Traumatic Self-Inflicted Ventricular Laceration: A Case of Smith-Lemli-Opitz Syndrome in an Adult
Jennifer J Beuschel, Grace I Ng, Joanna C Abaraoha, Robert J Fortuna

TL;DR
An adult with intellectual disability was diagnosed with Smith-Lemli-Opitz Syndrome at age 33 after years of self-injurious behavior and a traumatic heart injury.
Contribution
This case highlights the delayed diagnosis of SLOS in adults and the challenges of managing congenital conditions in individuals with intellectual disabilities.
Findings
The patient exhibited self-injurious behaviors and altered pain sensation for 15 years before SLOS diagnosis.
Whole-exome sequencing confirmed Smith-Lemli-Opitz Syndrome in an adult with intellectual disability.
The case underscores the need for adult clinicians to consider congenital conditions in patients with IDD.
Abstract
Adults with intellectual and developmental disabilities (IDD) are increasingly living into adulthood, highlighting the need for adult clinicians to expand their familiarity with congenital conditions. Smith-Lemli-Opitz syndrome (SLOS) is a rare autosomal recessive inborn error of cholesterol synthesis. SLOS is commonly diagnosed in childhood, but a number of adults with IDD progress into adulthood without a formal diagnosis. We present an 18-year-old male with a history of IDD and altered pain sensation who was hospitalized following a self-inflicted knife injury resulting in a traumatic ventricular septal defect. Over the following 15 years, the patient continued to exhibit self-injurious behaviors. At the age of 33, caregivers consented to further work-up of his intellectual disability, and whole-exome genetic sequencing revealed a diagnosis of SLOS. The clinical course of this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
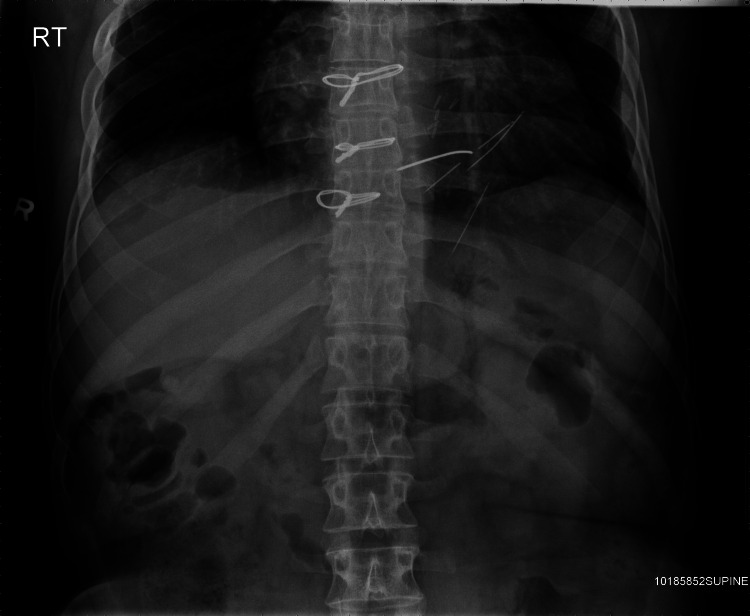 Figure 1
Figure 1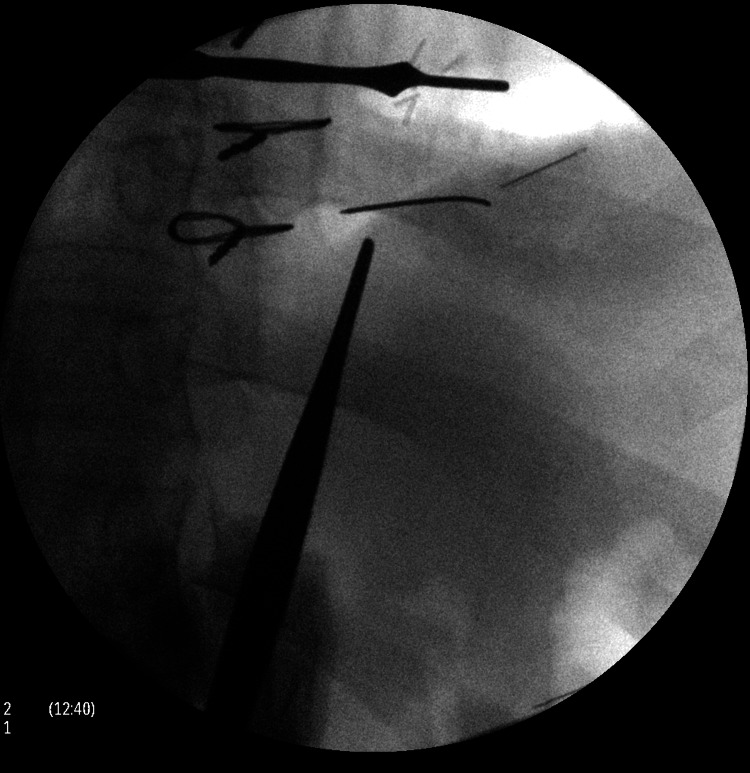 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4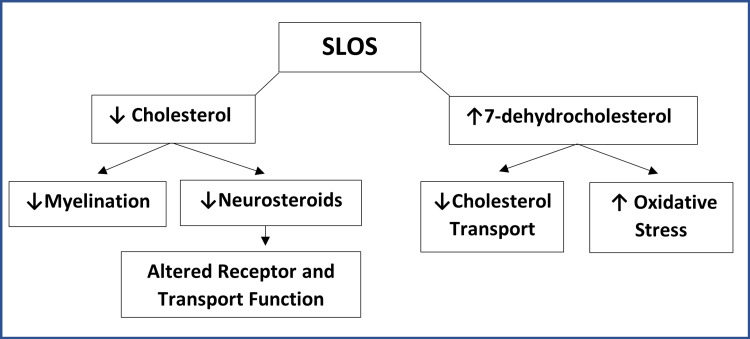 Figure 5
Figure 5| Testing Modality | Description | Clinical Use |
| Karyotype | Detects abnormalities in the count of chromosomes | Used to detect aneuploid conditions where the number of chromosomes is more or less at 46 Example: Trisomy 21 |
| Chromosomal Microarray Analysis (CMA) | Uses probes to bind to specific chromosome regions and compare to a reference | Used to detect clinically significant microdeletions or duplications Frequently used in work-up of intellectual disability and global developmental delay |
| Genetic Sequencing | Targeted gene/molecular testing sequencing | Used to analyze for a specific mutation |
| Gene panel testing | Analyzes regions in selected genes that are known to be associated with the presenting phenotype | |
| Whole exome sequence (WES) | Examines all coding regions of the genome | |
| Whole genome sequencing (WGS) | Examines the entire genome (coding and non-coding) |
| Resource | Description |
| National Resources | Disabled Peoples’ International (DPI) ( |
| State-Based Resources | NY Office for People with Developmental Disabilities (OPWDD) ( |
| Condition-Based Resources | Smith-Lemli-Opitz Foundation ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac Valve Diseases and Treatments · Diabetes Treatment and Management
Introduction
With ongoing scientific and medical advancements, more children with chronic conditions are living into adulthood. However, many young adults with childhood chronic conditions frequently encounter barriers to healthcare, including a lack of familiarity among adult clinicians and limitations of available diagnostic testing during the patient’s childhood [1,2]. As more adolescents and young adults age out of pediatric care, adult clinicians will increasingly need to care for patients with childhood-onset health conditions. One such condition is Smith-Lemli-Opitz syndrome (SLOS), a rare genetic syndrome first reported in Drs. Smith, Lemli, and Opitz’s 1964 paper describing three boys with similar congenital anomalies [3]. SLOS is characterized by mutations in 7-dehydrocholesterol reductase and may manifest through a broad range of intellectual and physical phenotypes [4]. Behavioral signs, such as poor feeding, and physical exam findings, such as syndactyly, often provide clues early in life, subsequently leading to a diagnosis. However, SLOS is occasionally not recognized until adulthood.
Case presentation
An 18-year-old male with a history of developmental delay, intellectual disability with a reported IQ of 60, a cleft palate repaired in infancy, and a prior gastrostomy tube during childhood presented with a self-inflicted penetrating stab wound to his left anterior chest in the precordial area at the mid-clavicular line with a 3-inch paring knife. He had no reported history of depression, substance use, or any other psychiatric history. Due to the altered pain sensation, the patient was reportedly attempting to stimulate his heart with the paring knife. He was emergently taken to the operating room, where a 1-centimeter right ventricular laceration was identified and repaired. A post-operative echocardiogram demonstrated a mid-septal ventricular septal defect with moderate shunting. The patient returned to the operating room on post-op day seven for a ventricular septal defect repair.
He had a previous history of self-injurious behavior that had not required surgical intervention. His family history was notable for having two brothers and an aunt with intellectual disabilities. The patient lived at home with his parents and attended high school with an individualized education plan (IEP) and 1:1 support. He was active in the band and did not consume tobacco, alcohol, or other substances.
After the patient’s ventricular septal repair, the patient continued to attempt to stimulate his heart by inserting paperclips and sewing needles through his thoracic wall into his myocardium (Figure 1). He described no pain whatsoever, but enjoyed the resulting palpitations. The patient returned again to the operating room four years later, where multiple sewing needles and a paperclip were removed from his pericardium and myocardium (Figure 2). Over the following years, the patient began inserting paperclips into his abdominal cavity. The paperclips slowly migrated through his peritoneal cavity and became embedded within his pelvic floor musculature (Figures 3, 4).
X-ray with a paperclip and sewing needle inserted in the pericardium and myocardium.
Surgical removal of the paperclip and sewing needle.
Abdominal X-ray with paperclips embedded in the pelvic floor.
Lateral X-ray with paperclips embedded in the pelvic floor.
At the age of 33, caregivers consented to further work-up of his intellectual and congenital disability, and he subsequently underwent whole-exome sequencing. This revealed two heterozygous pathogenic variants in the DHCR7 gene, which is associated with SLOS.
Placement and long-term living arrangements presented a significant challenge. After a seven-month hospitalization for safety, he was transferred to a group home with 24-hour line-of-site supervision. He has been managed medically and remains stable without further self-inflicted injuries or worsening cardiac function.
Discussion
The clinical course of this patient highlights an unusual presentation of altered pain sensation in Smith-Lemli-Opitz syndrome, delayed diagnosis into adulthood of a congenital condition, and the challenges of providing care to an individual with a severe intellectual disability. There were many factors that contributed to the delay in diagnosis. During the patient’s childhood, whole-exome genetic sequencing was not available. In addition, ethical concerns related to genetic testing were raised by the caregivers, further delaying the diagnosis. Although many patients carry a diagnosis of IDD as they enter adulthood, many, in fact, have an undiagnosed genetic condition. With the availability of new diagnostic tests, more formal diagnoses may provide additional therapeutic benefit to patients and guide their life care.
Smith-Lemli-Opitz syndrome: The patient was diagnosed with Smith-Lemli-Opitz syndrome at the age of 33 by way of whole exome sequencing. In brief, Smith-Lemli-Opitz syndrome is an autosomal recessive, multisystem syndrome caused by a deficiency of 7-dehydrocholesterol reductase, which is needed for proper cholesterol metabolism (Figure 5) [5]. The manifestations of this condition can range from mild to severe. Given the brain’s relatively higher concentration of cholesterol, neurological and behavioral manifestations are commonly seen in SLOS [5]. In the case of our patient, he had a history of developmental delay and intellectual disability throughout life (delayed gross motor skills and speech), as well as self-injurious behavior since the age of 17. While the specific pathophysiology of the self-injurious behavior and pain pathways have yet to be elucidated in SLOS, self-inflicted injury is a documented manifestation of the condition, which, for our patient, resulted in a traumatic VSD [6].
Impact of inborn errors in cholesterol synthesis (Smith-Lemli-Opitz syndrome).Adapted from "Pathogenesis SLOS", published under a Creative Commons License [7].
Genetic work-up for congenital conditions: With medical advances and the expanding availability of genetic testing, such as whole genome or whole exome sequencing, the medical community is now able to recognize and diagnose conditions that were previously attributed to an idiopathic or unknown etiology [8]. Like many adults with rare conditions and IDD, our patient had symptoms since childhood, but a formal diagnosis was not made until the age of 33, after he underwent whole-exome sequencing.
Familiarity with genetic testing is an important skill for clinicians caring for adults with conditions arising in childhood. For example, chromosomal microarray (CMA) analysis is considered the first-line genetic test for intellectual disabilities, replacing older modalities such as karyotyping and fluorescence in situ hybridization (FISH) (Table 1) [9,10]. In addition to IDD, genetic testing should also be considered to evaluate patients with conditions with known genetic associations, such as idiopathic cardiomyopathy, epilepsy, and certain types of chronic kidney disease [10-14].
With the increase in genetic testing, there is a corresponding increase in the detection of variants of uncertain significance (VUS). For genetic results that do not yield a clear diagnosis, it is important to seek the assistance of a clinical geneticist and genetic counselor. Geneticists are available at many academic medical centers, and some have created an eConsult program for primary care physicians [16].
Resources for patients with IDD: Patients with IDD and congenital disability often experience multiple systemic and social challenges throughout childhood, highlighting the importance of both early identification and early intervention [17]. With health care advances, vulnerable populations, such as those with IDD, now have life expectancies approaching those of the general population. Entering adulthood with IDD and a congenital disability, however, can present a range of challenges for adult clinicians who might be unfamiliar with some congenital conditions. Older adults with IDD are at increased risk of experiencing poor health outcomes, emphasizing the need to increase clinician comfort with IDD and congenital conditions. In addition to gaining familiarity with condition-specific recommendations, adult clinicians should avoid the pitfall of not providing age-appropriate health maintenance. Adult clinicians should also become familiar with resources available for their patients with IDD related to housing, education, and job training (Table 2). For example, the state of New York manages the State Office for People with Developmental Disabilities (OPWDD), and other states have similar programs. Given the many challenges, it is important for adult clinicians to ensure that patients are linked to appropriate services as soon as possible.
Conclusions
As more young adults age out of pediatric care, adult clinicians will be increasingly caring for patients with childhood-onset health conditions. This case of Smith-Lemli-Opitz syndrome (SLOS) highlights a rare presentation of an autosomal recessive inborn error of cholesterol metabolism. The case further highlights the challenges it poses to the adult health care system and emphasizes the need for adult clinicians to develop comfort with the diagnosis of IDD and other congenital conditions. With advances in genetic testing, our case also demonstrates the importance of understanding the typical workup and management of genetic conditions. Finally, clinicians should familiarize themselves with available local and national resources that provide support for patients with IDD and their families.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Transition planning for youth with special health care needs: results from the National Survey of Children with Special Health Care Needs Pediatrics Lotstein DS Mc Pherson M Strickland B Newacheck PW 1562156811520051593021710.1542/peds.2004-1262 · doi ↗ · pubmed ↗
- 2Healthcare system supports for young adult patients with pediatric onset chronic conditions: a qualitative study J Pediatr Nurs Szalda DE Jimenez ME Long JE Ni A Shea JA Jan S 1261323020152545043910.1016/j.pedn.2014.09.015PMC 8884029 · doi ↗ · pubmed ↗
- 3A newly recognized syndrome of multiple congenital anomalies J Pediatr Smith DW Lemli L and Opitz JM 2102176419641411952010.1016/s 0022-3476(64)80264-x · doi ↗ · pubmed ↗
- 4Smith-Lemli-Opitz syndrome: pathogenesis, diagnosis and management Eur J Hum Genet Porter FD 5355411620081828583810.1038/ejhg.2008.10 · doi ↗ · pubmed ↗
- 5Smith-Lemli-Opitz Syndrome In: Adam MP, Feldman J, Mirzaa GM, et al., editors. Gene Reviews® [Internet] Nowaczyk MJM Wassif CA Seattle University of Washington 1998 [updated 2020]https://www.ncbi.nlm.nih.gov/books/NBK 1143/20301322 · pubmed ↗
- 6Smith-Lemli-Opitz syndrome 2023 https://en.wikipedia.org/wiki/Smith%E 2%80%93Lemli%E 2%80%93Opitz_syndrome
- 7Cognitive and behavioral aspects of Smith-Lemli-Opitz syndrome Am J Med Genet C Semin Med Genet Diaz-Stransky A Tierney E 295300160 C 20122304258510.1002/ajmg.c.31342 · doi ↗ · pubmed ↗
- 8Shortcutting the diagnostic odyssey: the multidisciplinary Program for Undiagnosed Rare Diseases in adults (UD-Pr OZA)Orphanet J Rare Dis Schuermans N Hemelsoet D Terryn W 2101720223560676610.1186/s 13023-022-02365-y PMC 9128245 · doi ↗ · pubmed ↗