Penetrating Chest Trauma in a Child Caused by a Fall on a Metallic Bar: A Case Report
Hatim Jabri, Othmane Alaoui, Abdelhalim Mahmoudi, Khalid Khatalla, Youssef Bouabdallah

TL;DR
A 13-year-old child suffered chest trauma from a metallic bar but recovered well after careful removal without major surgery.
Contribution
This case report highlights the management of a rare pediatric intrathoracic foreign body without thoracotomy.
Findings
The metallic bar was successfully removed through the entry wound without thoracotomy or thoracoscopy.
The patient showed no complications and was discharged after three days with good follow-up improvement.
Imaging confirmed no vital organ damage despite the penetrating injury.
Abstract
Penetrating chest trauma in children is an uncommon condition. Patients may be asymptomatic or in a critical state. Visceral and vascular damage are frequently present when penetrating objects enter the thoracic cavity. Although many studies have discussed penetrating thoracic trauma in adults, very few deal with the pediatric population. Here, we present the case of a 13-year-old child with an intrathoracic metallic bar after penetrating chest trauma. The clinical examination showed a stable patient with a palpable bar and subcutaneous emphysema in the left axillary area. The radiological scan did not reveal any vital damage. The bar was removed through the entry wound without thoracotomy or thoracoscopy. The patient evolved without any incident and was discharged after three days. Good improvement was noted over three months of follow-up. Intrathoracic foreign bodies secondary to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1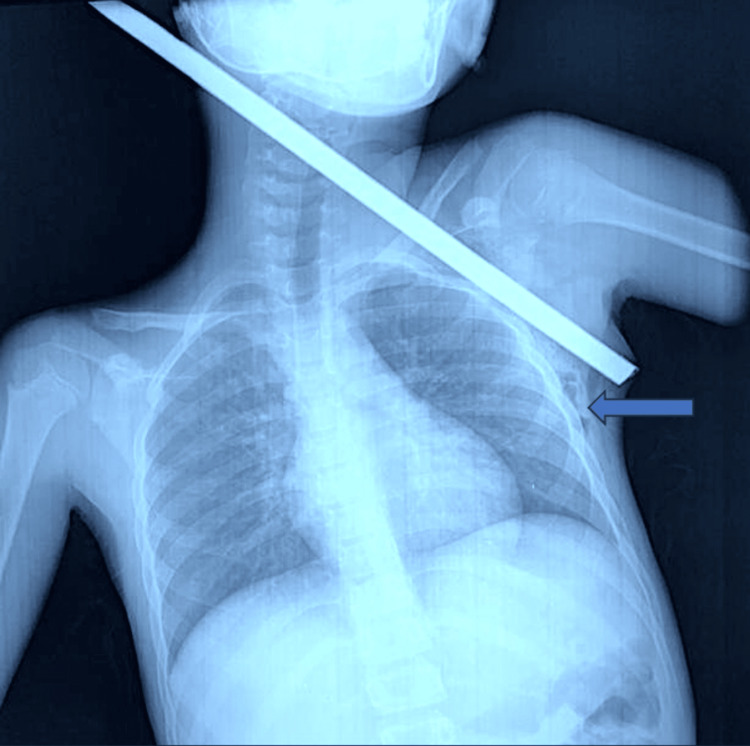 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5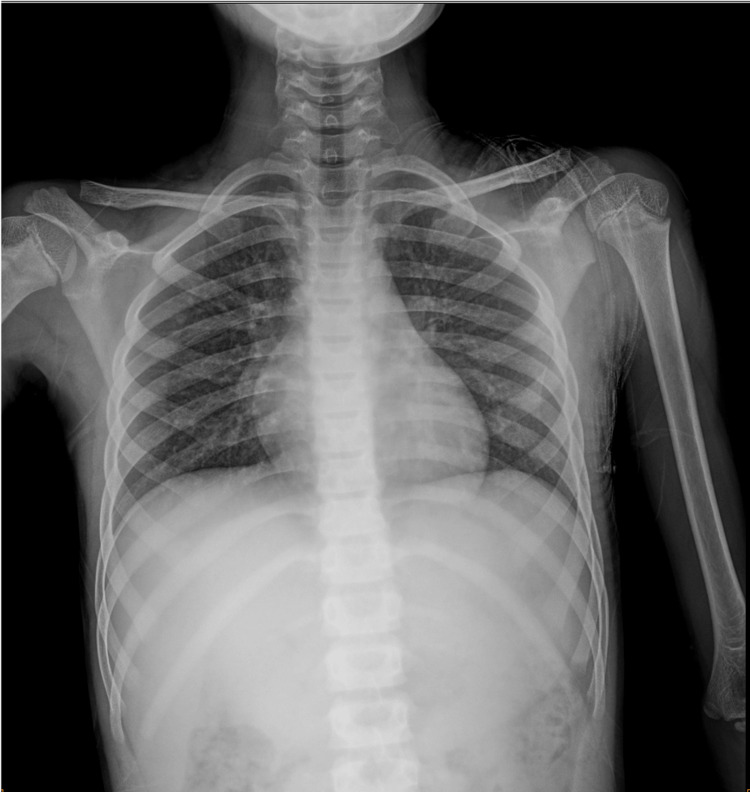 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma Management and Diagnosis · Traumatic Ocular and Foreign Body Injuries · Foreign Body Medical Cases
Introduction
Penetrating chest trauma is uncommon [1]. Its incidence remains unknown, with studies on this subject in children being rare. This case report presents an unusual case of penetrating thoracic trauma in a child.
Penetrating injuries can be mild or life-threatening, depending on the site, course of the penetrating object, and depth of the injury [2]. These lesions have a very high mortality rate due to the critical anatomical structures in the chest [2,3]. Efficient evaluation and identification of patients requiring surgical intervention is imperative. The approach in such circumstances must always consider the dangers associated with removing the object and the potential complications [4].
Here, we present an unusual case of a 13-year-old child who presented with penetrating chest trauma after falling on a metallic bar.
Case presentation
A 13-year-old male presented to the emergency department with penetrating thoracic trauma caused by a metal bar after an accidental fall from a height of 2 m, with an entry from the left subclavian region without leaving the axillary region (Figure 1).
Clinical image showing the foreign body penetrating the chest.
Clinical examination identified a conscious patient. The patient had a respiratory rate of 20 breaths per minute, an oxyhemoglobin saturation of 98% in room air, a pulse of 98 beats per minute, and a blood pressure of 96/64 mmHg. There were no signs of active bleeding. A complete clinical examination revealed a palpable foreign body with subcutaneous emphysema in the left axillary region. The vascular and neurological examination of the left upper limb was normal, without other abnormalities. After conditioning and giving 500 mg of amoxicillin-clavulanic acid with an intramuscular injection of 1,500 IU of anti-tetanus serum, the patient underwent a chest X-ray, which showed the metal bar penetrating through the left thorax, without signs of pneumothorax or hemothorax (Figure 2).
Chest X-ray showing a metallic rod penetrating through the left thorax.The blue arrow shows the subcutaneous emphysema.
We performed a CT angiography of the chest, which excluded pleural, pulmonary, cardiovascular, and neurovascular injuries evident in the three-dimensional reconstruction (Figure 3).
Three-dimensional visualization of the CT scan revealing a rod penetrating the left hemithorax through the middle part of the superior surface of the left clavicle and arriving at the axillary region.
However, we noted the presence of subcutaneous emphysema in the soft tissues of the left anterior and posterolateral chest wall (Figure 4).
CT angiography of the chest showing the presence of subcutaneous emphysema in the soft tissues of the left posterolateral chest wall without major injuries.
Blood storage was done. Then, we elected to extract the rod through the entry site from the same tract as its entry and exit under local anesthesia by percutaneous injection of 4 mL of lidocaine 2% solution in the operating room, which was performed without incident. The vital parameters did not change, and emphysema remained constant. There was no visible bleeding; the pectoralis major was torn, with necrotic and missing skin surrounding the areas of entry (Figure 5).
Post-extraction picture showing necrotic and missing skin surrounding the areas of entry.
Betadine-soaked gauze was put into the open thoracic wound to avoid infection. The pectoralis major was sutured, the dead tissue was debrided, and a pressure dressing was applied. The patient was shifted immediately to the observation room. He underwent a chest X-ray two hours after extraction, and no pneumothorax was noted (Figure 6).
Post-extraction chest X-ray without abnormalities.
The patient was discharged from the hospital on the third day after a normal chest X-ray. After 10 days, no wound infection was noted. Regular clinical and radiological findings over three months showed good recovery.
Discussion
Penetrating chest trauma represents a challenging situation. In children, this condition is rarely reported [5]. The guidelines for the management of penetrating chest trauma are as follows: avoid exploring the wound site, avoid removing the object without a complete check-up, and do so only when anesthesia and surgical support are available [2]. The treatment of thoracic wall foreign bodies remains controversial [1,6]. The thoracic angiogram provides a detailed analysis of the characteristics of the foreign body, its location, and associated organ damage. Fewer than 20% of patients require surgical treatment [7,8].
Thoracotomy has long been considered the standard treatment for major thoracic trauma involving foreign bodies [4]. However, the large incisions involved in thoracotomy might be associated with significant morbidity and hospitalization [4,9]. Since its appearance, thoracoscopy has become a safer approach for the management of stable patients, and thoracotomy is recommended in cases of hemodynamic instability [4].
The prognosis after penetrating thoracic trauma depends on the mechanism, location, associated injuries, hemodynamic status, appropriate imaging, and treatment [7].
According to Chen et al. [10], if it is confirmed that the foreign body has not caused organ, vessel, or nerve damage, surgical removal under local anesthesia should be considered; otherwise, general anesthesia and close hemodynamic monitoring should be considered.
Our patient had no vascular or organ damage. The first reason was that the metal bar was at a fortunate angle to the patient’s body. The second was that the cotton clothes around the bar provided soft protection for vessels. Therefore, after conditioning and performing a CT scan, which ruled out any severe lesions, the metallic bar was removed by just drawing it out. A postoperative chest X-ray confirmed the absence of complications.
Despite the particularity of this case, the principal limitation was the absence of vital damage, which made management less challenging.
Conclusions
Penetrating thoracic injuries by metallic bars in children are uncommon. An initial evaluation and transfer to an appropriate center are necessary. In stable patients, it is necessary to complete an assessment of the trauma injuries to determine the position of the foreign material and identify potential complications. Then, if the condition permits, direct removal of the foreign body is possible.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Metallic foreign bodies in the thoracic wall in three cases Eurasian J Emerg Med Sezer HF Dayanir H 202204172018
- 2Penetrating chest trauma with iron rod in-situ: a surgical challenge Int J Contemporary Med Res Das NN Lakhotia S Akanksha A 0372020
- 3Transmediastinal gunshot wounds in a mature trauma centre: changing perspectives Injury Okoye OT Talving P Teixeira PG 119812034420132329875510.1016/j.injury.2012.12.014 · doi ↗ · pubmed ↗
- 4Penetrating chest trauma caused by a falling metallic bar: a case report J Thorac Dis Zhao W Chu M Ma L 402740321520233755965310.21037/jtd-23-767PMC 10407516 · doi ↗ · pubmed ↗
- 5Penetrating pulmonary injury caused by a steel rod Respirol Case Rep Amore D Muto E Casazza D Cicalese M Rispoli M Curcio C 08202010.1002/rcr 2.640PMC 743455732832085 · doi ↗ · pubmed ↗
- 6Foreign bodies in pleura and chest wall Ann Thorac Surg Weissberg D Weissberg-Kasav D 9589618620081872159110.1016/j.athoracsur.2008.05.036 · doi ↗ · pubmed ↗
- 7Penetrating chest trauma J Vis Surg Birrer DL Edu S Nicol A Neuhaus V 962020
- 8Selective nonoperative management of penetrating thoracic injury Eur J Emerg Med Van Waes OJ Halm JA Van Imhoff DI Navsaria PH Nicol AJ Verhofstad MH Vermeulen J 32382520182709276810.1097/MEJ.0000000000000401 · doi ↗ · pubmed ↗