Birth by caesarean section and semen quality in adulthood: a Danish population-based cohort study
Kun Huang, Anne Gaml-Sørensen, Nis Brix, Andreas Ernst, Linn Håkonsen Arendt, Jens Peter Ellekilde Bonde, Karin Sørig Hougaard, Gunnar Toft, Sandra Søgaard Tøttenborg, Cecilia Høst Ramlau-Hansen

TL;DR
This study found no significant negative effects of caesarean section on adult sons' semen quality in a large Danish cohort.
Contribution
This is the first population-based study to examine the association between caesarean section and semen quality in adulthood.
Findings
Sons born by caesarean section had slightly higher progressive sperm motility compared to those born vaginally.
No significant differences were found in semen volume, sperm concentration, or morphology between delivery modes.
No adverse effects of caesarean section on overall semen quality were observed in this large cohort.
Abstract
The caesarean section (CS) rate has increased worldwide and there is an increasing public and scientific interest in the potential long-term health consequences for the offspring. CS is related to persistent aberrant microbiota colonization in the offspring, which may negatively interfere with sex hormone homeostasis and thus potentially affect the reproductive health. It remains unknown whether adult sons’ semen quality is affected by CS. We hypothesize that CS is associated with lower semen quality. This study was based on the Fetal Programming of Semen Quality cohort (FEPOS, enrolled from 2017 to 2019) nested within the Danish National Birth Cohort (DNBC, enrolled from 1996 to 2002). A total of 5697 adult sons of mothers from the DNBC were invited to the FEPOS cohort, and 1044 young men participated in this study. Information on mode of delivery was extracted from the Danish Medical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
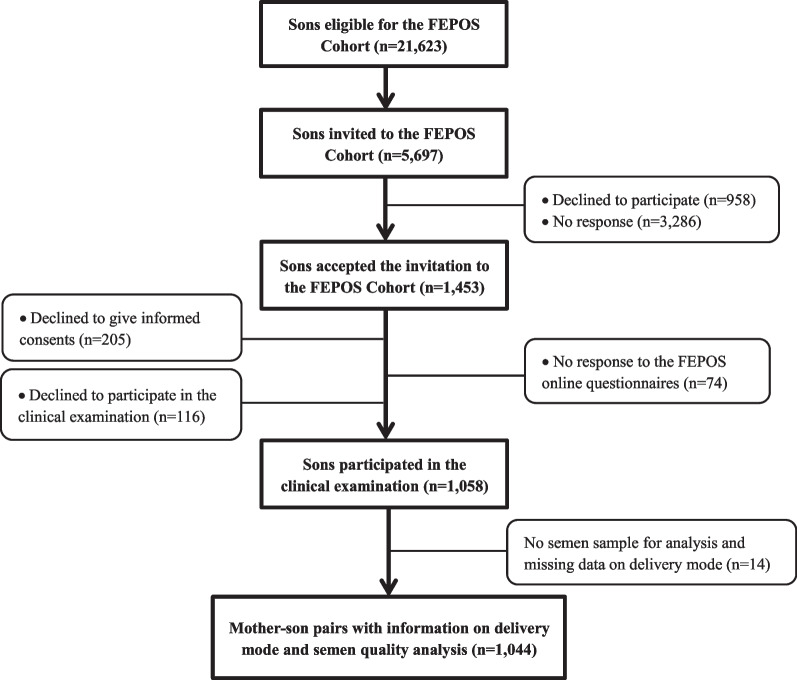 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Assisted Reproductive Technology and Twin Pregnancy · Reproductive Health and Contraception
Introduction
Worldwide, the caesarean section (CS) rate has almost doubled from 12% of all births in 2012 to 21% in 2015 [1] with large geographical differences. According to the World Health Organization, 6.2 million CSs are performed yearly without medical indication [2]. Understanding the long-term effects of CS on child health is important for guiding decision making for clinicians, policy makers and the parents. Potential consequences for the children’s respiratory, metabolic, cardiovascular and immune function affected by CS are described [3]. However, it remains unclear whether also the reproductive health of children is affected by CS.
There is scientific and public concern about the state of male reproductive health in Western countries [4]. Poor semen quality is a major cause of infertility [5], which affects psychosocial well-being of couples worldwide [6] and has major consequences for society, due to cost of treatment, absenteeism from work and, most importantly, lower birth rates [7, 8]. Whether mode of delivery impacts semen quality remains to be investigated. It has been indicated that infants born by CS may be colonized by aberrant microbiota [9–11] that may persist into adulthood [12]. Gut microbiota dysbiosis has been suggested to negatively modulate gonadal sex hormones production and regulation and thus potentially decrease reproductive fitness [13, 14]. In particular, it has been reported that gut microbiota in the infant born via elective CS was less rich and diverse than those born by emergency CS [15, 16], as may be due to “partial” microbial exposure during emergency CS following membrane rupture [15]. To the best of our knowledge, semen quality of sons delivered by CS has not previously been studied.
In this present population-based cohort study, we aimed to examine the potential association between birth by CS and the adult son’s semen quality, under the hypothesis that CS, in general, and elective CS, in particular, is associated with lower semen quality.
Materials and methods
Participants
This study is based on the Fetal Programming of Semen Quality (FEPOS) cohort [17], nested within the Danish National Birth Cohort (DNBC) [18]. In the DNBC, from 1996 to 2002, pregnant women were enrolled and interviewed by computer-assisted telephone interviews conducted around 16 and 30 weeks’ gestation, and at 6 months after childbirth.
The participants in the FEPOS cohort were recruited from March 2017 to December 2019. Recruitment to FEPOS is described in detail elsewhere [17]. In short, sons were eligible for invitation if their mothers responded to the first two telephone interviews during pregnancy in the DNBC and provided a gestational blood sample for the biobank within the DNBC. Invitation to the FEPOS cohort was further restricted to the following criteria: Son of at least 18 years and 9 months of age, living in close proximity to the FEPOS clinics in Copenhagen (the capital and largest city in Denmark) or Aarhus (the second largest city in Denmark). Sons were encouraged to decline participation if they had undergone sterilization, cancer treatment, orchidectomy, or had one or no testicles in the scrotum.
During the study period, 5697 of the 21,623 eligible young men were randomly invited to participate in FEPOS. Of these, 1174 (21%) responded to an online questionnaire on health behaviors, whereafter 1058 delivered a semen sample (participation rate 19%). After excluding sons with no semen sample and/or missing data on delivery mode, 1044 mother-son pairs (18%) were included in our main analysis (Fig. 1).Fig. 1. Flow chart of participants, the FEPOS Cohort, Denmark, 1998–2019
Delivery mode
Information on delivery mode was extracted from the Danish Medical Birth Registry (DMBR) [19, 20] based on ICD-10 diagnostic codes and procedure codes according to the Nordic Medico-Statistical Committee classification of surgical procedures. Delivery mode included vaginal delivery (ICD-10: DO800, DO801, DO808, DO809, DO810, DO813, DO814, DO815, DO840, DO841), elective CS before labor (ICD-10: DO820 and operation codes KMCA10B or KMCA11), emergency CS during labor (ICD-10: DO821, DO842 and operation codes KMCA10D, KMCA10E) and unspecified CS (ICD-10: DO828, DO829 and operation codes KMCA10A). The latter three categories of CS (elective CS, emergency CS and unspecified CS) were merged into an overall CS exposure category in the main analysis due to low numbers in some of the separate categories.
Semen quality characteristics
Participants provided a semen sample for analysis either at the clinic or at home. If collected at home, participants were recommended to keep the sample warm during transportation to the clinic and deliver the sample within one hour of ejaculation. Recommended abstinence time was 2–3 days.
Collection and analysis of semen followed recommendations by the WHO 2010 [21]. Analysis was conducted by two trained biomedical laboratory technicians and started within a maximum of two hours from ejaculation in 1029 out of 1044 semen samples (99%). In total, 786 (75%) semen samples were analyzed within one hour. Semen volume was measured by weighing of the sample in a pre-weighed container assuming 1 g = 1 ml. After liquefaction at 37 °C, sperm concentration was determined on two aliquots of semen using an Improved Neubauer Hemocytometer. Total sperm count was calculated by multiplication of semen volume and concentration. Sperm motility was determined by assessing progressive, non-progressive and immotile spermatozoa for at least 200 spermatozoa within each of two fresh drops of semen. The outcome used in the study was progressive motility, which, to ensure optimal model fit, was assessed as non-progressive motility modeled as non-progressive + immotile spermatozoa in percentage. Morphology was analyzed at the Reproductive Medicine Centre, Skåne University Hospital, in Malmö, Sweden. The percentage of normal spermatozoa was assessed in approximately 200 spermatozoa per slide.
External quality control with the European Society of Human Reproduction and Embryology (ESHRE) External Quality Assessment scheme (Centre for Andrology, Karolinska University Hospital, Stockholm, Sweden) indicated no distinct differences between the FEPOS laboratory technologists and the expert reference examiners [17].
Covariates
Potential confounders were identified a priori using existing literature and Directed Acyclic Graphs (DAGs) [22] (Additional file 1: Appendix S1). Maternal age at delivery was retrieved from DMBR. Information on maternal smoking in the first trimester, pre-pregnancy body mass index (BMI) and highest socioeconomic status of the parents was provided by the mothers in the first DNBC interview. Socioeconomic status was defined according to the International Standard Class of Occupation and Education codes (ISCO-88 and ISCED). Categorization of the covariates was presented in Table 1.Table 1. Baseline characteristics by delivery mode, N = 1044, the FEPOS cohort, Denmark, 1998–2019Background characteristicsDelivery modeMissingn (%)Vaginal delivery(n = 912)CS(n = 132)Maternal characteristics Maternal age at delivery, years, mean ± SD30.9 ± 0.131.4 ± 0.30 (0.0) Highest socioeconomic status of parents, n (%)0 (0.0) High-grade professional307 (33.7)50 (37.9) Low-grade professional307 (33.7)40 (30.3) Skilled worker171 (18.8)25 (18.9) Unskilled worker84 (9.2)11 (8.3) Student, economically inactive and un-definable43 (4.7)6 (4.6)Pre-pregnancy BMI, kg/m^2^, n (%)25 (2.4) < 18.555 (6.2)6 (4.7) 18.5–24.9663 (74.4)85 (66.4) 25.0–29.9136 (15.3)27 (21.1) ≥ 30.037 (4.2)10 (7.8)Smoking in the 1st trimester, n (%)< 15 (< 1.4)^b^ Nonsmoker702 (77.7)101 (78.9) 1–10 daily cigarettes171 (18.9)< 25 (< 18.9)^b^ > 10 daily cigarettes31 (3.4)< 5 (< 3.8)^b^Pregnancy complications, n (%)^a^0 (0.0) None860 (94.3)120 (90.9) One or more52 (5.7)12 (9.1)Son’s characteristics Gestational week at delivery, mean ± SD39.8 ± 1.539.3 ± 2.10 (0.0) Birth weight, kg, mean ± SD3.7 ± 0.53.6 ± 0.712 (1.1)Semen-related characteristics Place of semen sample delivery, n (%)6 (0.6) At home125 (13.7)13 (9.9) In the clinic781 (85.6)119 (90.2) Abstinence time, days, mean ± SD2.3 ± 0.02.4 ± 0.1< 5 (< 0.5)^b^ Interval from ejaculation to analysis, minutes, mean ± SD49.9 ± 0.750.2 ± 1.68 (0.8)Spillage of semen sample, n (%)5 (0.5) No747 (82.3)112 (85.5) Yes161 (17.7)19 (14.5)SD standard deviationBody mass index (BMI) = weight(kg)/height(m)^2^^a^Pregnancy complications defined as women reporting one or more of the following conditions: diabetes mellitus (type 1, type 2 or gestational diabetes), hypertension and preeclampsia^b^Due to data regulations that numbers less than five are not allowed to report, the numbers in the table have been changed or combined to cover up the numbers less than five
Information on precision variables was recorded at the clinical visit, including place of semen sample collection (at home or in the clinic), abstinence time (in days), spillage of semen sample (no; yes), and interval from ejaculation to analysis (in minutes).
Information on pregnancy complications, labor induction, gestational age at birth (in weeks) and birth weight (in grams) were used in sensitivity analyses. Pregnancy complications were self-reported in the women’s interview around 16 and 30 weeks of gestation and 6 months after childbirth and included diabetes mellitus (type 1, type 2 or gestational diabetes), hypertension and preeclampsia. Women, who reported one or several of these conditions, were defined as having pregnancy complications (none; one or more). Information on gestational age at birth, birth weight, and labor induction (pharmaceutical or non-pharmaceutical based on ICD diagnose codes DO837 and DO847 and procedure codes KMAC00, KMAC96A, BKHD20, BKHD20A and BKHD 21) were obtained from DMBR.
Statistical analysis
Data management and statistical analyses were conducted with STATA MP, version 15.1 (StataCorp, College Station, TX). According to the requirements of regulations [GDPR, Regulation (EU), 2016/679 of 25 May 2018)], a calculated percentile must be based on at least five observations. Thus, pseudo percentile 5, 50 (median), and 95 for the semen characteristics were calculated by delivery mode using STATA’s -sumat- commands.
As the distributions of the semen characteristics were over-dispersed, we applied negative binomial regression models to examine the association between CS and semen characteristics using STATA’s -nbreg- package. We estimated crude and adjusted relative differences in percentages with 95% confidence intervals (CIs) for each semen characteristics by comparing sons born by CS to those born by vaginal delivery.
Azoospermic men were excluded from analyses of motility and morphology (n = 17), and participants reporting spillage of the semen sample were excluded from analyses of semen volume and total sperm count (n = 180). All models were adjusted for abovementioned selected confounders, place of semen sample collection and abstinence time. The analysis of sperm concentration and morphology was further adjusted for spillage, and the analysis of motility was further adjusted for interval from ejaculation as sperm motility decreases with time [23].
We applied selection weights to all analyses to account for non-participation [24]. These were estimated as the inverse probability of participation derived from a multivariable logistic regression with participation status (yes; no) as the dependent variable and the primary exposure variable (delivery mode) and the potential confounding factors, in addition to region (Aarhus; Copenhagen), parental time to pregnancy (TTP) including use of medically assisted reproduction (MAR), included as explanatory variables. TTP and MAR were considered indicators of parental fertility, and these data were obtained in the first interview in the DNBC.
Assumptions were checked for each model. We compared the observed distribution of each semen characteristic against the model-based distributions from the fitted model using QQ-plots. Furthermore, the standardized deviance residuals were plotted against the model-based predictions. The model check was compatible with the assumptions (data not shown).
We performed three sensitivity analyses to assess confounding by indication. First, we further adjusted for birth weight z-scores [25] as being small or large for gestational age might be an important indicator for CS, and birth weight for gestational age has been reported to be associated with semen quality [26, 27]. Birth weight z-score was not included in the main analyses due to the risk of collider-stratification bias [28, 29]. Second, we restricted our analyses to women without induction of labor and pregnancy complications. Labor induction has been suggested by some researchers as an independent risk factor for CS [30, 31], and the indications for induction may be the same as for CS. In addition, severe pregnancy complications might be a potential medical indicator for CS. Third, CS was further classified into elective CS, emergency CS and unspecified CS, with vaginally-born sons as reference, to examine whether the type of CS was important for semen quality.
Results
Among the 1044 sons included, 132 (13%) were born by CS. Mothers giving birth by CS were on average older, had higher pre-pregnancy BMI and experienced more pregnancy complications than mothers giving birth vaginally (Table 1).
Overall, sons born by CS had similar median values for the assessed semen characteristics compared to sons born vaginally (Table 2).Table 2. Semen characteristics ^a^ by delivery mode, the FEPOS cohort, Denmark, 1998–2019Semen parametersNumber of observationsVaginal deliveryCesarean sectionP_5_MedianP_95_P_5_MedianP_95_Semen volume, mL^b^8581.02.75.41.02.95.9Total sperm count, million^b^8587.6101.2413.68.8105.7398.1Sperm concentration, million/mL10422.837.9136.51.541.3149.3Progressive sperm motility, %^c^102529.263.083.235.465.582.8Morphologically normal sperm, %^c^10200.56.015.00.16.014.5^a^Pseudo percentiles were presented and were calculated based on the average of five values^b^180 samples were excluded due to spillage^c^Progressive motility and morphology were not available for 17 samples due to azoospermia
In the main analysis, we found a slightly lower percentage of non-progressive sperm motility (reflecting higher percentage of progressive sperm motility) for sons born by CS than for sons born vaginally [relative difference (95% CI): − 7.5% (− 14.1% to − 0.4%)]. No differences were observed for other sperm characteristics (Table 3).Table 3. Relative differences in percentage in semen characteristics by delivery mode, the FEPOS cohort, Denmark, 1998–2019Semen parametersNumber of observations^a^Relative differences in percentage ^b^Unadjusted modelAdjusted model%% (95% CI)Semen volume^f^8185.6 (− 6.8 to 18.5)5.3 (− 5.3 to 17.1)^c^Total sperm count^f^8180.9 (− 17.4 to 22.3)− 0.8 (− 14.9 to 15.8)^c^Sperm concentration9885.4 (− 11.7 to 24.2)4.3 (− 11.2 to 22.5)^d^Non-progressive motility^gh^965− 6.0 (− 13.8 to 1.3)− 7.5 (− 14.1 to − 0.4)^e^Morphologically normal sperm^g^9662.0 (− 11.5 to 17.4)− 2.0 (− 14.2 to 11.8)^d^^a^Number of observations in adjusted model for each parameters^b^Relative percentage differences were obtained using sons born of vaginal delivery as the reference^c^Adjusted for maternal age at delivery, highest socioeconomic status of parents, maternal pre-pregnancy BMI, maternal smoking in the 1st trimester, place of semen sample collection, abstinence time^d^Further adjusted for spillage^e^Further adjusted for spillage and interval from ejaculation to analysis^f^180 samples were excluded for the analyses on semen volume and total sperm count due to spillage^g^For non-progressive motility and morphology, 17 samples were not available for analyses due to azoospermia^h^Non-progressive motility was modeled as (non-progressive + immotile spermatozoa) %, and a negative estimate indicated a relatively lower non-progressive motility (ie. higher progressive motility)
In the sensitivity analyses, with further adjustment for birth weight z-scores (model 1), or restriction to women without labor induction and pregnancy complications (model 2), the results did not change essentially. In model 3, when CS was further classified into elective CS, emergency CS and unspecified CS, no significant differences in non-progressive motility or any of the other semen characteristics were observed among sons born by any of the three types of CS compared to sons born vaginally (Table 4).Table 4. Sensitive analyses for relative differences in percentage in semen characteristics by delivery mode, the FEPOS cohort, Denmark, 1998–2019Semen parametersAnalysis strategiesNumber of observationsDelivery modeRelative differences in percentageUnadjusted modelAdjusted model ^a^%% (95% CI)Semen volume^b^Model 1^f^806Overall CS5.6 (− 6.8 to 18.5)5.4 (− 5.4 to 17.5)Model 2 g691Overall CS5.5 (− 7.0 to 19.7)5.2 (− 6.4 to 18.3)Model 3 h818Elective CS (n = 35)− 4.7 (− 21.8 to 16.0)− 2.4 (− 16.5 to 14.1)Emergency CS (n = 52)10.9 (− 4.8 to 29.2)10.1 (− 6.7 to 30.0)Unspecified CS (n = 17)11.1 (− 14.5 to 44.5)7.8 (− 9.9 to 29.0)Total sperm count^b^Model 1^f^806Overall CS0.9 (− 17.4 to 22.3)− 0.5 (− 14.8 to 16.1)Model 2 g691Overall CS− 0.4 (− 19.7 to 23.5)0.0 (− 15.9 to 19.0)Model 3 h818Elective CS (n = 35)− 20.0 (− 41.7 to 9.7)− 16.4 (− 36.7 to 10.5)Emergency CS (n = 52)6.0 (− 18.5 to 37.8)7.2 (− 12.0 to 31.0)Unspecified CS (n = 17)29.4 (− 17.7 to 103.3)9.5 (− 22.2 to 54.0)Sperm concentration^c^Model 1^f^975Overall CS5.4 (− 11.7 to 24.2)4.6 (− 11.2 to 23.3)Model 2 g828Overall CS3.9 (− 13.4 to 24.4)2.5 (− 14.0 to 22.3)Model 3 h988Elective CS (n = 41)− 7.9 (− 29.1 to 21.0)− 4.5 (− 27.6 to 26.0)Emergency CS (n = 60)13.1 (− 9.6 to 41.3)10.8 (− 11.3 to 38.5)Unspecified CS (n = 20)8.7 (− 26.4 to 60.4)4.1 (− 23.1 to 41.0)Non− progressive motility^de^Model 1^f^952Overall CS− 6.0 (− 13.8 to 1.3)− 7.3 (− 13.0 to 0.0)Model 2 g812Overall CS− 5.4 (− 12.1 to 2.6)− 6.8 (− 14.3 to 1.2)Model 3 h965Elective CS (n = 38)− 9.0 (− 19.8 to 3.2)− 10.8 (− 21.3 to 1.1)Emergency CS (n = 58)− 6.7 (− 15.8 to 3.3)− 7.4 (− 16.0 to 1.2)Unspecified CS (n = 20)1.9 (− 14.6 to 21.3)− 1.1 (− 16.8 to 17.9)Morphologically normal sperm^ce^Model 1^f^953Overall CS2.0 (− 11.5 to 17.4)− 2.1 (− 14.4 to 12.0)Model 2 g812Overall CS1.6 (− 12.8 to 18.3)− 2.0 (− 15.3 to 13.4)Model 3 h966Elective CS (n = 39)− 19.4 (− 36.7 to 2.7)− 20.4 (− 39.8 to 5.3)Emergency CS (n = 58)11.4 (− 7.8 to 34.6)5.6 (− 9.1 to 22.7)Unspecified CS (n = 20)15.4 (− 16.5 to 59.4)14.3 (− 11.9 to 48.4)CS caesarean section^a^Basic set of variables that were adjusted for all semen parameters included maternal age at delivery, highest socioeconomic status of parents, maternal pre-pregnancy BMI, maternal smoking in the 1st trimester, place of semen sample collection and abstinence time^b^For the analyses of semen volume and total sperm count, 180 samples were excluded due to spillage^c^For the analysis of sperm concentration and morphologically normal sperm, spillage was further adjusted for^d^Non-progressive motility was modeled as (non-progressive + immotile spermatozoa) %, and a negative estimate indicated a relatively lower non-progressive motility (ie. higher progressive motility). In the analysis, spillage and internal from ejaculation to analysis were further adjusted for^e^For non-progressive motility and morphology, 17 samples were not available for analyses due to azoospermia^f^Model 1: Birth weight z-scores were further adjusted for^g^Model 2: Restricted to women without labor induction and pregnancy complications^h^Model 3: CS was further classified into elective CS, emergency CS and unspecified CS, and percentage differences were obtained by comparing with the sons born of vaginal delivery
Discussion
To the best of our knowledge, this is the first study to examine the association between CS and semen quality in sons at adulthood. Overall, there was no significant evidence for an adverse effect of CS on semen quality.
There is no clear biological explanation for the slightly higher percentage of progressively motile spermatozoa among the young adults born by CS compared to sons born vaginally. Nevertheless, the effect size was small, and no associations were observed between CS and the other semen characteristics. Further, we did not observe associations when taking the different types of CS into account in sensitivity analysis. Therefore, the current result is likely a chance finding.
This study has several strengths. The FEPOS cohort is the largest population-based male offspring cohort worldwide with detailed and prospectively collected data on maternal health in pregnancy, including information on birth outcomes, which allowed for comprehensive confounding control and reduced the risk of recall bias. Besides the potential confounders, precision variables were adjusted for in the regression models to increase the statistical precision. As the prevalence of urogenital diseases was low in this population and are not suspected to affect the results, these diseases were not adjusted for in the analyses. Information on CS was prospectively registered, and data from the DMBR are considered valid [21] with high predictive values, although we cannot rule out some misclassification regarding the type of CS. Neither participants, nor the biomedical laboratory scientists conducting the semen quality analyses, were aware of the objective of the current study. Therefore, the risk of differential misclassification is limited.
Some limitations must be considered. The participation rate in FEPOS was 19%, which increases the risk of selection bias. However, we consider participation not to be related to CS (CS rate was 13% and 14% in participants and non-participants, respectively), and that self-selection into the cohort did not depend on semen quality. The sons were young and most would not yet be aware of their fertility status, which minimizes the risk of self-selection. However, sons from families with fertility problems could be more likely to participate. Therefore, we estimated selection weights, including parental time to pregnancy and MAR use, to take the potential selective participation into account. Further, in this study, we could not differentiate between indicators for elective CS. Medical indication for elective CS (e.g. preeclampsia) could interfere with the development of the male reproductive organs [32]. The DMBR have only registrations of elective CS on maternal request from late 2001 and onwards. We could therefore not differentiate between reasons for elective CS to examine if potential effects associated with CS could be attributed to the underlying medical conditions or the surgical procedure. We performed sensitivity analysis to assess confounding by indication by adjusting for birth weight for gestational age, excluding women with induction of labor and pregnancy complications and categorizing CS into elective, emergency and unspecified CS. Still, other sources of unmeasured confounding, in particular confounding by indication, cannot not be ruled out.
Conclusions
In summary, this large population-based cohort study found no significant evidence for an adverse effect on semen quality in adult sons born by CS.
Supplementary Information
Additional file 1: Appendix S1. DAG for CS and semen quality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boerma T Ronsmans C Melesse DY Barros AJD Barros FC Juan L Global epidemiology of use of and disparities in caesarean sections Lancet 20183921341134810.1016/S 0140-6736(18)31928-730322584 · doi ↗ · pubmed ↗
- 2Sandall J Tribe RM Avery L Mola G Visser GH Homer CS Short-term and long-term effects of caesarean section on the health of women and children Lancet 20183921349135710.1016/S 0140-6736(18)31930-530322585 · doi ↗ · pubmed ↗
- 3Skakkebaek NE Rajpert-De Meyts E Buck Louis GM Toppari J Andersson AM Eisenberg ML Male Reproductive Disorders and Fertility Trends: Influences of Environment and Genetic Susceptibility Physiol Rev 2016961559710.1152/physrev.00017.201526582516 PMC 4698396 · doi ↗ · pubmed ↗
- 4Levine HJørgensen N Martino-Andrade A Mendiola J Weksler-Derri D Mindlis I Temporal trends in sperm count: a systematic review and meta-regression analysis Hum Reprod Update 20172364665910.1093/humupd/dmx 02228981654 PMC 6455044 · doi ↗ · pubmed ↗
- 5Vander Borght M Wyns C Fertility and infertility: definition and epidemiology Clin Biochem 20186221010.1016/j.clinbiochem.2018.03.01229555319 · doi ↗ · pubmed ↗
- 6Baird DT Collins J Egozcue J Evers LH Gianaroli L Leridon H Fertility and ageing Hum Reprod Update 20051126127610.1093/humupd/dmi 00615831503 · doi ↗ · pubmed ↗
- 7Christiansen T Erb K Rizvanovic A Ziebe S Mikkelsen Englund AL Hald F Costs of medically assisted reproduction treatment at specialized fertility clinics in the Danish public health care system: results from a 5-year follow-up cohort study Acta Obstet Gynecol Scand 201493647210.1111/aogs.1229324266525 · doi ↗ · pubmed ↗
- 8Jakobsson HE Abrahamsson TR Jenmalm MC Harris K Quince C Jernberg C Decreased gut microbiota diversity, delayed Bacteroidetes colonisation and reduced Th 1 responses in infants delivered by caesarean section Gut 20146355956610.1136/gutjnl-2012-30324923926244 · doi ↗ · pubmed ↗