Single-nephron assessment of urate excretion in patients with IgA nephropathy
Hirokazu Marumoto, Nobuo Tsuboi, Takaya Sasaki, Yusuke Okabayashi, Kotaro Haruhara, Go Kanzaki, Kimiyoshi Ichida, Takashi Yokoo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
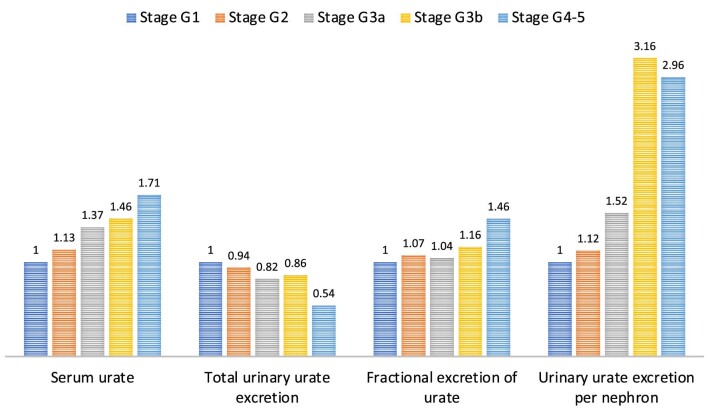 Figure 1
Figure 1- —JSPS10.13039/501100001691
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGout, Hyperuricemia, Uric Acid · Renal Diseases and Glomerulopathies · Pediatric Urology and Nephrology Studies
To the Editor,
Hyperuricemia and abnormal urate excretion are thought to be involved in the progression of chronic kidney disease (CKD). Among the causative diseases of CKD, immunoglobulin A nephropathy (IgAN) has been the most extensively studied in relation to blood urate levels [1, 2]. Although hyperuricemia was initially considered a poor prognostic factor for IgAN, recent large-scale studies have reported its limited sensitivity in certain populations, including men, the elderly and patients with an impaired kidney function or advanced tubulointerstitial injury (S1, S2).
We recently established a method to estimate the total nephron number in clinical practice and reported nephron number estimates in patients with IgAN [3]. As a subanalysis of our data, we estimated the urinary urate excretion per nephron in patients with IgAN. Single-nephron urate excretion was calculated by dividing the total urinary urate excretion by the number of non-globally sclerotic glomeruli in both kidneys and was compared among CKD stage groups. The detailed methods for patient selection and nephron number measurements are described in the Supplementary Methods.
This retrospective study included 158 adult Japanese patients who underwent native kidney biopsy and who were diagnosed with primary IgAN at Jikei Hospital, Tokyo, between 2007 and 2017. The clinicopathological and morphometric findings of the patients are summarized in Supplementary data, Table S1. The mean age was 39.0 years, and 95 (60.5%) patients were male. As CKD stages advance, patients tend to be older, and to have more systemic hypertension, heavier proteinuria and more severe chronic histopathological lesions, including interstitial fibrosis/tubular atrophy. In the CKD stages G1, G2, G3a, G3b and G4–5 groups, the average single-nephron urate excretion was 0.25, 0.28, 0.38, 0.79 and 0.74 ng/mg creatinine, respectively. Figure 1 shows the fold-differences in uric acid–related parameters among the CKD stage groups relative to CKD stage G1 as the reference. In this study population, conventionally used uric acid–related parameters, such as serum urate, total urinary urate excretion and fractional excretion of urate, showed only modest changes with advancing CKD stages. In contrast, single-nephron urate excretion was markedly increased in patients with stage G3b or more advanced CKD stages, even though compensatory excretion from the intestinal tract is expected to increase in these patients (S3, S4).
A biopsy study showed a close relationship between serum urate levels in patients with IgAN and periglomerular arteriolar hyalinosis, suggesting that serum urate disrupts the arteriolar autoregulatory function and induces glomerular hyperperfusion injury (S5). Another clinical study demonstrated that hyperuricemia was independently associated with the progression of tubulointerstitial lesions in patients with IgAN [4]. However, the mechanisms by which urate exposure to tubules promotes kidney disease progression remain to be fully elucidated. A previous study showed that urate induces epithelial–mesenchymal transition of kidney tubular cells in vitro in a dose-dependent manner [5]. This suggests that urate exposure to tubules may induce direct cell injury under certain circumstances in which urate is abnormally and constitutively concentrated in the tubulointerstitium. The elevated single-nephron urate levels in IgAN patients with advanced CKD may represent part of the pathophysiological abnormalities of urate dynamics in the tubulointerstitium. A major limitation of this cross-sectional study was the difficulty in referring to causal relationships. Further studies, including validation of progressive kidney diseases other than IgAN, are warranted.
In conclusion, we evaluated urinary urate excretion per nephron in IgAN patients and showed markedly concentrated levels of single-nephron urate in patients with advanced CKD. Clinical assessment of single-nephron excretion of a certain molecule, as demonstrated for urate in this study, may be a promising tool for elucidating the pathophysiology of human kidney diseases, such as IgAN, in which nephron mass reduction is a common feature of disease progression.
Supplementary Material
sfae036_Supplemental_File
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Syrjänen J, Mustonen J, Pasternack A. Hypertriglyceridaemia and hyperuricaemia are risk factors for progression of Ig A nephropathy. Nephrol Dial Transplant 2000;15:34–42. 10.1093/ndt/15.1.3410607765 · doi ↗ · pubmed ↗
- 2Ohno I, Hosoya T, Gomi H. et al. Serum uric acid and renal prognosis in patients with Ig A nephropathy. Nephron 2001;87:333–9. 10.1159/00004593911287777 · doi ↗ · pubmed ↗
- 3Marumoto H, Tsuboi N, D'Agati VD. et al. Total nephron number and single-nephron parameters in patients with Ig A nephropathy. Kidney 360 2021;2:828–41. 10.34067/KID.000697202035373063 PMC 8791345 · doi ↗ · pubmed ↗
- 4Myllymäki J, Honkanen T, Syrjänen J. et al. Uric acid correlates with the severity of histopathological parameters in Ig A nephropathy. Nephrol Dial Transplant 2005;20:89–95. 10.1093/ndt/gfh 58415572382 · doi ↗ · pubmed ↗
- 5Ryu ES, Kim MJ, Shin HS. et al. Uric acid-induced phenotypic transition of renal tubular cells as a novel mechanism of chronic kidney disease. Am J Physiol Renal Physiol 2013;304:F 471–80. 10.1152/ajprenal.00560.201223283992 · doi ↗ · pubmed ↗