, et al. Concussion occurrence and recognition in professional boxing and MMA matches: toward a concussion protocol in combat sports. Phys Sportsmed 2021;49(4):469–475; doi: 10.1080/00913847.2020.185663133251911 · doi ↗ · pubmed ↗
- 3Rueda MAF, Halley WL, Gilchrist MD. Fall and injury incidence rates of jockeys while racing in Ireland, France and Britain. Injury 2010;41(5):533–539; doi: 10.1016/j.injury.2009.05.00919524903 · doi ↗ · pubmed ↗
- 4Casson IR, Viano DC, Powell JW, et al. Twelve years of National Football League concussion data. Sports Health 2010;2(6):471–483; doi: 10.1177/194173811038396323015977 PMC 3438866 · doi ↗ · pubmed ↗
- 5Manley G, Gardner AJ, Schneider KJ, et al. A systematic review of potential long-term effects of sport-related concussion. Br J Sports Med 2017;51(12):969–977; doi: 10.1136/bjsports-2017-09779128455362 PMC 5466926 · doi ↗ · pubmed ↗
- 6Zetterberg H, Blennow K. Fluid biomarkers for mild traumatic brain injury and related conditions. Nat Rev Neurol 2016;12(10):563–574; doi: 10.1038/nrneurol.2016.12727632903 · doi ↗ · pubmed ↗
- 7Mc Crea M, Broglio SP, Mc Allister TW, et al. Association of blood biomarkers with acute sport-related concussion in collegiate athletes: findings from the NCAA and Department of Defense CARE Consortium. JAMA Netw Open 2020;3(1):e 1919771; doi: 10.1001/jamanetworkopen.2019.1977131977061 PMC 6991302 · doi ↗ · pubmed ↗
- 8Mc Donald SJ, O'Brien WT, Symons GF, et al. Prolonged elevation of serum neurofilament light after concussion in male Australian football players. Biomark Res 2021;9(1):4; doi: 10.1186/s 40364-020-00256-733422120 PMC 7797141 · doi ↗ · pubmed ↗