Vaccination status, incidence of adverse events, and awareness of COVID-19 vaccine among outpatients undergoing chemotherapy
Satoshi Iwakawa, Takuya Azechi, Orie Saigo, Ryunosuke Imai, Ayumi Nakai, Shoji Koshiba, Uki Saito, Kota Asakura, Kuniyoshi Sato, Toshimi Kimura

TL;DR
This study examines vaccination rates and concerns among cancer patients receiving chemotherapy, finding high vaccination rates but lingering worries about timing and safety.
Contribution
The study provides new insights into vaccination status and adverse events among cancer patients, highlighting the role of pharmacists in addressing concerns.
Findings
96.7% of surveyed cancer patients received two doses of the COVID-19 vaccine.
Common adverse events included injection site pain, fever, and fatigue.
Most patients consulted primary care physicians, but few sought advice from pharmacists.
Abstract
Cancer has been identified as a risk factor for severe illness and mortality in coronavirus disease (COVID-19), underscoring the importance of recommending COVID-19 vaccinations to patients with cancer. However, few reports have focused on the vaccination status and the incidence of adverse events among patients with cancer. In this study, we aimed to evaluate the vaccination status, incidence of adverse events, concerns, and anxiety related to COVID-19 vaccination among patients with cancer. In addition, we explored the utilization of information sources by these patients and the ease of use. A survey was conducted among outpatients undergoing chemotherapy who received medication counseling from a pharmacist at Juntendo University Hospital. Responses were gathered from 60 out of the 143 participants. Of the respondents, 96.7% had received two doses of the COVID-19 vaccine. Common…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
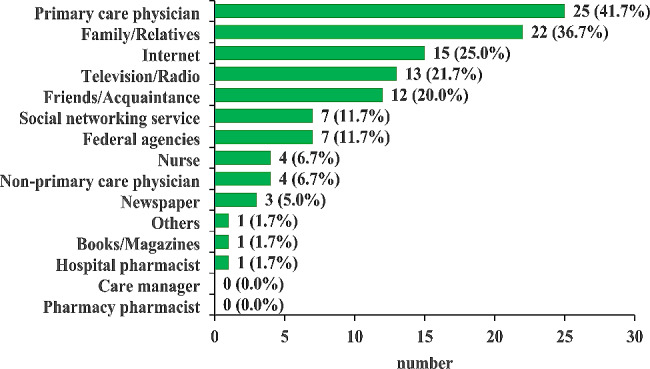 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Vaccine Coverage and Hesitancy · Hepatitis B Virus Studies
Background
Vaccination contributes to reducing the mortality and incidence rates of various infectious diseases, such as eradicating smallpox, representing one of the greatest achievements in public health [1]. In the context of coronavirus disease (COVID-19), in addition to preventive measures centered on standard precautions, the development and widespread administration of vaccines are essential to prevent the spread of the disease [2]. Since the approval of COVID-19 vaccines in February 2021, Japan has employed several of these vaccines [3–5]. Although vaccination has decreased the risk of infection and severe illness, the emergence of mutant viruses has fueled the persistence of COVID-19. In May 2022, a fourth dose of the vaccine was administered to older people and individuals with underlying health conditions. The fifth dose of the vaccine was initiated in September 2023, indicating the need for continuous COVID-19 vaccine administration [6].
Because cancer is cited as a risk factor contributing to the mortality and severity of COVID-19, vaccination is recommended for patients with cancer [7, 8]. However, few reports have focused on the vaccination status and the incidence of adverse events among patients with cancer. Concerns about vaccine-related adverse events, uncertainties regarding the efficacy and safety of vaccines, and skepticism about the rapid development of vaccines constitute major reasons for hesitancy toward COVID-19 vaccination [9]. When patients with cancer experience anxiety or concerns about vaccination, they access various sources of information to address their concerns. Because incorrect information may be obtained depending on the information source, the involvement of healthcare professionals is important to alleviate these concerns. However, there have been insufficient reports on anxiety and concerns in patients with cancer, the information sources they access, and their interactions with healthcare professionals.
In this study, we aimed to clarify the vaccination status and the incidence of adverse events related to COVID-19 vaccination among patients with cancer. In addition, we elucidated the anxiety and concerns of patients with cancer regarding COVID-19 vaccination, consultation channels, information sources before vaccination, and their ease of utilization among patients with cancer.
Materials and methods
Study design and participants
This study was a cross-sectional, web-based, anonymous questionnaire survey designed to clarify the COVID-19 vaccination rate, adverse event occurrences, anxiety and concerns about COVID-19 vaccination, usage and ease of consultation channels, and information sources among patients with cancer. This survey was conducted among outpatients undergoing chemotherapy who received medication counseling from the pharmacist at Juntendo University Hospital from October 1, 2022, to January 31, 2023. In this hospital, five pharmacists with specialized or certified qualifications related to cancer treatment are employed at a time. Among them, one pharmacist is dedicated daily to providing medication counseling services to outpatients with cancer. After the pharmacist provided information regarding the purpose of the survey and guidance on the online questionnaire was given, participants accessed the survey. The details of the survey items are shown in Additional file 1. Each survey item was collectively devised based on multiple information sources and reports concerning adverse events [4, 5, 10, 11] by the co-authors who are experienced and certified pharmacists specializing in cancer chemotherapy. Thereon, the questionnaire was finalized after consultation with pharmacists specialized in infection control.
Data analysis
Data were collected using Questant software, an online questionnaire program (Macromill Inc., Tokyo, Japan). Simple tabulation and statistical analysis were performed using the JMP pro 17 (SAS Institute, Cary, NC, USA). A scoring system was implemented to compare the ease of utilizing consultation channels and information sources as a reference for COVID-19 vaccination. Each answer was given a specific score; “Very easy to consult/utilize” = 5, “Easy to consult/utilize” = 4, “Neutral” = 3, “Difficult to consult/utilize” = 2, “Very difficult to consult/utilize” = 1, and " Not involved” = 0. The averages and standard deviations for each item were calculated. To compare the average value of each item with “hospital pharmacist” as the control, a Dunnett’s test was performed. Statistical significance was set at a P level of < 0.05.
Results
Respondent background and the reasons for non-vaccination
The response rate to the questionnaire was 42.0% (60/143 patients undergoing chemotherapy). The demographic and clinical characteristics of the participants are summarized in Table 1 and Additional file 2. Notably, 97% of the respondents received two doses of the COVID-19 vaccine. Moreover, 21.7% of the respondents contracted COVID-19 after receiving the vaccine. Table 2 lists the reasons for non-vaccination. A common response for missing the third and fourth vaccine doses was “Schedule did not match.” Additionally, for missing the fourth dose, the most frequently received response pertained to “Interaction with current medications.” In addition, the “Others” category included responses indicative of plans for future COVID-19 vaccination.
Table 1. Demographic and clinical characteristics of the participantsNumber%SexMale1626.7Female4473.3Age (years)< 4035.040–491525.050–592135.060–691321.770–79813.3≥ 8000.0HistoryAllergy915.0Experience of feeling unwell after receiving some vaccine58.3VaccinationstatusNever23.31st dose5896.72nd dose5896.73rd dose4778.34th dose2135.0CancerstageStage 000.0Stage I915.0Stage II1321.7Stage III1321.7Stage IV1321.7Unknown1220.0Duration of cancertreatment< 1 years4473.31–5 years915.06–10 years58.3≥ 11 years23.3History of COVID-19Have a history of COVID-19 without the vaccination00.0Have a history of COVID-19 before vaccination23.3Have a history of COVID-19 after vaccination1220.0Have a history of COVID-19 both before and after vaccination11.7No history of COVID-194575.0COVID-19, coronavirus disease
Table 2. Reasons for non-COVID-19 vaccination and interruption of COVID-19 vaccination1st doseConcerns about safety, such as severe adverse events1Unknown evidence about its effectiveness0Unknown relief services for adverse health effects0Unknown medical procedure for a severe allergic reaction0No habit of vaccinations such as flu0Not recommended by my friend0Unable to receive vaccination due to allergy status0Chronic disease0Interaction with current medications0Schedule did not match1Others02nd does3rd dose4th doseThe adverse events were intolerable021I did not feel the effectiveness of the vaccination000I had allergic symptoms000Vaccination impaired physical and mental health011Not recommended by my friend010Chronic disease010Interaction with current medications017Schedule did not match044Others0413Numbers in the table indicate the number of respondentsCOVID-19, coronavirus disease
Basic knowledge and awareness of COVID-19 vaccination
Table 3 shows the results of the responses regarding basic knowledge and awareness of COVID-19 vaccination. A significant 72% of the respondents believed that COVID-19 vaccines alleviate symptoms of COVID-19, and no respondents answered: “COVID-19 vaccines completely prevent COVID-19.” Nearly half of the respondents expressed concerns about ongoing cancer treatments or surgeries and questioned the appropriate timing for vaccination. Furthermore, 20% of the respondents answered “no specific concerns.”
Table 3. ReasonsBasic knowledge and awareness of COVID-19 vaccination in cancer patientsNumber%COVID-19 vaccine’s efficacyCOVID-19 vaccines completely prevent COVID-1900.0COVID-19 vaccines are highly effective in preventing COVID-192846.7COVID-19 vaccines tend to alleviate the symptoms of COVID-194371.7Vaccination provides sustained protection against COVID-19–associated serious complications2440.0Mass infections (cluster infections) can be prevented by the vaccination915.0Nothing applies46.7Concerns regarding COVID-19 vaccineMay be ineffective or poor response because of cancer11.7Cancer may get worse1118.3COVID-19 vaccines may cause COVID-19 in patients with weekend immune system1525.0When should I get vaccinated if I am scheduled for cancer treatment or surgery?2948.3Probability of cancer-specific adverse events2440.0Increasing adverse events than the other people such as pain at the vaccination site1118.3Possibility of vaccination for the people in the developed an allergy to chemotherapy00.0Possibility of reducing the effectiveness of cancer treatment by vaccination711.7Possibility of interruption of cancer chemotherapy1321.7Which vaccine should I choose?46.7Are the vaccines safe?1423.3No specific concerns1220.0COVID-19, coronavirus disease
Adverse events of COVID-19 vaccination
Table 4 shows the profiles of adverse events of COVID-19 at each dose. Irrespective of the dose, the most prevalent adverse event was localized pain at the injection site. Regarding systemic symptoms, fever, and fatigue rates were higher than other symptoms at each dose. Most respondents reported that their schedules for cancer treatment were unaffected.
Table 4COVID-19 vaccination profile and adverse events in cancer patients1st dose2nd dose3rd dose4th doseNumber%Number%Number%Number%Type of vaccinationsPfizer4374.14679.32859.61571.4Moderna1424.11119.01940.4628.6AstraZeneca00.000.000.000.0Others00.000.000.000.0I do not know /I do not remember11.711.700.000.0Not answer00.000.000.000.0Impact on cancer treatment scheduleYes35.200.012.114.8No5493.15696.64493.61990.5Not answer11.723.424.314.8Presence of adverse eventsShock/Anaphylaxis00.000.000.000.0Pain at the injection site2339.72136.21838.3628.6Swelling at the infection site1017.21017.2919.1419.0Redness/erythema at the injection site11.723.412.114.8Headache58.658.624.314.8Diarrhea00.000.000.000.0Muscle pain1017.21017.2612.814.8Joint pain610.3610.3612.814.8Fatigue1322.41322.41021.3314.3Cold58.658.6612.800.0Fever (over 37.5ºC)2136.21729.31327.7314.3None2746.62848.32451.11466.7COVID-19, coronavirus disease
Consultation channels and information sources used for COVID-19 vaccination
Figure 1 shows the utilization pattern of consultation channels and information sources related to COVID-19 vaccination. The top three channels/sources with notably high response rates as consulted references were “primary care physician,” “family/relatives,” and “Internet.” No responses indicated consultation with a “pharmacy pharmacist,” and only one respondent consulted a “hospital pharmacist.” Table 5 shows the ease of utilizing consultation channels and information sources related to COVID-19 vaccination. When ranking the ease of utilization for each consultation channel or information tool, “family members/relatives” were most accessible, which was statistically higher than “hospital pharmacists.” Furthermore, among healthcare professionals, “primary care physicians” were the most accessible; however, no statistically significant difference was observed in the average compared to “hospital pharmacists.” On the other hand, “pharmacy pharmacists” displayed a tendency towards lower average value compared to “hospital pharmacists,” although no statistically significant difference was noted.
Fig. 1. Utilization patterns of consultation channels and information sources
Table 5. Ease of utilizing consultation channels and information sourcesConsultation channelsand information sourcesEase of utilizing consultation channels and information sourcesAveragescoreStandarddeviationp-valueVeryeasyEasyNeutralDifficultVerydifficultNotinvolvedHospital pharmacist16121401172.851.98-Pharmacy pharmacist972011222.271.900.381Primary care physician25141010103.551.780.184Non-primary care physician8102042162.501.760.911Nurse21111320133.201.890.911Care manager52500480.801.67< 0.001Family/Relatives3117111004.300.83< 0.001Friends/Acquaintance1420151283.321.600.660Federal agencies342320281.731.720.004Television/Radio242911231.931.620.031Newspaper142221301.531.620.000Books/Magazines152401291.631.660.001Internet6132411152.621.690.996Social networking service472332212.081.710.113 Statistical differences compared to Hospital pharmacist as a control were determined by Dunnett’s test
Discussion
Several surveys in the general population have shown that the frequency of adverse events of COVID-19 vaccine, such as fever and fatigue, increased after the second dose compared with the first dose [4, 12]. However, we found that the incidence of fever after the first dose in patients with cancer was higher than that in a previous report and was almost the same as that of the second vaccination. Although the individual clinical course of the respondents is unknown because of the anonymous questionnaire used in this study, factors other than vaccine-related adverse events, such as fever with febrile neutropenia after chemotherapy, might be involved. It is difficult to distinguish between these factors that lead to fever after vaccination; since febrile neutropenia necessitates urgent intervention, patients with cancer need to know what to do if they have a fever after receiving the COVID-19 vaccination.
COVID-19 vaccination is recommended for patients with cancer because of the high risk of mortality and the severity associated with a compromised immune response during chemotherapy [7, 8]. A systematic review and meta-analysis reported that female sex and chemotherapy were significant factors associated with COVID-19 vaccination hesitancy in patients with cancer [9]. However, most of the respondents in this study had received two or more doses of the COVID-19 vaccine at the time of their responses, demonstrating a vaccination rate higher than the overall vaccination rate in Japan [13]. Over half of the respondents acknowledged the infection prevention and severity mitigation effects of COVID-19 vaccination, leading them to believe in the vaccine’s efficacy and receive it. Additionally, 41.7% of the respondents cited their “primary care physician” as the consultation source, suggesting that communication with physicians might have influenced their decision to be vaccinated.
Regarding the effectiveness of the COVID-19 vaccination, some respondents indicated a lack of correct understanding of the low response rates for herd immunity (15%) and a misunderstanding of the potential cause of COVID-19 post-vaccination (25%). These findings suggest that the respondents did not understand the efficacy of COVID-19 vaccination in patients with cancer. Continuous dissemination of information regarding the utility of COVID-19 vaccination in patients with cancer is crucial.
Even after vaccination, it is well known that people continue to have some anxiety and concern about the vaccine [14]. This survey also confirmed that 80% of the respondents had anxiety or concerns about COVID-19 vaccination. Regarding the timing of COVID-19 vaccination that showed the highest response as a concern in this study and other reports [15], the Japanese Society of Clinical Oncology recommends the time period when it is better to avoid COVID-19 vaccination [8]. Considering the latest domestic and international evidence, information regarding vaccination timing is deemed beneficial for endorsing the COVID-19 vaccination. Furthermore, approximately 20–40% of the respondents in this study expressed concerns about the incidence of adverse events, unique adverse events, and the safety of the COVID-19 vaccine. Given that concerns about vaccine-related adverse events can be a deterrent to vaccination [16], providing healthcare professionals with information on adverse events is crucial. Compared with other survey reports [4, 12, 17], this survey found no higher incidence of adverse events or unique adverse events regardless of the number of COVID-19 vaccine doses administered, except for a tendency toward more frequent fevers after the first dose. Additionally, this study has identified concerns of patients with cancer regarding COVID-19 vaccine interactions with current medications, and post-vaccination fever in relation to COVID-19 vaccination. Generally, while antipyretics are the first choice for fever management after vaccination, fever following chemotherapy may require appropriate intervention, and the approach may vary. However, our institution lacks guidelines pertaining to fever management. Additionally, although there are risks such as bleeding at the administration site due to antithrombotic agents, there are no explicit recommendations regarding interactions with concomitant medications. Patients undergo vaccination based on the discretion of their attending physicians. To potentially enhance vaccination rates, it may be necessary to establish institutional regulations concerning fever management and interactions between the vaccine and current medicines.
Additionally, there was no difference in the occurrence of adverse events related to COVID-19 vaccination based on the presence or absence of chemotherapy [18]. While many uncertainties remain regarding the long-term safety of COVID-19 vaccination, these findings suggest that patients with cancer can safely receive the vaccine, similar to healthy individuals. Communicating this lack of significant differences in adverse reactions between patients with cancer and the general population can be valuable in allaying concerns. Furthermore, this survey obtained responses citing the severity of adverse events and health damage as reasons for interrupting COVID-19 vaccination. For patients with cancer, it is necessary to assess the feasibility of continuing COVID-19 vaccination from a medical and pharmaceutical perspective, along with implementing interventions, such as proposing medications for symptom relief, to enhance vaccination rates.
Prospective vaccine recipients gather and evaluate information from various sources to address their anxieties and concerns. Telephone interview surveys showed that physicians (77.6%) and federal agencies (50.5%) were highly trusted sources of information on the COVID-19 vaccine, whereas family members (25.9%) and social media (3.8%) were deemed less reliable [19]. People relying on family/friends, faith-based organizations, or social media for healthcare information tend to be hesitant about getting vaccinated [20]. However, even with these information sources considered to be unreliable, our study indicated a high percentage of respondents who utilize “family/acquaintance” and “social networking service” as the source of consultation and information. Conversely, workplaces/schools, LINE (a communication tool like WhatsApp and iMessage highly popular in Japan), and social media sources have encouraged citizens to receive the COVID-19 vaccine [21]. Although the impact of information sources on vaccination intention was not thoroughly examined in this study, it is plausible that consultations with family/friends and the use of social media could have contributed to the high COVID-19 vaccination rates. Continuous research is essential to understand the influence of various information sources on patients with cancer who intend to receive the COVID-19 vaccine.
Consultation with “primary care physicians” was the most common response in this study. This underscores the significance of primary care physicians for patients with cancer in making decisions regarding vaccination feasibility, considering the impact on cancer treatment, vaccination schedules, and existing health conditions. Notably, only one respondent mentioned pharmacists in the survey, indicating a perception of no involvement of pharmacy/hospital pharmacists compared to other healthcare professionals, making them less utilized as consultation channels, possibly because of limited communication opportunities compared to other professions. Particularly in our institution, pharmacist’s interventions for the patients with cancer are primarily focused on the initial and second treatments, with limited opportunities for sustained interventions. Consequently, there are few occasions for pharmacists to engage in communication with the patients with cancer, potentially resulting in lower contact with pharmacists compared to other healthcare professionals. In addition, the low response rate of 42.0% in this study can be attributed to the scarcity of communication opportunities with pharmacists, along with the possibility that some elderly individuals are less proficient in operating tablet devices such as smartphones. Consultations with primary care physicians may have resolved patient’s concerns about COVID-19 vaccination, making consultations with other healthcare professionals unnecessary. However, some respondents in this study still harbored concerns about the COVID-19 vaccination, indicating that unresolved anxieties and worries might persist despite consulting primary care physicians.
In this survey, “hospital pharmacist” was among the easiest to approach, following primary care physicians and nurses. This could be attributed to the trust established through medication counseling and adverse event monitoring during outpatient chemotherapy. With the promotion of designated pharmacies and advanced pharmaceutical management functions, pharmacists are expected to build better relationships with patients with cancer, enhancing the ease of consultation. Pharmacists with an established trust could potentially address the unresolved concerns of patients with cancer, proving invaluable for the continued promotion of COVID-19 vaccination. Since utilization of our hospital as a consultation point is limited, we believe that fostering a trustful relationship with patients with cancer is crucial. This can be achieved by pharmacists conducting sustained interventions and increasing opportunities for communication with cancer patients. A detailed exploration of patient anxieties regarding the COVID-19 vaccine and assessment of pharmacist interventions is crucial for future research.
The limitation of this study may impose difficulty in generalizing our findings and conclusions. The survey was conducted within a single hospital, and the sample size was small. Additionally, there is a significant bias towards cancer types (shown in an Additional file 2), and the participants in this survey may not fully represent the entirety of patients with cancer. Moreover, we did not confirm the treatment regimens and the timing of chemotherapy of patients with cancer. Therefore, the effects of these factors on the purpose of this study could not be evaluated. Although definitive conclusions are challenging, valuable insights were gained to consider the necessary interventions to foster the ongoing acceptance of COVID-19 vaccine administration among patients with cancer.
Conclusions
The high vaccination rate among patients with cancer indicates that they can receive the COVID-19 vaccine with the same level of safety as patients without cancer. Furthermore, while patients with cancer engage in COVID-19 vaccination consultations primarily with their primary care physicians, they may harbor some form of apprehension. However, access to pharmacists for administering the COVID-19 vaccine to patients with cancer is limited, highlighting the potential for pharmacist intervention. It is essential to explore pharmacist intervention methods to promote continuous vaccination against COVID-19, thereby maintaining and enhancing the quality of life of patients with cancer.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Additional file 1: Survey items
Additional file 2: Cancer type and use of immune checkpoint inhibitor of the respondents
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Centers for Disease Control and Prevention (CDC)Ten great public health achievements–United States, 1900–1999 MMWR Morb Mortal Wkly Rep 199948241310220250 · pubmed ↗
- 2Farsalinos K Poulas K Kouretas D Vantarakis A Leotsinidis M Kouvelas D Improved strategies to counter the COVID-19 pandemic: Lockdowns vs. primary and community healthcare Toxicol Rep 202181910.1016/j.toxrep.2020.12.00133294384 PMC 7713637 · doi ↗ · pubmed ↗
- 3Oliver SE Gargano JW Marin M Wallace M Curran KG Chamberland M The Advisory Committee on Immunization practices’ interim recommendation for use of Pfizer-Bio N Tech COVID-19 vaccine– United States, December 2020 MMWR Morb Mortal Wkly Rep 2020691922410.15585/mmwr.mm 6950 e 233332292 PMC 7745957 · doi ↗ · pubmed ↗
- 4Polack FP Thomas SJ Kitchin N Absalon J Gurtman A Lockhart S Safety and efficacy of the BNT 162b 2 m RNA Covid-19 vaccine N Engl J Med 202038326031510.1056/NEJ Moa 203457733301246 PMC 7745181 · doi ↗ · pubmed ↗
- 5Heath PT Galiza EP Baxter DN Boffito M Browne D Burns F Safety and Efficacy of NVX-Co V 2373 Covid-19 vaccine N Engl J Med 202138511728310.1056/NEJ Moa 210765934192426 PMC 8262625 · doi ↗ · pubmed ↗
- 6Ministry of Health., Labour and Welfare of Japan. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/vaccine_00184.html. Accessed November 28 2023.
- 7Kuderer NM Choueiri TK Shah DP Shyr Y Rubinstein SM Rivera DR Clinical impact of COVID-19 on patients with cancer (CCC 19): a cohort study Lancet 202039519071810.1016/S 0140-6736(20)31187-932473681 PMC 7255743 · doi ↗ · pubmed ↗
- 8Japanese Society of Medical Oncology. https://www.jsmo.or.jp/news/coronavirus-information/qa_vaccinel_3gakkai.html. Accessed November 28 2023.