Rehabilitation and return to sport criteria following surgical treatment of osteochondritis dissecans of the capitellum: a systematic review
Andrew George, Brendan M. Holderread, Brian M. Phelps, Emily R. Erwin, William Singer, Robert A. Jack

TL;DR
This review examines when athletes can safely return to sports after surgery for a condition called osteochondritis dissecans of the capitellum.
Contribution
The study identifies a lack of standardized return-to-sport criteria and highlights the need for functional benchmarks.
Findings
Most studies use time-based criteria for return to sport, with a 6-month timeline being most common.
Elbow range of motion and imaging results are the most consistent return-to-sport criteria reported.
Return to sport rates after surgery are high, but there is no consensus on standardized rehabilitation protocols.
Abstract
Osteochondritis dissecans (OCD) of the capitellum is a well-described condition that most commonly affects adolescent throwing athletes and gymnasts. There is no gold standard rehabilitation protocol or timing for return to sport (RTS) after surgical management of OCD of the capitellum. The purpose of the study was to identify in the existing literature any criteria used for RTS following surgical treatment of OCD of the capitellum. The hypothesis was that surgeons would utilize length of time rather than functional criteria or performance benchmarks for RTS. Level 1 to 4 studies evaluating athletes who underwent surgery for OCD of the capitellum with a minimum follow-up of 1-year were included. Studies not describing RTS criteria, including less than 1-year follow-up, non-operative management only, and revision procedures were excluded. Each study was analyzed for RTS criteria, RTS…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
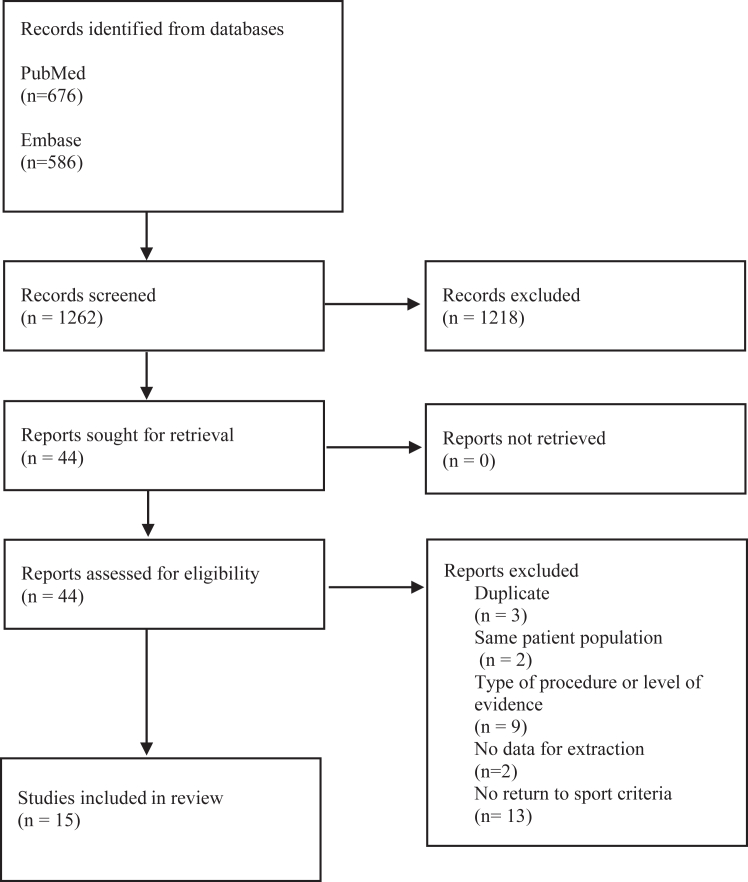 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Shoulder Injury and Treatment · Orthopedic Surgery and Rehabilitation
Osteochondritis dissecans (OCD) of the capitellum is a well-described condition that most commonly affects adolescent throwing athletes and gymnasts.11 It is theorized to result from repetitive valgus compression and shear forces across the radio-capitellar joint. This leads to localized injury and vascular insufficiency to the capitellum, and ultimately separation of articular cartilage from subchondral bone.5
Stable OCD lesions of the capitellum can be treated non-operatively with activity restriction and close observation.19 Stable lesions that do not respond to nonoperative care, as well as unstable lesions, warrant surgical management.23 Surgical management is diverse and may include open or arthroscopic débridement, loose body removal, microfracture, or drilling.6 Fixation (cartilage repair) may be warranted for larger lesions that are not completely displaced. In cases of larger lesions that engage the radial head, as well as revision cases in which arthroscopic treatment has failed, osteochondral autograft or allograft transplantation surgery may be warranted.22
While surgical techniques and outcomes following operative management of capitellar OCD lesions have been investigated in depth in the literature, the timeline of rehabilitation and return to sport (RTS) criteria after surgery is not standardized. The purpose of this study was to identify any described criteria in the literature used to advance patients through their rehabilitation and ultimately to RTS. The authors hypothesized that length of time from surgery would be used most often, rather than functional criteria or performance benchmarks. This hypothesis was based on several recent studies in the sports and shoulder/elbow literature that found time-based criteria were most often used after other surgeries of the shoulder and elbow, including surgical stabilization for anterior shoulder instability and ulnar collateral ligament reconstruction.9^,^12
Materials and methods
Search strategy
A search was conducted in PubMed and Embase databases from their inception to December 2022 using the terms “elbow”, “arthroscopy”, “athlete”, “return to”, “osteochondritis dissecans”, “treatment”, “capitellar” or “capitellum”, and “outcome”. All references of articles selected were evaluated to identify articles that were potentially missed by this search strategy.
The article search and review were completed by 3 reviewers under supervision of an attending orthopedic surgeon who has fellowship training in sports medicine. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart provides the exact number of articles identified, screened, excluded, and included with rationale (Fig. 1). Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria were followed throughout the described systematic review.Figure 1PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram depicting assessment strategy for including studies in the systematic review.
Inclusion/exclusion criteria
Included studies were those (1) evaluating patients undergoing surgical treatment of OCD of the capitellum, (2) with a minimum 1-year follow-up, and (3) with an English version of the article available for review. Studies not describing RTS criteria, narrative reviews, technical notes/tips, letters to the editor, studies with less than 1-year follow-up, studies describing nonoperative management only, and studies evaluating only revision procedures, were excluded.
Patient demographics and outcomes
Surgical indication, surgical technique, total numbers of patients, elbows receiving operative treatment, age of patient cohort (mean), level of competition, and sport played were extracted for evaluation. Patient-reported outcomes surveys were not recorded due to heterogeneity in surveys used. However, mean time of follow-up and success in return to activities or sport were extracted. Particular attention was given to analyzing explicit criteria utilized in decision making for gradual RTS/activity or full and unrestricted RTS/activity. Articles with missing or unclear data were excluded.
Quality of literature assessment
Coleman Methodology Scores (CMS) were assigned by two independent reviewers. CMS quantitatively assesses methodological quality of a reported research study with 10 criteria providing a possible score from 0 to 100 (Table I). The assessment specifically evaluates study size, follow-up, surgical procedures, type of study, diagnostic certainty, description of surgical technique, description of postoperative rehabilitation, outcome criteria, procedure for assessing outcome, and description of subject selection process.Table IColeman Methodology Scores along with the means and standard deviations for each scoring category with a maximum score of 100.Authorship12345678910TotalAyzenberg et al, 20212751005510105562Allahabadi et al, 2020110270551023549Matsuura et al, 20201610510005533546Matsuura et al, 201715105100551023555Oshiba et al, 20162045100551024550Maruyama et al, 20161445100351023547Takeba et al, 201524102100051023547Koehler et al, 201513051010551023555Uchida et al, 2015251051010551035568Nishinaka et al, 2014171051010551025567Wulf et al, 20122775100551023552Bojanić et al, 20127451010051025556Rahusen et al, 20062105101003025540Yamamoto et al, 200628105101055023555Byrd et al, 200284500031023532Mean ± SD6.3 ± 3.94.4 ± 1.28.8 ± 3.04.0 ± 4.93.3 ± 2.44.8 ± 0.88.3 ± 3.53.0 ± 2.44.1 ± 1.65.3 ± 1.352.1 ± 9.5SD, standard deviation.1, study size (10); 2, mean follow-up (5); 3, No. of interventions per group (10); 4, study type (15); 5, diagnostic certainty (5); 6, description of surgical technique (5); 7, description of postoperative rehabilitation (10); 8, outcome criteria (10); 9, procedure for assessing outcomes (15); 10, description of patient selection process (15).
Quality of return to sport assessment
Quality of RTS methodology was assessed according to methodology described by Zaman et al29 by two independent reviewers (Table II). This assessment evaluates description of rehabilitation protocol, timeline for return to activity, objective/subjective criteria, and specific measurement criteria.Table IIScoring report for return to sport value assessment.Surgical techniqueAuthorshipRehabilitation protocolTimeline for return to activityObjective/Subjective criteriaSpecific measurement criteriaRTS article rating score (4)Arthroscopic microfracture/debridementAllahabadi et al, 2020111114Wulf et al, 20122711103Bojanić et al, 2012711002Rahusen et al, 20062110001Matsuura et al, 20201611002Byrd et al, 2002811103Osteochondral autograft transplantationOshiba et al, 20162011103Maruyama et al, 20161411114Matsuura et al, 20171511114Nishinaka et al, 20141711114Yamamoto et al, 20062811103Ayzenberg et al, 2021211103Arthroscopic fragment fixationAllahabadi et al, 2020111114Takeba et al, 20152411103Koehler et al, 20151311103Uchida et al, 20152511114Mean ± SD1.0 ± 0.000.9 ± 0.260.8 ± 0.410.3 ± 0.493.1 ± 0.88RTS, return to sport.A maximum of 1 point was given per category if the study met the criteria.
Statistical analysis
All data were collected and analyzed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA).
Results
1262 studies identified were assessed for eligibility. Fifteen studies met inclusion criteria with 288 athletes.1^,^2^,^7^,^8^,^13^,^14, 15, 16, 17^,^20^,^21^,^24^,^25^,^27^,^28 The methodological quality was fair (CMS: 52.1+/− 9.5) with most studies reporting sufficient follow-up, as well as good diagnostic certainty and description of surgical technique (Table I). Surgical procedures included arthroscopic microfracture/débridement, arthroscopic fragment fixation, or osteochondral autograft transplantation. Among grafts used in the osteochondral autograft transplantation cohort, the most common site of graft harvest was the ipsilateral olecranon. Baseball was the most commonly identified sport (13/15, Table III). Recreational/amateur level of preoperative play was most commonly reported (6/15, Table IV).Table IIIThe distribution of sports included in the overall patient population.Surgical techniqueSport included in patient populationNo. of studies includedArthroscopic microfracture/debridementNot reported2Baseball3Softball1Gymnastics3Basketball1Tennis2Water polo1Handball1Track and field1Karate1Volleyball1Osteochondral autograft transplantationNot reported1Baseball6Basketball2Soccer1Gymnastics1Tennis1Weightlifting1Arthroscopic fragment fixationNot reported1Baseball3Gymnastics1Lacrosse1Table IVLevels of play at time of surgery.Surgical techniqueLevel of play before surgeryNo. of studies includedArthroscopic microfracture/debridementNot reported2Recreational2Middle school3High school3Competitive/elite1Osteochondral autograft transplantationNot reported1Recreational4Competitive/elite2Arthroscopic fragment fixationNot reported2Recreational1Competitive/elite1Several studies described multiple patient populations.
Described rehabilitation protocols were extracted, and recurring themes are summarized in Table V, stratified by type of surgical procedure. All studies reported a rehabilitation protocol with immobilization followed by bracing with progressive range of motion (ROM). The majority of studies reported using time-based criteria for RTS (11/15). Twelve out of fifteen studies described a multiphase rehabilitation program, with an average of 4 phases. Ten studies utilized a postoperative survey. The most commonly used survey was the Timmerman-Andrews assessment. All studies reported RTS as a rate. The overall RTS rate was 80.9% (233/288). The most commonly reported time to RTS was 6 months (4/15). The earliest time to RTS was 3 months, and the longest time was 12 months (Table VI).Table VSummary of the postoperative rehabilitation parameters.Surgical techniquePostoperative rehabilitation parametersNo. of studies includedArthroscopic microfracture/debridementImmobilization/bracing with progressive ROM/continuous passive motion5Strengthening3Sport-specific protocol4Supervised physical therapy5Multiphase program5# of phases3.6∗Throwing mechanic education1Interval throwing program2Postop survey used for RTS criteria3Osteochondral Autograft TransplantationImmobilization/bracing with progressive ROM/continuous passive motion6Strengthening4Sport-specific protocol5Supervised physical therapy3Multiphase program5# of Phases4.3∗Interval throwing program6Throwing mechanic education1Provided interval throwing program specifics3Postop survey used for RTS criteria5Arthroscopic Fragment FixationImmobilization/bracing with progressive ROM/continuous passive motion4Strengthening4Sport-specific protocol1Supervised physical therapy1Multiphase program2# of Phases3∗Interval throwing program1Cryotherapy & electrical stimulation1Cardiovascular training1Postop survey used for RTS criteria3∗Average rather than count.Table VIReturn to sport timelines.Surgical techniqueRTS timeline reportedNo. of studies includedArthroscopic microfracture/debridementN/R44.5 months15 months1Osteochondral autograft transplantationN/R13 months16 months38-12 months1Arthroscopic fragment fixationN/R36 months1RTS, return to sport.Studies that only mentioned return to activity or throwing are not represented and are included under the “Not reported” category.
Each article was rated on a scale of 0-4 to assess its value in reviewing RTS criteria as described by Zaman et al29 (Table II). All studies reported at least 1 of the following 4 metrics of RTS criteria: rehabilitation protocol, timeline for return to activity, objective/subjective criteria, and specific measurement criteria. The average RTS value score was 3.1 +/− 0.88. Five out of fifteen studies achieved a value of 4/4, which is notably higher than other RTS criteria literature, ie, UCL reconstruction.12 Four of these five studies utilized either x-ray or magnetic resonance imaging to confirm graft healing or fragment fixation healing. Three of the five studies utilized return of normal elbow ROM as an objective criterion for RTS. Three of the five studies utilized time-based criteria in addition to these objective measures, ranging from 2-3 months postoperatively before throwing activities resumed.
Discussion
While surgical techniques and outcomes after operative management of capitellar OCD lesions are well-described, validated rehabilitation protocols and RTS criteria are lacking in the literature. The authors’ hypothesis was supported, as the majority of studies utilized time-based criteria for return to activity, rather than functional criteria or performance-based metrics.
All studies reported a rehabilitation protocol with immobilization followed by bracing with progressive ROM or continuous passive motion. While return to play criteria are more standardized after other sports medicine procedures such as anterior cruciate ligament reconstruction,3^,^4^,^10 there is a lack of well-defined objective criteria that could advance a patient through rehabilitation after capitellar OCD surgery.
Of the 5 studies that achieved 4/4 in terms of their value in assessing RTS criteria as defined by Zaman et al,8 the most common objective measures were return of normal elbow ROM without pain and healing on radiographs and/or magnetic resonance imaging. These were also the two most common objective measures utilized when assessing all 15 studies. Objective measures were most often used in conjunction with time-based criteria. While radiographic healing may be one of the more objective measures utilized, this could be limited by the degree of intrarater and inter-rater agreement in assessing OCD characteristics and healing.18 Nevertheless, return of elbow ROM and healing on imaging are the two objective measures most consistently found in the literature. Interestingly, no two studies employed the same RTS/activity criteria, highlighting the variability in postoperative protocols. Given this wide variability, further comparative research is needed to determine an optimal protocol and RTS criteria following surgical treatment of capitellar OCD.
In terms of RTS rate, 81% of patients were able to RTS at the same level. There was a wide variety of timelines for RTS, ranging from 3 to 12 months. The average time to RTS was 6 months. This is consistent with previously published work, reporting about an 86% RTS rate at 6 months after surgical management of capitellar OCD lesions.26 In a systematic review and meta-analysis of RTS after surgical management of capitellar OCD, Westerman et al26 found a greater percentage of athletes were able to return to high-level athletics after osteochondral autograft or allograft transplantation surgery procedures compared to débridement or fixation procedures. However, rehabilitation protocols and RTS criteria were not assessed.
This study has several important limitations. Physicians who regularly treat OCD lesions of the elbow may have published RTS criteria and rehabilitation protocols available for patients and physical therapists. This review would have excluded these protocols in an effort to remain standardized and in accordance with prior RTS criteria study methodology.12 Second, while we stratified our data by type of procedure performed, within this stratification there is still likely variability in size and geography of lesion that could affect postoperative rehabilitation protocol and outcomes. Finally, there was variability in the competitive level of athletes. Higher level athletes likely had a more personalized and sport-specific protocol than recreational athletes.
Conclusion
The overall RTS rate after surgical treatment of capitellar OCD is high with no consensus on RTS criteria. The two most consistent RTS criteria reported in the literature are return of elbow ROM and healing demonstrated on postoperative imaging. There is a wide range of time to RTS in the literature, which may be sport dependent. Further research is needed to develop functional and performance-based metrics to better standardize RTS criteria and rehabilitation protocols.
Disclaimers:
Funding: No funding was disclosed by the authors.
Conflicts of interest: The authors, their immediate families, and any research foundation with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Allahabadi S.Bryant J.K.Mittal A.Pandya N.K.Outcomes of arthroscopic surgical treatment of osteochondral lesions of the elbow in pediatric and adolescent athletes Orthop J Sports Med 82020232596712096305410.1177/2325967120963054 PMC 765853033225011 · doi ↗ · pubmed ↗
- 2Ayzenberg M.Clippinger B.Slate E.L.Kozin S.H.Zlotolow D.A.Outcomes of osteochondral autograft transplantation in pediatric patients with osteochondritis dissecans of the capitellum J Hand Surg Am 4620211028.e 11028.e 1510.1016/j.jhsa.2021.02.02433902975 · doi ↗ · pubmed ↗
- 3Barber-Westin S.D.Noyes F.R.Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction Arthroscopy 2720111697170510.1016/j.arthro.2011.09.00922137326 · doi ↗ · pubmed ↗
- 4Barber-Westin S.D.Noyes F.R.Objective criteria for return to athletics after anterior cruciate ligament reconstruction and subsequent reinjury rates: a systematic review Phys Sportsmed 39201110011010.3810/psm.2011.09.192622030946 · doi ↗ · pubmed ↗
- 5van Bergen C.J.van den Ende K.I.Ten Brinke B.Eygendaal D.Osteochondritis dissecans of the capitellum in adolescents World J Orthop 7201610210810.5312/wjo.v 7.i 2.10226925381 PMC 4757654 · doi ↗ · pubmed ↗
- 6Bexkens R.van den Ende K.I.M.Ogink P.T.van Bergen C.J.A.van den Bekerom M.P.J.Eygendaal D.Clinical outcome after arthroscopic debridement and microfracture for osteochondritis dissecans of the capitellum Am J Sports Med 4520172312231810.1177/036354651770484228520461 · doi ↗ · pubmed ↗
- 7Bojanic I.Smoljanovic T.Dokuzovic S.Osteochondritis dissecans of the elbow: excellent results in teenage athletes treated by arthroscopic debridement and microfracture Croat Med J 532012404710.3325/cmj.2012.53.4022351577 PMC 3284183 · doi ↗ · pubmed ↗
- 8Byrd J.W.Jones K.S.Arthroscopic surgery for isolated capitellar osteochondritis dissecans in adolescent baseball players: minimum three-year follow-up Am J Sports Med 30200247447810.1177/0363546502030004040112130399 · doi ↗ · pubmed ↗