Endovascular Treatment of a Multi-visceral Aortic Conduit Blowout With Parallel Stent Grafts and Coils
Dimitrios Moris, Mitchell W Cox, Zachary Williams

TL;DR
This paper describes a successful endovascular treatment for a life-threatening complication in a complex organ transplant surgery.
Contribution
The novel approach combines parallel stent grafts and coils to salvage a multi-visceral aortic conduit blowout without removing the transplanted organs.
Findings
Endovascular repair with parallel stent grafts and coils controlled bleeding effectively.
The method preserved graft perfusion and avoided sacrificing the transplanted viscera.
This approach is a viable alternative to open surgery in a high-risk, complex scenario.
Abstract
Multi-visceral transplantation (MVT) is a complex surgical procedure involving the transplantation of multiple abdominal organs as a single unit, typically used as bailout treatment of patients with devastating abdominal pathologies. Due to the complexity of the procedure, major and even life-threatening complications can happen. Vascular complications, including anastomotic breakdowns or pseudoaneurysms due to infections, can be universally lethal. Open surgical repair is often not an option due to the hostile operative field. We report a case of endovascular salvage of multi-visceral aortic conduit blowout utilizing parallel stent grafts and coils without sacrifice of the transplanted viscera. This combination can successfully control bleeding and maintain graft perfusion in this rare but devastating complication.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1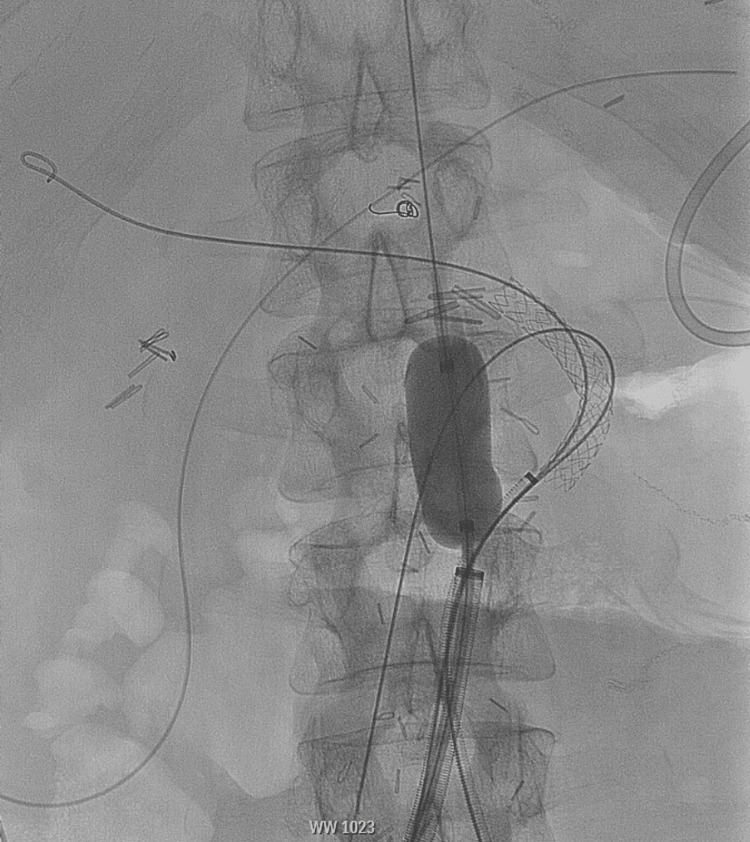 Figure 2
Figure 2 Figure 3
Figure 3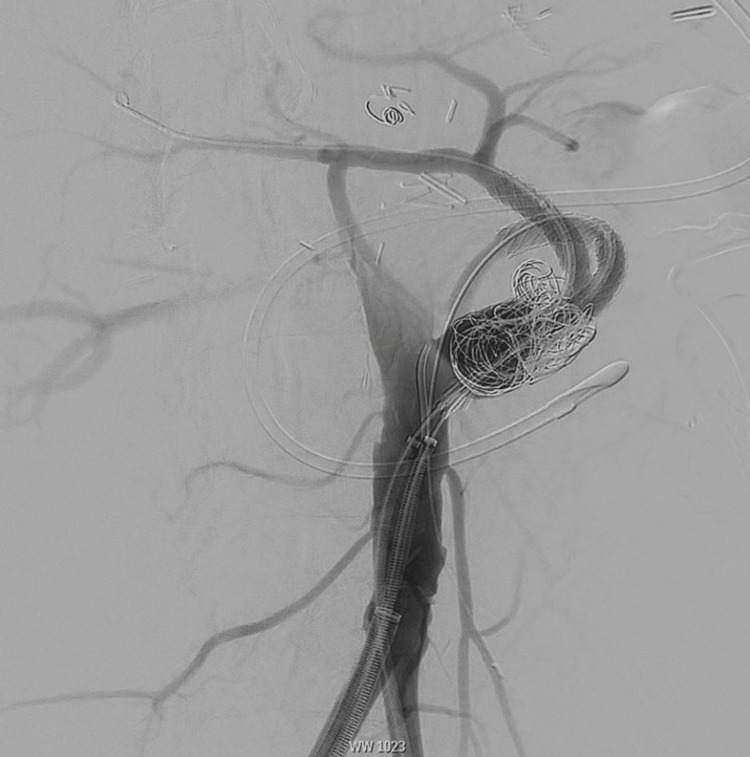 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Renal and Vascular Pathologies · Organ Donation and Transplantation
Introduction
Multi-visceral transplantation (MVT), also known as composite visceral transplantation or multiorgan transplantation, is a complex surgical procedure involving the implantation of multiple abdominal organs as a single unit, which typically includes the liver, pancreas, stomach, and small intestine and sometimes other organs such as the colon [1]. It is usually performed in cases where patients have extensive abdominal organ failure or diseases affecting multiple organs (short gut syndrome, intestinal failure, etc.).
Due to the complexity of MVT, complications are relatively common, mainly attributed to vascular complications, infections, and immunologic complications. Anastomotic breakdown or pseudoaneurysm is a universally lethal complication attributed to infections of the graft; thus, they require urgent repair. The incidence of arterial bleeding can be as high as 5% of cases and can pose a great challenge to surgeons involved due to the complexity of vascular reconstructions used for MVT and the presence of a hostile surgical field [2-4]. Thus, open repair is difficult, and its outcomes might be poor with many patients dying of graft loss or re-bleeding [2,3]. Anastomotic pseudoaneurysms are particularly challenging as rupture is typically fatal and attempts at repair often lead to graft loss or thrombosis and patient death. Endovascular techniques are appealing because they allow the exclusion of the pseudoaneurysm and control of the bleeding with minimal interruption in transplant organ perfusion. This technique also avoids an extremely challenging dissection in the setting of uncontrolled aortic bleeding. This report describes a case of endovascular salvage of MVT aortic conduit blowout utilizing parallel stent grafts and coils without compromising the transplanted viscera.
Technical report
A 45-year-old male with a remote history of Hodgkin lymphoma was treated with splenectomy and radiation therapy. He suffered multiple complications including cirrhosis, radiation enteritis requiring parenteral nutrition, and duodenal obstruction. He ultimately underwent an MVT of the liver, pancreas, stomach, small intestine, and right colon. The arterial reconstruction of donor viscera was accomplished via an end-to-side anastomosis of the infrarenal native aorta and donor thoracic aorta (Figure 1).
3D volume-rendered images demonstrating altered arterial anatomy with the visceral vessels being supplied via an infrarenal aortic conduit
Postoperatively, the patient developed severe necrotizing pancreatitis requiring multiple takebacks and debridements. During one of the re-explorations, significant bleeding was noted from the aortic conduit. Vascular surgery was intraoperatively consulted. Upon exploration, it appeared that the donor aorta was bleeding due to infection and a durable open surgical repair would be impossible due to the open abdomen, pancreatitis, infection, and prior transplant. An endovascular approach was pursued, and the patient was transferred to the hybrid suite. Bilateral femoral arterial access was obtained, and an aortogram was performed to better delineate the anatomy. An 18-Fr DrySeal (W.L. Gore & Associates, Inc., Flagstaff, AZ) was placed in the native aorta, and it was doubly accessed with two 7-Fr ANL sheaths (Cook Inc., Bloomington, IN). The aortic conduit was accessed, and a wire was advanced into the superior mesenteric artery. As the celiac artery was selected, massive bleeding was noted from the open abdominal incision, and it was clear that the donor aorta had ruptured, creating an aorto-atmospheric fistula. Temporary hemostasis was obtained with a Coda balloon in the native aorta and pledgeted sutures in the area of rupture (Figure 2).
Intraoperative angiogram showing Coda balloon in the native aorta assisted with hemostasis during stent graft placement
Leaving the Coda balloon inflated, the celiac artery was then re-selected. Two parallel covered stents (GORE® VIABAHN® VBX), one in the celiac artery and the other in the superior mesenteric artery, were deployed. Large coils were then deployed around these stents to try and seal any gutter leak. This achieved hemostasis (Figure 3).
Postoperative imaging after parallel stent grafting and coil embolization of the aortic conduit
Completion angiogram demonstrated excellent flow to the superior mesenteric artery and celiac artery with no contrast extravasation. The patient remained critically ill with incremental improvement and without any further bleeding episodes for the next month. At that time, surveillance cross-sectional imaging revealed a new pseudoaneurysm originating from the conduit.
The patient was taken back to the hybrid suite. Bilateral femoral arterial access was obtained, the celiac artery and superior mesenteric artery stents were cannulated, and the 7-Fr ANL sheaths were left in place. Several large coils were placed in the aortic conduit around the sheaths. Additional covered stents (GORE® VIABAHN® VBX) were deployed, extending the previously placed celiac artery and superior mesenteric artery stents up to the native aorta. Completion angiogram revealed good flow in the superior mesenteric artery and celiac artery without any filling of the pseudoaneurysm (Figure 4).
Intraoperative angiogram showing stent extension and additional coil placement up to the native aorta
Multiple intraoperative cultures and blood cultures grew Candida glabrata. After an 18-week hospitalization, the patient was ultimately discharged home remaining on suppressive isavuconazonium. Months later, he was readmitted with pneumonia and failure to thrive, ultimately requiring a tracheostomy. He ultimately elected to transition to comfort care and passed away 10 months after his initial repair.
Discussion
Multi-visceral transplantation is a complex surgical procedure involving the transplantation of multiple abdominal organs as a single unit, typically used as bailout treatment of patients with devastating abdominal pathologies. Starzl et al. performed the first MVT in 1987, and since then, there has been significant evolution of the procedure and its outcomes [5]. The arterial reconstructions performed for MVT use a donor thoracic aortic conduit sewn end-to-side to the native recipient infrarenal aorta [4]. Arterial bleeding due to conduit ruptures is extremely uncommon but fatal complications. When occurring late, as in our case, they may be associated with bacterial or fungal infection [2,3,6,7]. Emergent open surgery for damage control and repair of these life-threatening complications is challenging due to the hostility of the abdomen, often attributed to infection, desmoplastic reaction, or adhesive disease. Hybrid or endovascular techniques using wires, balloons or stents, coils, hydrogels, and thrombin have been proposed [8,9], but cases still require multiple takebacks due to re-bleeding events [2].
Pure endovascular access and management do not require exposure of the abdomen, but the complexity of the vascular anatomy in these cases is challenging. The morphology and etiology of the arterial blowout can limit the use of embolization, especially in the setting of large vessels such as the aortic conduit that was involved in our case. Managing a stump rupture from a previous MVT with aortic endograft has been previously reported [2]. Commercially available fenestrated aortic endografts are inadequate to adjust to the post-MVT anatomy. However, the use of physician-modified fenestrated endografts for the treatment of visceral transplant pseudoaneurysms has been reported [10]. Aortic endograft placement in conjunction with chimney or snorkel grafts for visceral perfusion has also been described and remains an option in this challenging situation [11,12].
Conclusions
Multi-visceral transplantation is a complex surgical procedure involving the transplantation of multiple abdominal organs as a single unit, typically used as bailout treatment of patients with devastating abdominal pathologies. These are challenging cases requiring complex arterial reconstructions. Anastomotic blowout or pseudoaneurysm formation attributed to infection is a universally lethal complication. In these patients, open surgical repair is often not an option due to the hostile operative field. The combination of endovascular parallel covered stent grafting and coil embolization can successfully control bleeding and maintain graft perfusion in this rare but devastating complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intestinal and multivisceral transplantation: indications and surgical techniques Radiol Clin North Am Pugliesi RA Dasyam AK Borhani AA 8618706120233749529310.1016/j.rcl.2023.04.007 · doi ↗ · pubmed ↗
- 2Combined surgical and interventional radiologic management strategies in patients with arterial pseudo-aneurysms after multivisceral transplantation Transplantation Amesur NB Zajko AB Costa G Abu-Elmagd KM 2352449720142412173410.1097/TP.0b 013e 3182 a 9029 a · doi ↗ · pubmed ↗
- 3100 multivisceral transplants at a single center Ann Surg Tzakis AG Kato T Levi DM 48049024220051619280810.1097/01.sla.0000183347.61361.7a PMC 1402343 · doi ↗ · pubmed ↗
- 4Composite and multivisceral transplantation: nomenclature, surgical techniques, current practice, and long-term outcome Gastroenterol Clin North Am Costa G Parekh N Osman M Armanyous S Fujiki M Abu-Elmagd K 3934154720182973503210.1016/j.gtc.2018.01.013 · doi ↗ · pubmed ↗
- 5Transplantation of multiple abdominal viscera JAMA Starzl TE Rowe MI Todo S 144914572611989 https://pubmed.ncbi.nlm.nih.gov/2918640/2918640 PMC 3005343 · pubmed ↗
- 6Intestinal and multivisceral transplantation: complications Radiol Clin North Am Dasyam AK Borhani AA Tirukkovalur NV Cruz RJ Jr 8718876120233749529410.1016/j.rcl.2023.04.008 · doi ↗ · pubmed ↗
- 7Aortic graft mycotic pseudoaneurysm as a severe complication after multivisceral transplantation: a case report Transplant Proc Calvo Pulido J Manrique Municio M Loinaz Segurola C 5395424820162710999610.1016/j.transproceed.2015.10.083 · doi ↗ · pubmed ↗
- 8Endovascular management of complete disruption of aortic anastomosis after pediatric multivisceral transplant J Vasc Surg Cases Innov Tech Mc Enaney RM Go C Li X Eslami MH 331336620203271516610.1016/j.jvscit.2020.05.004PMC 7371609 · doi ↗ · pubmed ↗