Unusual Cause of Right Upper Quadrant Pain: Hepatic Amoebic Abscess
Elif Gündoğdu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
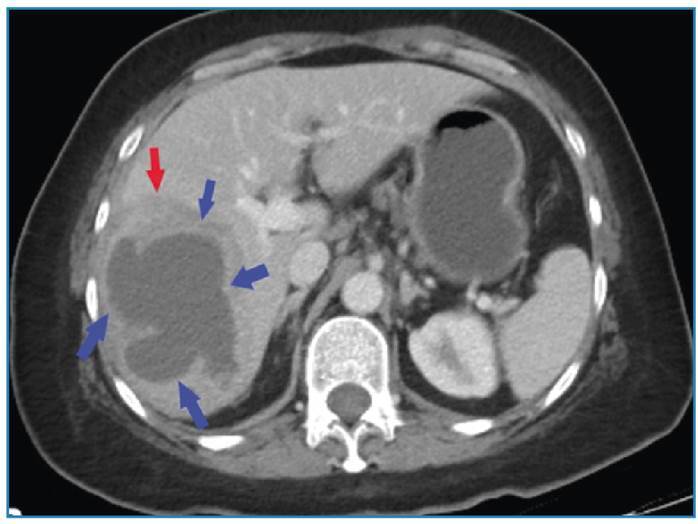 Figure 1
Figure 1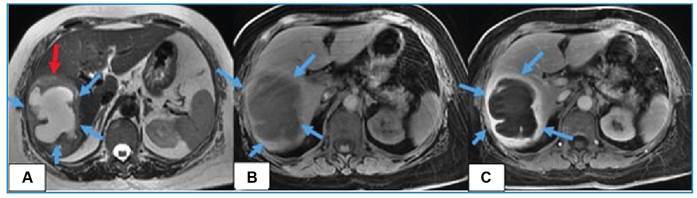 Figure 2
Figure 2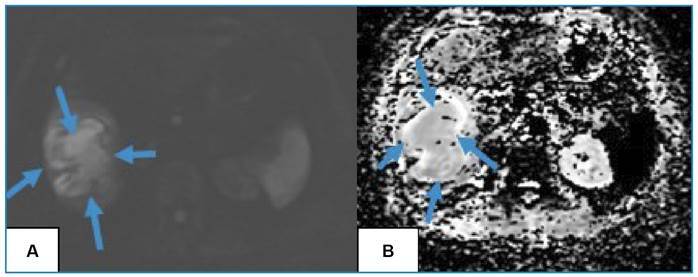 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Appendicitis Diagnosis and Management · Gallbladder and Bile Duct Disorders
A 66-year-old female, with no significant history, presented with a two-week history of right upper quadrant pain and chills. Her temperature was 36.8°C, and other vital signs were within normal limits. Physical examination revealed tenderness to palpation in the right upper quadrant.
Laboratory tests showed leukocytosis (12.6×10^3^ uL), elevated C-reactive protein (45 mg/L), erythrocyte sedimentation rate (38 mm/h), procalcitonin (0.06 ng/mL). Liver enzymes were slightly elevated (AST: 35 U/L, ALT: 48 U/L, and ALP: 162 U/L).
A computed tomography scan revealed a thick-walled cystic lesion with surrounding edema in the right lobe of the liver (Figure 1). Magnetic resonance imaging was performed to confirm the diagnosis. It showed the abscess with its characteristic thick enhancing wall and diffusion-restricting content (Figure 2, 3).
FIGURE 1:Computed tomography showing a thick-walled hypodense cystic lesion (blue arrows) with surrounding edema (red arrow).
FIGURE 2:Magnetic resonance imaging scan showing a A) hyperintense lesion on T2-weighted imaging (blue arrows) with perilesional edema (red arrow), a B) hypointense lesion on T1-weighted imaging (blue arrows), with an C) enhancing peripheral rim-like thick capsule (blue arrows).
FIGURE 3: A) Diffusion-weighted images and B) apparent diffusion coefficient map shows restricted diffusion within the lesion (blue arrows).
Based on the clinical presentation, imaging findings, and elevated inflammatory markers, a diagnosis of hepatic amoebic abscess was made. She was treated with metronidazole (500 mg) thrice daily for 10 days. Her symptoms significantly improved after initiation of treatment. Repeat imaging six months later showed a complete resolution of the abscess. While Entamoeba histolytica is a well-known pathogen1, causing potentially life-threatening hepatic amoebic abscess, its presentation can be atypical, as seen in this case. The extraintestinal disease is uncommon, and the liver (3-9%) is the most commonly affected organ1 ^,^ 2. Amoebic liver abscesses are more likely to be solitary than multiple lesions, and are more commonly found in the right lobe than in the left3. Drainage is not recommended because of the risk of rupture; medical treatment is preferred.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stanley SL Jr Amoebiasis Lancet 20033619362102510341266007110.1016/S 0140-6736(03)12830-9 · doi ↗ · pubmed ↗
- 2Usuda D Tsuge S Sakurai R Kawai K Matsubara S Tanaka R Amebic liver abscess by Entamoeba histolytica World J Clin Cases 2022103613157131663668364710.12998/wjcc.v 10.i 36.13157 PMC 9851013 · doi ↗ · pubmed ↗
- 3Chang CY Radhakrishnan AP Amoebic liver abscess Rev Soc Bras Med Trop 202255 e 06653523992010.1590/0037-8682-0665-2021 PMC 8909445 · doi ↗ · pubmed ↗