Heart transplantation in a patient with infective endocarditis bridged with Impella 5.5: a case report
Nadeem A Khan, Bassam Shukrullah, Peter M Eckman, Katarzyna M Hryniewicz

TL;DR
A patient with heart failure and infective endocarditis was stabilized with Impella 5.5 before heart transplant, showing a novel bridging strategy.
Contribution
Demonstrates the use of Impella as a bridge to heart transplant in septic patients with endocarditis.
Findings
Impella 5.5 stabilized a patient with heart failure and endocarditis before heart transplant.
The patient recovered from endocarditis and underwent successful heart transplant after three weeks.
MCS with Impella enabled infection control and stabilization prior to transplantation.
Abstract
Infective endocarditis (IE) is a feared complication after surgical valve replacement accounting for 10% to 30% of all cases of IE. Our case is unique as we present a decompensated heart failure patient with IE who urgently needed mechanical circulatory support (MCS) to stabilize while IE was treated. We used Impella to bridge him to sterile state before heart transplant was done. This case highlights the importance of different strategies for bridge to heart transplant in decompensated heart failure patients with endocarditis. We describe a case of 62-year-old male who initially presented with severe shortness of breath with minimal exertion, weight gain, and lower extremity oedema diagnosed with acute on chronic systolic heart failure (HF) exacerbation (ACC stage D, NYHA class IV). Initial blood cultures and extensive work-up for IE were negative. He continued to decompensate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
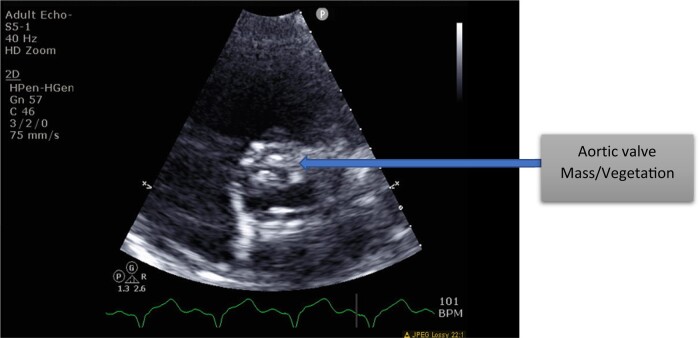 Figure 1
Figure 1 Figure 2
Figure 2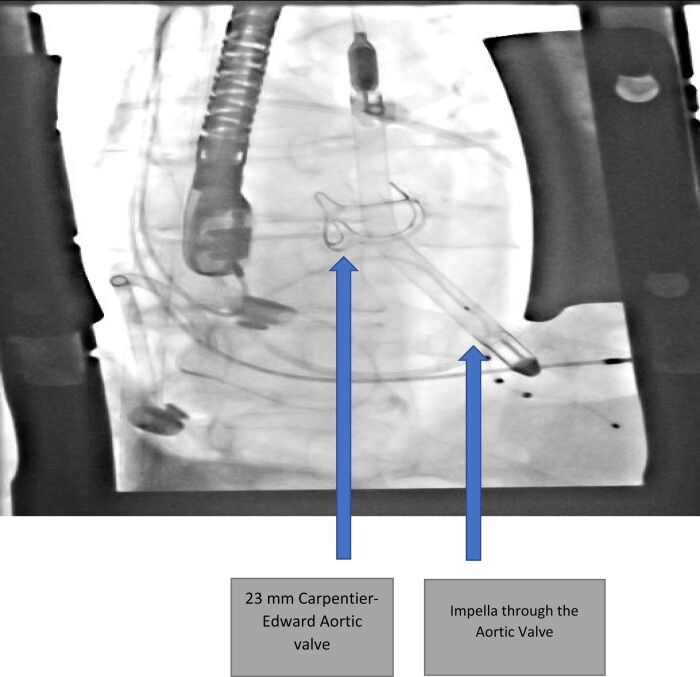 Figure 3
Figure 3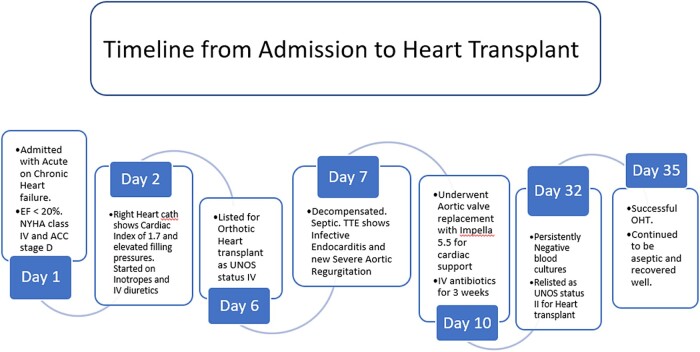 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Structural Anomalies and Repair · Mechanical Circulatory Support Devices
Introduction
Infective endocarditis (IE) causes significant complications after valve replacement, ranging from valvular dehiscence, abscess, mycotic aneurysms, complete heart block, stroke, or perforations.^1,2^ Incidence of IE has increased with increasing number of valve replacements.^3,4^ It is associated with high mortality and morbidity and it ranks as the fourth most common life-threatening infection syndrome after sepsis, pneumonia, and intra-abdominal abscess.^5^
Patients with severe progressive cardiomyopathy who develop IE have limited options for advanced therapies due to risk of bacterial seeding on a left ventricular assist device (LVAD) and risk of fulminant infection in a setting of immunosuppression after heart transplantation.
We present a case of aortic valve replacement (AVR) for IE and successful bridge to heart transplantation with temporary mechanical circulatory support (MCS; Impella 5.5) that allowed for the treatment of infection as well as overall improvement in patient’s clinical condition. Our case provides additional options for clinicians when faced with limited options in managing decompensated heart failure patients with active infection, who are currently waiting for LVAD or orthotopic heart transplantation (OHT).
Case report
This is a 62-year-old male with history of dilated bi-ventricular non-ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) of 19%, right ventricular EF of 31%, left ventricular end diastolic dimension of 7.5 cm, bicuspid aortic valve complicated by endocarditis, status post-mechanical AVR 15 years ago and bioprosthetic AVR 5 years ago, permanent pacemaker placement for complete heart block 3 years ago, and right middle cerebral artery stroke. He was recently found to have a left bundle branch block and underwent cardiac resynchronization therapy-defibrillator upgrade. A follow-up cardiac MRI revealed advanced non-ischaemic dilated cardiomyopathy without infiltrative disease. He was continued on aggressive guideline-directed medical therapy for advanced heart failure (HF).
He was admitted with progressive shortness of breath with minimal exertion, lower extremity oedema, weight gain, fatigue, and weakness. He was diagnosed with acute on chronic systolic HF exacerbation. Patient denied fever or chills. Transthoracic echocardiogram revealed EF of <20% with bi-ventricular enlargement; no valvular abnormalities were noted. Initial laboratory values were within normal limits except leucocytosis of 14.7 (4.5–11.0 × 10^9^/L), transaminitis with AST of 486 (8–33 U/L), ALT of 686 (7–56 U/L), troponin 0.214 (0.0–0.04 ng/mL), brain natriuretic peptide (BNP) 3115 (normal < 100 pg/mL), and C-reactive protein of 15 (normal < 0.5 mg/dL). Patient was borderline hypotensive and right heart catheterization demonstrated right atrial pressures of 18 mmHg, pulmonary artery pressures of 58/29/39 mmHg, and pulmonary capillary wedge pressure of 28 mmHg, with estimated Fick cardiac index of 1.7. He was found to be in cardiogenic shock with Forrester classification IV with cold and wet physiology. He was admitted to Intensive Care for inotropic support and i.v. diuresis.
He was in American College of Cardiology (ACC) stage D and New York Heart Association (NYHA) class IV. We initiated evaluation for advanced heart failure therapies and the patient was listed for heart transplantation as United Network for Organ Sharing (UNOS) status 4.^6,7^ On Day 2 after listing, he decompensated further and became febrile. A repeat echocardiogram revealed a large (1.3 × 1.1 cm) echodensity on the bioprosthetic aortic valve (see Figure 1) and severe aortic insufficiency (AI). Blood cultures grew Cutibacterium acnes. He was started on vancomycin and ceftriaxone and his UNOS status was deactivated to status 7. He was in cardiogenic and septic shock requiring inotropes and vasopressors. Temporary MCS options were limited due to his severe AI and active endocarditis precluded him from intra-aortic balloon pump (IABP), veno-arterial extracorporeal membrane oxygenation (VA-ECMO), or Impella placement. Despite high Society of Thoracic Surgery (STS) risk, we proceeded with urgent AVR. At the time of surgery, the patient was found to have large vegetation on the two leaflets of the bioprosthetic aortic valve (Figure 2). His root was debrided for all visible foreign material and a 23 mm Carpentier-Edwards Perimount Magna Ease bioprosthetic aortic valve was placed followed by Impella 5.5 via right subclavian artery cutdown. Impella was necessary due to patient’s persistent cardiogenic shock with inability to wean off of cardiac bypass despite being on maximal inotropic and vasopressor support. Impella 5.5 via subclavian access was chosen over IABP/VA-ECMO as it enabled early mobilization of the patient. Patient was extubated and mobilized within 24 h from surgery. He was continued on i.v. antibiotics for a total of 3 weeks.^8^ Tissue cultures of aortic valve were consistent with blood cultures of C. acnes. His repeat blood cultures were persistently negative and he was deemed sterile prior to being reactivated on the heart transplant list as UNOS status 2.^9^ He underwent successful OHT within a week from relisting (Figures 3 and 4).
Aortic valve mass; diagnosed on endocarditis.
Surgical specimen of the aortic valve mass. Prosthetic aortic valve with significant vegetations noted.
Post-operative image showing Impella through a newly placed 23 mm Carpentier-Edwards aortic valve.
Timeline of the events from admission to heart transplant.
He was initiated on our institutional approved immunosuppression protocol. For pre-induction, he received mycophenolate and methylprednisolone followed by tacrolimus, mycophenolate, and prednisone for maintenance. He did not receive any antibody induction with basiliximab or thymoglobulin. He did not develop any recurrent infections and progressed well post-OHT. He was discharged from hospital in 2 weeks. Post-OHT work-up remained negative for infection or rejection. He has recovered completely from the multiple surgeries and continues to enjoy good health as noted at his 6- and 12-month OHT follow-up visit.
Discussion
Infective endocarditis in prosthetic valve remains challenging despite advancements in diagnostic and treatment modalities. It has a worse prognosis if patient is in cardiogenic shock. Timing of procedures is crucial and requires an experienced team including an advanced heart failure cardiologist, cardiothoracic surgeon, interventional cardiologist, and an infectious disease specialist.
Our case reports a challenging clinical scenario of a patient with severely advanced cardiomyopathy and concomitant IE. The use of urgent valve replacement combined with temporary mechanical support to allow clearing of infection but at the same time providing adequate haemodynamic support, early extubation, mobilization, and nutrition seems to be a reasonable option in this patient population.
Supplementary Material
ytae062_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Olsen NT, De Backer O, Thyregod HGH, Vejlstrup N, Bundgaard H, Sondergaard L, et al Prosthetic valve endocarditis after transcatheter aortic valve implantation. Circ Cardiovasc Interv 2015;8:e 001939.25873728 10.1161/CIRCINTERVENTIONS.114.001939 · doi ↗ · pubmed ↗
- 2Alexis SL, Malik AH, George I, Hahn RT, Khalique OL, Seetharam K, et al Infective endocarditis after surgical and transcatheter aortic valve replacement: a state of the art review. J Am Heart Assoc 2020;9:e 017347.32772772 10.1161/JAHA.120.017347 PMC 7660802 · doi ↗ · pubmed ↗
- 3Petersson GB, Hussain ST. Surgical treatment of aortic valve endocarditis. In: Cohn LH and Adams DH (eds.), Cardiac surgery in the adult. 5th ed. New York: Mc Graw Hill Education; 2018. p 731–741.
- 4Amat-Santos IJ, Messika-Zeitoun D, Eltchaninoff H, Kapadia S, Lerakis S, Cheema AN, et al Infective endocarditis after transcatheter aortic valve implantation: results from a large multicenter registry. Circulation 2015;131:1566–1574.25753535 10.1161/CIRCULATIONAHA.114.014089 · doi ↗ · pubmed ↗
- 5Baddour LM, Wilson WR, Bayer AS, Fowler VG, Tleyjah IM, Rybak MJ, et al Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 2015;132:1435–1486.26373316 10.1161/CIR.0000000000000296 · doi ↗ · pubmed ↗
- 6OPTN/UNOS policy notice clarification to the adult heart allocation system policy language. Organ Procurement and Transplantation Network Policy and Organ Allocation guidelines. December 2016. optn.transplant.hrsa.gov.
- 7Mehra MR, Kobashigawa J, Starling R, Russell S, Uber PA, Parameshwar J, et al Listing criteria for heart transplantation: International Society for Heart and Lung Transplantation guidelines for the care of cardiac transplant candidates—2006. J Heart Lung Transplant 2006;25:1024–1042.16962464 10.1016/j.healun.2006.06.008 · doi ↗ · pubmed ↗
- 8Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al 2015 ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015;36:30753128.10.1093/eurheartj/ehv 31926320109 · doi ↗ · pubmed ↗