Physicians' Perspectives on the Impact of Insurance Status on Clinical Decision-Making in Saudi Arabia
Abdullah A Alotaibi, Khalid A Alotaibi, Ahmad N Almutairi, Anas Alsaab

TL;DR
This study explores how physicians in Saudi Arabia consider patients' insurance status when making clinical decisions and how this affects treatment options and outcomes.
Contribution
The study provides insights into how insurance status influences physicians' decision-making and patient outcomes in Saudi Arabia.
Findings
Most physicians consider insurance status when discussing treatment options.
Over 80% of physicians believe insurance status affects patient outcomes and treatment modalities.
Physician age, experience, and practice type significantly influence how insurance status impacts clinical decisions.
Abstract
Background The decision-making process in clinical practice depends heavily on collaboration and information sharing. Physicians' decision-making processes are profoundly influenced by the patient's insurance status, which warrants focused investigation. Hence, this study aimed to investigate how physicians perceive the influence of insurance status on treatment options and medical interventions and to explore the extent to which physicians discuss insurance-related considerations with patients during the shared decision-making process. Methodology This was a cross-sectional exploratory study conducted in various healthcare facilities all over Saudi Arabia. The electronic questionnaire was the primary tool for data collection. Data were then coded, entered, and analyzed using both descriptive and inferential statistical methods. Results The study involved 430 physicians, primarily…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
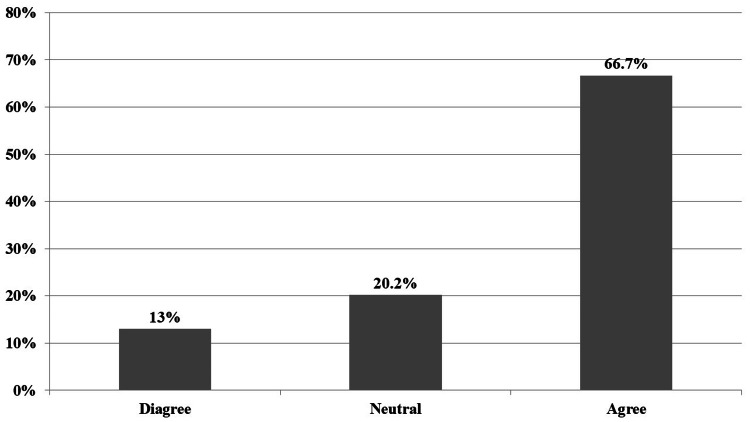 Figure 1
Figure 1| Variable | Categories | Frequency | Percentage (%) |
| Gender | Male | 230 | 53.5 |
| Female | 200 | 46.5 | |
| Age (in years) | 25-30 | 71 | 16.5 |
| 31-40 | 215 | 50 | |
| 41-59 | 116 | 27 | |
| 60 or more | 28 | 6.5 | |
| Nationality | Saudi | 145 | 33.7 |
| Non-Saudi | 285 | 66.3 | |
| Category | General practitioner | 115 | 26.7 |
| Registrar | 101 | 23.5 | |
| Senior registrar | 100 | 23.3 | |
| Consultant | 114 | 26.5 | |
| Specialty | Dentist | 71 | 16.5 |
| Medical | 258 | 60 | |
| Surgical | 101 | 23.5 | |
| Years of experience | Less than one year | 15 | 3.5 |
| 1-5 years | 187 | 43.5 | |
| 6-10 years | 156 | 36.3 | |
| More than 10 years | 72 | 16.7 | |
| Type of practice | Private-only | 301 | 70 |
| Both (Government/Private) | 129 | 30 |
| Statement | Disagree, | Neutral, | Agree, |
| 1. I take into consideration a patient's insurance status when discussing potential treatment options. | 56 (13) | 87 (20.2) | 287 (66.7) |
| 2. I ensure that my patients are aware of how their insurance status might impact the range of treatment options available to them. | 14 (3.3) | 99 (23) | 317 (73.7) |
| 3. I discuss the financial implications of different treatment options with patients, considering their insurance coverage. | 0 (0) | 112 (26) | 318 (74) |
| 4. I have observed differences in the treatment choices made by patients based on their insurance status. | 0 (0) | 99 (23) | 331 (77) |
| 5. Insurance-related considerations influence the time taken by patients to receive necessary medical interventions. | 42 (9.8) | 100 (23.3) | 288 (67) |
| 6. I believe that insurance status can impact patient outcomes and treatment effectiveness. | 28 (6.5) | 29 (6.7) | 373 (86.7) |
| 7. Insurance-related factors play a role in the shared decision-making process between me and my patients. | 0 (0) | 156 (36.3) | 274 (63.7) |
| 8. I feel that patients with different insurance statuses receive equitable medical care. | 29 (6.7) | 141 (32.8) | 260 (60.5) |
| 9. I believe that addressing insurance-related disparities in healthcare is essential for improving patient outcomes. | 28 (6.5) | 84 (19.5) | 318 (74) |
| Variable | Categories | Score of insurance status Impacts on clinical decision-making |
| |
| Mean | SD | |||
| Gender | Male | 23.85 | 3.684 | 0.381 |
| Female | 24.12 | 2.555 | ||
| Age (in years) | 25-30 | 23.00 | 3.740 | <0.001 |
| 31-40 | 25.38 | 2.113 | ||
| 41-59 | 24.83 | 2.242 | ||
| 60 or more | 23.50 | 1.528 | ||
| Nationality | Saudi | 24.06 | 2.852 | 0.710 |
| Non-Saudi | 23.93 | 3.379 | ||
| Category | General practitioner | 24.16 | 2.664 | 0.382 |
| Registrar | 24.33 | 2.367 | ||
| Senior registrar | 23.75 | 2.717 | ||
| Consultant | 23.68 | 4.495 | ||
| Specialty | Dentist | 24.24 | 2.659 | 0.005 |
| Medical | 24.26 | 3.402 | ||
| Surgical | 23.07 | 2.892 | ||
| Years of experience | Less than 1 year | 25.00 | 0.000 | 0.002 |
| 1-5 years | 23.43 | 3.521 | ||
| 6-10 years | 24.04 | 3.364 | ||
| More than 10 years | 25.04 | 1.682 | ||
| Type of practice | Private only | 23.76 | 3.528 | 0.012 |
| Both (Government/Private) | 24.47 | 2.226 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Malpractice and Liability Issues · Patient-Provider Communication in Healthcare · Healthcare Policy and Management
Introduction
Clinical decision-making is a collaborative process that hinges on the exchange of information [1]. In this process, healthcare providers disseminate the advantages and drawbacks of various treatment possibilities, while patients contribute their personal values and lifestyle choices. This amalgamation of data facilitates decisions grounded in the most relevant evidence, tailored to individual preferences and requirements. The crux of decision-making arises when several medically viable alternatives are at hand, with no universally optimal solution.
The contemporary landscape of healthcare systems is marked by a dynamic interplay between clinical decision-making and an array of external factors that collectively shape patient care [2]. Among these, influential factors, the patient’s insurance status has risen to prominence, warranting focused investigation into its impact on the decision-making processes of the physicians [3].
Particularly within the context of Saudi Arabia, a country undergoing rapid advancements in healthcare, the intricate relationship between insurance status and clinical decision-making has emerged as a subject of paramount importance [4]. This research embarks on a comprehensive exploration, aiming to unravel the nuanced layers of physicians’ perceptions concerning how insurance status intricately influences their clinical decision-making practices within the intricate tapestry of the Saudi Arabian healthcare landscape.
This study posits that the interface between insurance status and clinical decision-making is an intricate and multifaceted domain that extends far beyond monetary considerations. It signifies a juncture where the art and science of medicine converge with socioeconomic dynamics, ethical considerations, and patient-centered care. The choices physicians make, guided by their perceptions and insights, hold the potential to be influenced by a patient’s insurance status, thereby shaping the trajectory of medical interventions, diagnostic pathways, and treatment modalities [5]. Specifically, it seeks to comprehend the intricate ways in which insurance status reverberates through the corridors of clinical decision-making in Saudi Arabia’s intricate healthcare.
As Saudi Arabia forges ahead in its mission to elevate its healthcare ecosystem, the insights derived from this research hold significant implications. A comprehensive grasp of physicians’ perceptions regarding the intricate interplay between insurance status and clinical decision-making could illuminate potential areas of improvement in patient care, resource allocation, and policy formulation [3]. The findings can catalyze informed dialogues among stakeholders, fostering a healthcare system that is not only technologically advanced but also deeply attuned to the diverse needs and dynamics of its patient population.
The nexus between insurance status and clinical decision-making has garnered substantial global attention within the healthcare discourse in recent years. The research by Riley has underscored the formidable challenges that uninsured patients often encounter in accessing comprehensive medical care, exacerbating pre-existing disparities within healthcare systems [6]. This observation has illuminated the profound implications of insurance status, reaching far beyond financial implications, and reinforcing the need for equitable healthcare access.
Interestingly, within the context of Saudi Arabia, a parallel perspective has remained relatively underexplored. Al-Hanawi et al. ventured into this uncharted territory, revealing a noteworthy correlation between insurance coverage and the promptness of medical treatments [4]. This revelation has highlighted the potentially pivotal role of insurance status in shaping the timely delivery of healthcare services [7]. Yet, despite these significant findings, the scholarly landscape continues to grapple with a palpable gap in comprehensive inquiry into the intricate interplay between physicians’ perceptions and their navigation of the intricate disparities within the Saudi Arabian healthcare fabric.
The realm of healthcare delivery is inextricably intertwined with the influence of physicians’ perceptions upon their clinical practices [8]. Kruk et al. have illuminated the pivotal role of physicians’ understanding of the healthcare system, particularly insurance policies, in shaping their clinical decisions [9]. The healthcare landscape of Saudi Arabia elegantly harmonizes traditional values and progressive medical practices, and beckons for an in-depth exploration into how physicians’ perceptions meld with the intricate nuances of insurance status. This interplay signifies a critical determinant that can potentially shape the trajectory of medical choices. To illuminate this complex interplay, it is essential to navigate the multifaceted cultural and healthcare framework within which Saudi Arabian physicians operate [10]. Understanding these perceptions within this broader context becomes a cornerstone for unraveling the complexities that underline the intricate interplay between insurance status and physicians’ medical decisions.
Saudi Arabia’s societal fabric intricately weaves together cultural, social, and economic threads that can potentially overlay the interface between insurance status and clinical decisions [11]. The scholarly insight provided by Alodhayani et al. has highlighted the discernible impact of cultural norms and societal expectations on medical choices [12]. This multifaceted interjection necessitates a deliberate exploration of how these cultural and contextual elements intersect with insurance-related considerations. This intersection amplifies the intricate dynamics that influence physicians’ decision-making processes, accentuating the complexity of their responses to insurance-related factors. Unpacking these multidimensional layers provides a more profound understanding of the intricate influences that shape clinical choices within the dynamic Saudi Arabian healthcare landscape.
Hence, this study aimed to investigate how physicians perceived the influence of insurance status on treatment options and medical interventions and to explore the extent to which physicians discussed insurance-related considerations with patients during the shared decision-making process.
Materials and methods
Study design and area
This research employed a cross-sectional exploratory study conducted in various healthcare facilities all over Saudi Arabia from April to October 2023. The study involved data collection regarding their perceptions of the impact of insurance status on clinical decision-making.
Participants' inclusion and exclusion criteria
The study participants included practicing physicians from various specialties and categories (consultants, registrars, senior registrars/general practitioners) working in private or both types of practices (government and private) and holding Saudi and non-Saudi nationality. Doctors exclusively working in government settings were excluded.
Data collection
Data were collected using an electronic questionnaire. The questionnaire was composed of two sections, including sociodemographic information and the Modified 9-item Shared Decision-Making Questionnaire (SDM-Q-Doc, physician version) [13]. SDM-Q-Doc was modified to reflect the context of insurance-related considerations in clinical decision-making.
Data sampling
A stratified random sampling technique was used to collect data.
Data analysis
Data collected through the questionnaire was analyzed using both descriptive and inferential statistical methods using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY) software. Descriptive statistics were used to summarize sociodemographic information and participants' responses to individual questionnaire items. Inferential statistics such as analysis of variance (ANOVA) and student's t-test were employed to identify significant associations between participants' characteristics and their perceptions of insurance-related influences on clinical decision-making. P-value was considered significant if it was less than 0.05.
Ethical considerations
Ethical approval was sought from an appropriate institutional review board (IRB) before conducting the study. Informed consent was obtained from all participating physicians. To ensure confidentiality, all collected data were anonymized and stored securely. This study was a non-interventional, survey-based research focusing on the impact of insurance status on physicians' clinical decision-making processes. The study methodology did not involve direct patient interactions, use of human tissue, or access to identifiable patient records. Furthermore, all data collected were entirely anonymous, ensuring that no identifiable information was used or mentioned.
Results
Participants' characteristics
About 430 participants were included in the current study, of which 230 (53.5%) were male and 200 (46.5%) were female. Half of the participants (*n *= 215, 50%) were within the age group of 31 to 40 years. About 145 (33.7%) were Saudi, and the rest 285 (66.3%) were non-Saudi. The majority of the participants (*n *= 258, 60%) were medical officers with one to five years of experience (*n *=187, 43.5%). Three hundred one participants (70%) were engaged in private practice only, while the remaining 129 participants (30%) were involved in both private and governmental practices (Table 1).
Physicians’ perceptions of insurance status impact on clinical decision-making
About 287 (66.7%) participants agreed that they take into consideration the patient's insurance status when discussing potential treatment options. Around 317 (73.7%) agreed that they would ensure that their patients are aware of how their insurance status might impact the range of treatment options available to them. Discussing the financial implications of different treatment options with patients considering their insurance coverage was agreed by 318 (74%) participants. Differences in the treatment choices made by patients based on their insurance status and insurance-related considerations influenced the time was agreed by 331 (77%) and 288 (67%) participants, respectively. Almost 373 (86.7%) participants agreed that insurance status can impact patient outcomes and treatment effectiveness, and 274 (63.7%) participants agreed that insurance-related factors played a role in the shared decision-making process between them and their physicians. However, 260 (60.5%) felt that patients with different insurance statuses received equitable medical care. Only 318 (74%) participants agreed that addressing insurance-related disparities in healthcare is essential for improving patient outcomes (Table 2).
When discussing treatment options, 287 (66.7%) participants agreed that they considered the patient's insurance status (Figure 1).
Physicians' answers about whether they take into consideration a patient's insurance status when discussing potential treatment options.
The mean of the SDM-Q-Doc total score was found to be 24.0 ± 3.21 (range 13-27) out of a total of 27. A statistically significant association was found between years of experience and the score of insurance status impact on clinical decision-making (*P *= 0.002). Participants with more than 10 years of experience had a higher score of insurance status impact on clinical decision-making. Physicians in the age group of 31 to 40 years had a higher score of insurance status impact on clinical decision-making (P < 0.001 and 0.005, respectively). The type of practice was also found to be significantly associated with the score of insurance status impact on clinical decision-making (P = 0.012). Participants practicing in both private and governmental sectors had a higher score of insurance status impact on clinical decision-making (Table 3).
Table 3: Factors associated with physicians' perceptions of how insurance status impacts clinical decision-making.The data have been represented as mean ± SD. A higher mean reflects a higher impact on clinical decision-making.P-value was considered significant at P < 0.05.
Discussion
Determination of physicians’ perception about how insurance status impacts clinical decision-making. It also plays an undeniable role in deciding the patient's plan of management to be finalized from the patient's side [3].
About two-thirds (287, 66.7%) of participants agreed that they considered the patient's insurance status when discussing potential treatment options; similar findings were reported in a congruent study [14].
More than two-thirds (317, 73.7%) agreed that they would ensure that their patients were aware of how their insurance status might impact the range of treatment options available to them; analogous findings were reported in Murray's study [15].
Discussing the financial implications of different treatment options with patients considering their insurance coverage was agreed by 318 (74%) participants; similar findings were mentioned in a parallel study in which decision-making belonged to both the physician and the patient [16]. More than two-thirds (318, 74%) of the participants agreed that addressing insurance-related disparities in healthcare is essential for improving patient outcomes. And 373 (86.7%) participants agreed that insurance status can impact patient outcomes and treatment effectiveness.
Out of 27, the mean SDM-Q-Doc total score was found to be 24.0 ± 3.21, whereas similar findings were reported in a congruent study [17].
Regarding the association between factors related to physicians’ perception of how insurance status impacted clinical decision-making; age was found to be significantly associated with the score as participants aged 31-40 years had higher scores than others, while contradictory findings were reported in the study [17]. A statistically significant association was found between years of experience and score of insurance status impact on clinical decision-making, with participants who had more than 10 years of experience having the higher score. The type of practice was also found to be significantly associated with the score of insurance status impact on clinical decision-making. Similar results were reported in a congruent study, which demonstrated that the type of practice influenced the physicians’ clinical decision-making in patients with insurance [18,19].
At the heart of modern healthcare ecosystems lies the instrumental role of Health Information Systems (HIS) in optimizing care delivery. Patient information, harvested meticulously from these systems, informs clinical decisions while potentially recalibrating the weight assigned to insurance-related factors. The investigation in some prior studies aptly emphasized the precision of diagnoses and treatment strategies catalyzed by the integration of comprehensive electronic health records [20, 21]. However, within the unique contours of the Saudi Arabian healthcare milieu, the intricate dance between HIS integration and the delicate balance of insurance status and clinical decisions remains an untrodden path. Delving into this domain holds the promise of unearthing the extent to which technology-driven insights reshape physicians’ perceptions regarding treatment decisions, subsequently finding expression in the intricate tapestry of clinical scenarios [22]. This exploration extends beyond mere technological integration, unveiling the dynamic ways in which healthcare systems evolve to harmonize diverse determinants, including insurance status, into the delicate fabric of clinical decision-making processes.
This study had some limitations. Despite using stratified random sampling, there was insufficient randomization due to nonresponse from the section of the targeted sample to the online questionnaire resulting in the observed demographic characteristics of the current study sample as well as the subsequent result. Additionally, the exclusion of doctors who work only in government is devoid of the study of important sections and might affect the observed responses.
Conclusions
This study concluded that insurance status’ had impact on the clinical decision-making process, which was influenced by specific parameters of physicians like age, experience, specialty, and type of practice. Physician-patient relationship and interaction should be improved and all management options should be discussed with the advantages and disadvantages of particular management option compared to other options to set the suitable plan of management for particular patients according to their economic and insurance status with the most proper management plan available and acceptable for the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A review of clinical decision making: models and current research J Clin Nurs Banning M 1871951720081733109510.1111/j.1365-2702.2006.01791.x · doi ↗ · pubmed ↗
- 2Teamwork in healthcare: key discoveries enabling safer, high-quality care Am Psychol Rosen MA Diaz Granados D Dietz AS Benishek LE Thompson D Pronovost PJ Weaver SJ 4334507320182979245910.1037/amp 0000298 PMC 6361117 · doi ↗ · pubmed ↗
- 3Primary care physicians' perceptions of the effect of insurance status on clinical decision making Ann Fam Med Meyers DS Mishori R Mc Cann J Delgado J O'Malley AS Fryer E 399402420061700313810.1370/afm.574PMC 1578641 · doi ↗ · pubmed ↗
- 4The effects of health insurance on health-seeking behaviour: evidence from the Kingdom of Saudi Arabia Risk Manag Healthc Policy Al-Hanawi MK Mwale ML Kamninga TM 5956071320203260702710.2147/RMHP.S 257381 PMC 7308143 · doi ↗ · pubmed ↗
- 5Taking action on the social determinants of health in clinical practice: a framework for health professionals CMAJ Andermann A 083188201610.1503/cmaj.160177 PMC 513552427503870 · doi ↗ · pubmed ↗
- 6Health disparities: gaps in access, quality and affordability of medical care Trans Am Clin Climatol Assoc Riley WJ 1671741232012 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 3540621/23303983 PMC 3540621 · pubmed ↗
- 7Does insurance status influence outpatient flow? cross-sectional comparison of insured and uninsured patients in a tertiary hospital in Nigeria J Patient Exp Opurum NE Kemdirim CJ Uduak A Hart D Ogaji DS 23743735221077546920223528463110.1177/23743735221077546 PMC 8905219 · doi ↗ · pubmed ↗
- 8Physicians' perceptions and use of a health information exchange: a pilot program in South Korea Telemed J E Health Lee SI Park H Kim JW Hwang H Cho EY Kim Y Ha K 6046121820122235289810.1089/tmj.2011.0261 PMC 3466924 · doi ↗ · pubmed ↗