Moyamoya Syndrome: Differential Diagnosis in Patients With Central Nervous System Symptoms and Hyperthyroidism
Yosuke Maezawa, Kazuya Nagasaki, Hitoshi Aiyama, Yuki Yamamoto, Yasushi Shibata

TL;DR
This paper reports a rare case of moyamoya syndrome caused by Graves' disease, highlighting the importance of considering underlying conditions during diagnosis.
Contribution
The paper presents a novel case linking moyamoya syndrome with Graves' disease and emphasizes the need for differential diagnosis.
Findings
Moyamoya syndrome was diagnosed in a patient with Graves' disease and central nervous system symptoms.
Treating the underlying Graves' disease resolved the patient's moyamoya-related symptoms.
The case underscores the importance of identifying primary illnesses in moyamoya syndrome diagnosis.
Abstract
Moyamoya syndrome, known as secondary moyamoya disease, is associated with various primary illnesses, such as brain tumor, meningitis, autoimmune disease, and thyrotoxicosis, and their relations are not clear. We report a rare case of moyamoya syndrome in a patient with Graves' disease. An 18-year-old woman was admitted to our hospital due to convulsions. She had symptoms of palpitations and fatiguability for half a year and transient numbness in her left upper extremity and dysarthria for a month. In physical findings, tachycardia and diffuse thyroid swelling were noted. A blood test revealed thyrotoxicosis and antithyroid antibody, and a diagnosis of Graves' disease was obtained. Brain magnetic resonance imaging (MRI) showed bilateral internal carotid artery occlusion. We finally diagnosed the patient with moyamoya syndrome caused by Graves' disease. Moyamoya disease or syndrome can…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
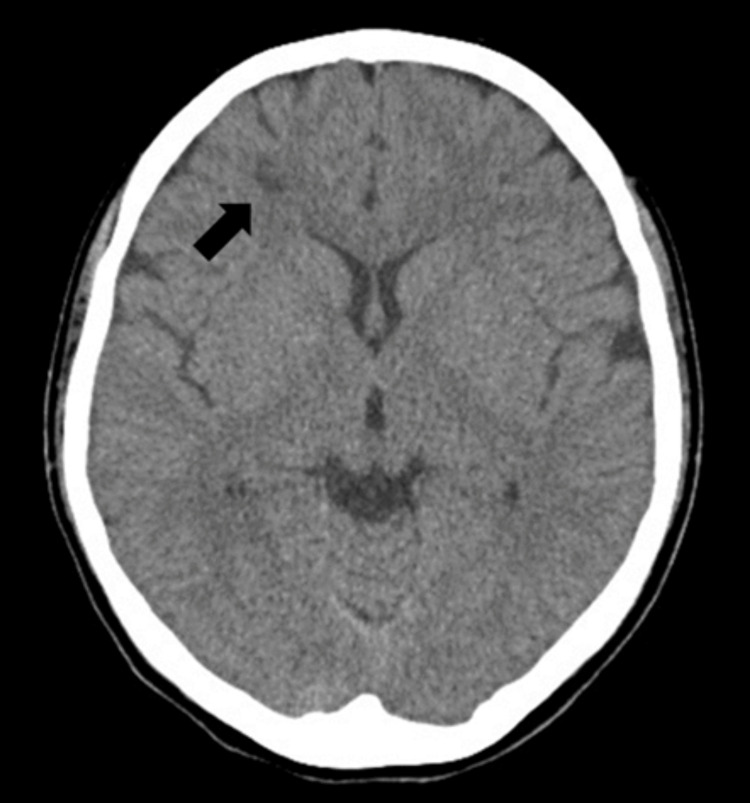 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMoyamoya disease diagnosis and treatment · Neurological Complications and Syndromes · Intracranial Aneurysms: Treatment and Complications
Introduction
Moyamoya disease (cerebrovascular "moyamoya" disease) causes chronic progressive narrowing in the terminal parts of both internal carotid arteries, forming an abnormal vascular network in the base of the brain, known as the "moyamoya vessels." Generally, it refers to cases without an underlying disease. However, cases with underlying diseases, including Graves' disease and systemic lupus erythematosus, are referred to as moyamoya syndrome [1,2]. The prevalence of moyamoya syndrome in patients with Graves' disease is reported to be 0.0454% [3], making it relatively rare. Therefore, we report a case of moyamoya syndrome associated with Graves' disease in an 18-year-old female.
Case presentation
An 18-year-old Japanese woman presented to our emergency department (ED) with a sudden loss of consciousness, which she regained after 15 min. She had experienced palpitations, increased appetite, and fatigue over the last six months. Physical examination revealed tachycardia (137 bpm) but no focal neurological symptoms. Cranial computed tomography (CT) revealed two low-density areas in the right frontal lobe (Figure 1). We suspected multiple sclerosis or brain tumors; therefore, the patient was discharged from the ED and scheduled for the outpatient clinic.
Computed tomography revealed two low-density areas in the right frontal lobe (black arrow).
Subsequently, the patient developed generalized seizures and immediately returned to the ED. Diazepam (10 mg) and fosphenytoin (1125 mg) were administered intravenously, and the seizures stopped within five minutes. She had a blood pressure of 148/80 mmHg, a pulse rate of 118 bpm, a respiratory rate of 19 breaths per minute, oxygen saturation of 100% in room air, and a body temperature of 37.5°C. Physical examination revealed a goiter and blood tests showed elevated free T3 (>20.0 pg/mL) and free T4 (3.58 ng/dL) levels and low thyroid-stimulating hormone (TSH) levels (0.00 μIU/mL). The patient was admitted for the management of seizures and hyperthyroidism. A positive anti-TSH receptor antibody test confirmed Graves' disease and thiamazole was started. The patient experienced no convulsive or ischemic attacks and recovered to normal status during hospitalization. She was discharged on the sixth hospital day.
Post-discharge, cranial magnetic resonance imaging (MRI) revealed obstruction of the bilateral internal carotid arteries and a hazy appearance in the surrounding blood vessels (Figure 2), resulting in the diagnosis of moyamoya syndrome associated with hyperthyroidism. The two low-density areas in right frontal lobe detected in the brain CT at the ED were consistent with high signals on fluid attenuated inversion recovery (FLAIR), diffusion-weighted imaging (DWI), and T2-weighted images and low signals on T1-weighted images. From these findings, the lesions were suspected of being old infarctions. We suspected that her seizures and ischemic attacks were ischemic symptoms of moyamoya syndrome. We continued to treat Graves' disease and maintained her euthyroid status. There was no relapse of seizures in the year following discharge.
Magnetic resonance angiography showed obstruction of the bilateral internal carotid arteries (white arrows) and a hazy appearance in the surrounding blood vessels.
Discussion
Moyamoya syndrome is associated with various congenital disorders and acquired diseases [1,2]. The prevalence of moyamoya syndrome in patients with Graves’ disease was reported to be 45.36 per 100,000 patients (0.0454%) [3].
Its clinical features can be divided into ischemic and hemorrhagic symptoms, clinically similar to primary moyamoya disease [4]. In moyamoya syndrome associated with hyperthyroidism, it may be challenging to differentiate moyamoya disease and thyroid crisis. These diseases present with central nervous system (CNS) symptoms, such as disturbance of consciousness and seizures. Despite that, in our case, no apparent end-organ damage was observed, indicating that the patient’s symptoms may have been associated with moyamoya syndrome and not thyroid crisis.
Previous studies have reported that hyperthyroidism may cause moyamoya disease because it increases cerebral oxygen consumption and blood flow, resulting in damage to blood vessel walls, sympathetic regulation causing cerebral vascular stenosis [5] and immune stimulation of the thyroid gland being involved in T cell function causing vascular abnormalities [6,7]. In moyamoya syndrome with Graves’ disease, it has been reported that normalization of thyroid function improves CNS symptoms and internal carotid artery stenosis [4,8,9]. On the other hand, there are also reports that the symptoms and artery stenosis, even if thyroid function becomes normalized and antiplatelet drugs or surgical revascularization is required [4,10-12]. In our case, there has been no recurrence of symptoms since thyroid function was normalized, and there was no need for antiplatelet drugs or revascularization of the internal carotid artery.
Conclusions
Hyperthyroidism is one of etiologies of moyamoya syndrome; consequently, it is a potential differential diagnosis for Grave's disease, presenting with CNS symptoms. When a stroke occurs in a patient with Graves' disease, the coexistence of moyamoya syndrome should be suspected. Occasionally, this syndrome can be controlled with antithyroid medication alone.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Imaging of moyamoya disease and moyamoya syndrome: current status J Comput Assist Tomogr Li J Jin M Sun X 2572634320193058972110.1097/RCT.0000000000000834 PMC 6426357 · doi ↗ · pubmed ↗
- 2Moyamoya disease and moyamoya syndrome N Engl J Med Scott RM Smith ER 1226123736020091929757510.1056/NEJ Mra 0804622 · doi ↗ · pubmed ↗
- 3Clinical features of moyamoya disease with Graves' disease: a retrospective study of 394,422 patients with thyroid disease Endocr J Hiruma M Watanabe N Mitsumatsu T 1411487020233619861610.1507/endocrj.EJ 22-0319 · doi ↗ · pubmed ↗
- 4Moyamoya syndrome associated with Graves' disease: a case report and review of the literature J Stroke Cerebrovasc Dis Malik S Russman AN Katramados AM Silver B Mitsias PD 5285362020112113066810.1016/j.jstrokecerebrovasdis.2010.03.006 · doi ↗ · pubmed ↗
- 5Increased stiffness in common carotid artery in hyperthyroid Graves' disease patients Biomed Pharmacother Inaba M Henmi Y Kumeda Y 2412465620021219962310.1016/s 0753-3322(02)00195-6 · doi ↗ · pubmed ↗
- 6Concurrence of Graves' disease and dysplastic cerebral blood vessels of the moyamoya variety Thyroid Tendler BE Shoukri K Malchoff C Mac Gillivray D Duckrow R Talmadge T Ramsby GR 62562971997929295310.1089/thy.1997.7.625 · doi ↗ · pubmed ↗
- 7Moyamoya-like disease with inflammation Eur Neurol Panegyres PK Morris JG O'Neill PJ Balleine R 260263331993846785110.1159/000116950 · doi ↗ · pubmed ↗
- 8Co-morbidity of moyamoya disease with Graves' disease. report of three cases and a review of the literature Intern Med Sasaki T Nogawa S Amano T 6496534520061675509810.2169/internalmedicine.45.1543 · doi ↗ · pubmed ↗