Maternal Obesity Modulates Cord Blood Concentrations of Proprotein Convertase Subtilisin/Kexin-type 9 Levels
Dimitrios Rallis, Aimilia Eirini Papathanasiou, Helen Christou

TL;DR
Babies born to overweight or obese mothers have higher levels of a protein called PCSK9 in their blood, which may be linked to inflammation and metabolic issues.
Contribution
This study is the first to show a link between maternal obesity and elevated PCSK9 levels in neonates.
Findings
Neonates born to overweight/obese mothers had significantly higher cord blood PCSK9 concentrations.
Higher cord blood PCSK9 was significantly associated with maternal overweight/obesity status after adjusting for perinatal factors.
Abstract
In utero exposure to maternal obesity or diabetes is considered a pro-inflammatory state. To evaluate whether cord blood proprotein convertase subtilisin/kexin-type 9 (PCSK9), which is regulated by inflammation and metabolic derangements, is elevated in neonates born to overweight, obese, or diabetic mothers. A retrospective study in full-term neonates born between 2010 and 2023, at Brigham and Women's Hospital. There were 116 neonates included in our study, of which 74 (64%) were born to overweight/obese mothers and 42 (36%) were born to nonoverweight/nonobese mothers. Neonates born to overweight/obese mothers had significantly higher cord blood concentrations of PCSK9 compared with neonates born to nonoverweight/nonobese group (323 [253-442] ng/mL compared with 270 [244-382] ng/mL, P = .041). We found no significant difference in cord blood concentrations of PCSK9 between neonates…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
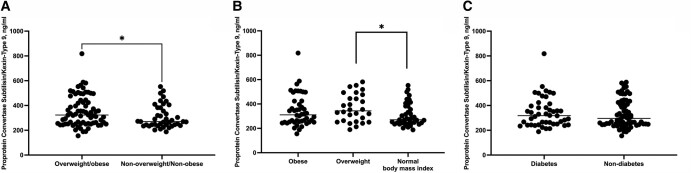 Figure 1
Figure 1| Overweight/obese (n = 74) | Normal BMI (n = 42) |
| |
|---|---|---|---|
| PCSK9, ng/mL | 323 (253-442) | 270 (244-382) | .041 |
| Gestational age, weeks | 38.5 ± 0.8 | 38.2 ± 0.8 | .083 |
| Birthweight, g | 3551 ± 585 | 3225 ± 514 | .003 |
| Birth length, cm | 49.8 ± 2.5 | 49.4 ± 2.6 | .440 |
| Head circumference, cm | 35.3 ± 2.6 | 34.4 ± 1.6 | .166 |
| Sex, male | 39 (53%) | 23 (55%) | .849 |
| Intrauterine growth restriction | 6 (8%) | 5 (12%) | .524 |
| Maternal diabetes | 32 (43%) | 14 (33%) | .328 |
| Maternal BMI | 34.1 ± 4.8 | 24.1 ± 3.1 | <.001 |
|
| <.001 | ||
|
Normal (18.5-24.9) Overweight (25-29.9) Obese (≥30) | - | 42 (100%) | |
| Delayed cord clamping | 54 (73%) | 33 (79%) | .656 |
| First parity | 24 (33%) | 13 (31%) | .289 |
| Maternal age, years | 34.1 ± 4.8 | 34.7 ± 4.6 | .520 |
|
| .286 | ||
| White/Caucasian | 41 (55%) | 29 (69%) | |
|
Black/African American Hispanic Asian Other | 14 (19%) | 3 (7%) | |
| Conception, in vitro fertilization | 4 (5%) | 6 (14%) | .165 |
| Delivery mode, cesarean section | 73 (99%) | 41 (98%) | 1.000 |
| Twin pregnancy | 1 (1%) | 2 (5%) | .297 |
| Gestational hypertension | 15 (20%) | 4 (10%) | .192 |
| Prolonged rupture of membranes | 3 (4%) | 1 (2%) | 1.000 |
| Chorioamnionitis | 1 (1%) | 2 (4%) | .297 |
| Apgar first minute | 8 (8-8) | 8 (8-8) | .141 |
| Apgar fifth minute | 9 (9-9) | 9 (9-9) | .319 |
| Resuscitation | 8 (11%) | 3 (7%) | .744 |
| Survival | 74 (100%) | 42 (100%) | 1.000 |
| Diabetes (n = 46) | Nondiabetes (n = 70) |
| |
|---|---|---|---|
| PCSK9, ng/mL | 318 (250-395) | 296 (250-418) | .729 |
| Gestational age, weeks | 38.2 ± 0.9 | 38.5 ± 0.8 | .154 |
| Birthweight, g | 3567 ± 687 | 3345 ± 482 | .043 |
| Birth length, cm | 49.8 ± 2.8 | 49.6 ± 2.3 | .658 |
| Head circumference, cm | 35.7 ± 3.3 | 34.6 ± 1.5 | .066 |
| Sex, male | 26 (57%) | 36 (51%) | .704 |
| Intrauterine growth restriction | 5 (11%) | 6 (9%) | .751 |
| Maternal BMI | 31.7 ± 7.2 | 30.1 ± 6.9 | .253 |
|
| .188 | ||
|
Normal (18.5-24.9) Overweight (25-29.9) Obese (≥30) | 14 (30%) | 28 (40%) | |
| Delayed cord clamping | 35 (76%) | 52 (74%) | 1.000 |
| First parity | 19 (41%) | 18 (26%) | .120 |
| Maternal age | 35.0 ± 4.6 | 34.0 ± 4.8 | .276 |
|
| .556 | ||
| White/Caucasian | 29 (63%) | 41 (59%) | |
|
Black/African American Hispanic Asian Other | 5 (11%) | 12 (17%) | |
| Conception, in vitro fertilization | 4 (9%) | 6 (9%) | 1.000 |
| Delivery mode, cesarean section | 44 (96%) | 70 (100%) | .155 |
| Twin pregnancy | 3 (7%) | — | .060 |
| Gestational hypertension | 6 (13%) | 13 (19%) | .458 |
| Prolonged rupture of membranes | 1 (2%) | 3 (4%) | 1.000 |
| Chorioamnionitis | 1 (2%) | 2 (3%) | 1.000 |
| Apgar first minute | 8 (8-8) | 8 (8-8) | .570 |
| Apgar fifth minute | 9 (9-9) | 9 (9-9) | .239 |
| Resuscitation | 7 (15%) | 4 (6%) | .110 |
| Survival | 46 (100%) | 70 (100%) | 1.000 |
| rho |
| |
|---|---|---|
| Overweight/obesity | 0.142 | .231 |
| Non-overweight/non-obesity | 0.495 | .002 |
| Diabetes | 0.043 | .783 |
| Non-diabetes | 0.180 | .146 |
| b | 95% CI |
| |
|---|---|---|---|
| PCSK9 | |||
| Overweight/obesity | 50.12 | 4.02-96.22 | .033 |
| Gestational age | −16.60 | (−96.22)-10.02 | .219 |
| Birth weight | −0.01 | (−0.05)-0.04 | .963 |
| Sex, male | −8.83 | (−52.86)-35.19 | .692 |
| Intrauterine growth restriction | 13.45 | (−70.32)-97.24 | .751 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLipid metabolism and disorders · Folate and B Vitamins Research · Metabolism, Diabetes, and Cancer
In utero exposure to maternal obesity or diabetes is associated with a pro-inflammatory state [1, 2] and increased risk of cardiometabolic diseases in the offspring [3], including obesity, elevated blood pressure, impaired insulin/glucose homeostasis, and abnormal lipid profiles [4-6]. Maternal metabolic changes during pregnancy lead to perturbations in fetal insulin sensitivity, lipid metabolism, and placental energy metabolism [3]. The placenta produces an array of signaling molecules that control crosstalk between the mother and the fetus and regulate the fetal metabolism including lipoprotein homeostasis [7]; however, the mechanisms regulating fetal lipoprotein homeostasis in high-risk pregnancies have not been fully evaluated.
Proprotein convertase subtilisin/kexin type 9 (PCSK9) is primarily derived from hepatocytes; it is also expressed in other tissues such as small intestine, kidney, pancreas, and immune system [8] and binds low-density lipoprotein (LDL) receptors thereby leading to higher serum LDL cholesterol concentrations [9, 10]. The large molecular weight of PCSK9 likely precludes its transplacental transfer, but PCSK9 is detectable in cord blood and may regulate fetal lipid levels [10, 11]. Previous studies showed that PCSK9 concentrations in cord blood or the serum of high-risk neonates (ie, neonates born premature, with intrauterine growth restriction, or small or large for gestational age [GA]) differ significantly compared with neonates born at term, without growth restriction, or with appropriate birth weight for GA [12-14]. However, the impact of maternal overweight/obesity and/or diabetes on the concentrations of PCSK9 in the neonatal-placental circulation is unknown. In the current study, we examined the cord blood concentrations of PCSK9 in neonates born to overweight/obese compared with neonates born to nonoverweight/nonobese and diabetic compared with nondiabetic mothers.
Materials and Methods
We conducted a retrospective case-control study at Brigham and Women's Hospital, Boston, MA, USA. The study was approved by the Mass General Brigham Human Research Committee, which is the institutional review board of Mass General Brigham, on behalf of the Brigham and Women's Hospital (Protocol Number 2012P000384/02.10.2012). The Human Research Committee waived the requirement to obtain a consent. From our biorepository of cord blood samples from 2013 to 2023, we included 116 available samples from neonates born at ≥37 weeks of GA. Prepregnancy maternal body mass index (BMI) was calculated based on the maternal weight and height that were measured at the time of the initial pregnancy assessment, according to the formula BMI = weight/height^2^. Maternal BMI of 18.5 to 24.9 was classified as normal, BMI of 25 to 29.9 as overweight, and BMI ≥30 as obesity per accepted standards [15]. Maternal diabetes was diagnosed according to the guidelines of the American Diabetes Association, including preexisting diabetes and gestational diabetes mellitus [16]. We compared cord blood PCSK9 concentrations in neonates born to overweight/obese vs nonoverweight/nonobese mothers and to diabetic vs nondiabetic mothers.
We collected the perinatal data for neonates including GA, birth weight, length, and head circumference, sex, intrauterine growth restriction, delayed cord clamping, parity, maternal age, and race, mode of conception and delivery, multiple pregnancy, gestational hypertension, prolonged rupture of membranes, chorioamnionitis, Apgar score in the first and fifth minutes, resuscitation at birth, and survival.
Measurement of Cord Blood PCSK9 Concentration
Mixed arteriovenous blood samples were collected at the time of delivery from the doubly clamped umbilical cord, in EDTA tubes, and were immediately centrifuged. The supernatant plasma was kept frozen at −80 °C until assay.
Plasma PCSK9 levels were determined in a single batch in duplicate using a sandwich enzyme-linked immunosorbent assay kit (Bio Vendor Laboratory Medicine, catalog number RD191473200R, RRID AB_3083527; limit of detection: 9 pg/mL). The intra- and interassay coefficients of variation were 5.2% to 5.3% and 4.0% to 7.5%, respectively.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median (interquartile range), as appropriate. The normality of the distributions of continuous variables was assessed by the Kolmogorov-Smirnov test. Comparisons of continuous variables between 2 groups were performed using the Student unpaired t-test or the nonparametric Mann-Whitney test. Comparison of cord blood PCSK9 levels between more than2 groups was performed using the nonparametric Kruskal-Wallis test. Categorical variables were expressed as n (percentage %) and compared with the χ^2^ test or Fisher exact test. The correlation between prepregnancy maternal BMI with the cord blood PCSK9 concentration in neonates born to overweight/obese, nonoverweight/nonobese, diabetic, and nondiabetic mothers was examined with Spearman rho. A multivariate linear regression model with generalized estimating equations to account for multiples in our patient cohort was used to examine the association of PCSK9 levels (dependent variable) with maternal overweight/obesity, adjusted for GA, birth weight, sex, and intrauterine growth restriction (independent variables). Coefficients and 95% CIs were calculated.
All tests were 2-sided and a P < .05 was considered statistically significant (alpha .05). A power analysis revealed that a sample size of 116 neonates is sufficient to detect a difference of 15% in cord plasma PCSK9 concentration between groups, with a power of 0.8 and a type I error of 0.05. The data were analyzed using SPSS Statistics (IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY, USA).
Results
Among the 116 neonates included in our study, 74 (64%) were born to overweight/obese mothers and 42 (36%) were born to nonoverweight/nonobese mothers. There were no differences in perinatal characteristics between the 2 groups, except for a significantly higher birthweight in favor of the overweight/obese group (Table 1). The mean GA in the overweight/obese group was 38.5 ± 0.8 weeks and the mean birth weight was 3551 ± 585 g, compared with a mean GA of 38.2 ± 0.8 (P = .083) and birth weight of 3225 ± 514 g (P = .003) in the nonoverweight/nonobese group (Table 1). Neonates in the overweight/obese group had significantly higher cord blood concentrations of PCSK9 compared with neonates in the nonoverweight/nonobese group (323 [253-442] ng/mL compared with 270 [244-382] ng/mL, P = .041) (Fig. 1A). When analyzed by maternal prepregnancy BMI, a significant difference was found between cord blood PCSK9 concentrations in neonates of overweight mothers vs neonates born to mothers with normal prepregnancy BMI (343 [259-460] ng/mL vs 270 [244-382] ng/mL, P = .023) (Fig. 1B).
(A) Proprotein convertase subtilisin/kexin type 9 (PCSK9) in neonates born to overweight/obese mothers compared with neonates born to mothers with normal body mass index. (B) PCSK9 in neonates born to mothers with normal body mass index, overweight, and obesity. (C) PCSK9 in neonates born to diabetic mothers compared with neonates born to nondiabetic mothers.
Of the 116 neonates, 46 (40%) were born to diabetic mothers and 70 (60%) were born to nondiabetic mothers. There were no differences in perinatal characteristics between neonates born to diabetic mothers and neonates born to nondiabetic mothers except for a significantly higher birth weight among infants of diabetic mothers (3567 ± 687 g vs 3345 ± 482 g; P = .043) (Table 2). We found no significant difference in cord blood concentrations of PCSK9 between neonates of diabetic mothers compared with neonates of nondiabetic mothers (318 [250-395] ng/mL compared with 296 [250-418] ng/mL, P = .729) (Fig. 1C). Also, among the 74 neonates of overweight/obese mothers, we found no significant difference in cord blood concentrations of PCSK9 between the 32 (43%) neonates of diabetic mothers compared with the 42 (57%) neonates of nondiabetic mothers (314 [247-379] ng/mL compared with 340 [255-493] ng/mL, P = .230).
Prepregnancy maternal BMI was significantly associated with cord blood PCSK9 only in neonates born to nonoverweight/nonobese mothers (r = 0.495, P = .002). This association was not significant in any other neonatal-maternal group (Table 3).
In multivariate linear regression analysis, higher cord plasma PCSK9 concentration was significantly associated with maternal overweight/obesity status (b = 50.12; 95% CI, 4.02-96.22; P = .033) after adjusting for GA (b = −16.60; 95% CI, −96.22 to −10.02; P = .219), birth weight (b = −0.01; 95% CI, −0.05 to −0.04; P = .963), male sex (b = −8.83; 95% CI, −52.86 to −35.19; P = .692), and intrauterine growth restriction (b = 13.45; 95% CI, −70.32 to −97.24; P = .751) (Table 4).
Discussion
Our study demonstrates that cord blood PCSK9 concentrations are significantly higher in neonates born to overweight/obese mothers compared with neonates born to nonoverweight/nonobese mothers. Prepregnancy maternal BMI is significantly associated with cord blood PCSK9 in neonates born to nonoverweight/nonobese mothers, whereas higher cord blood PCSK9 concentrations are significantly associated with maternal overweight/obesity status, after adjusting for GA, birth weight, sex, and intrauterine growth restriction.
PCSK9 regulates circulating LDL cholesterol levels by promoting the degradation of LDL receptors [9]. It is mainly produced in the liver but also expressed in various cells throughout the body, including small intestinal enterocytes, vascular endothelial and smooth muscle cells [17], cardiomyocytes [18], macrophages [19], and various cells in the placenta [20]. In fetal life, PCSK9 expression has been first detected in the liver at embryonic day 9 and in the skin, kidney, small intestine, and cerebellum at embryonic day 15 [21]. In tissue culture and animal studies, PCSK9 expression is increased in response to hypoxia, cardiomyocyte injury [22], systemic inflammation [23], hemodynamic shear stress, and oxidative stress [24-26]. In human studies in adults, serum PCSK9 levels are positively associated with acute myocardial infarction [27] and high-sensitivity C-reactive protein levels [28], whereas PCSK9 inhibitors such as evolocumab or alirocumab reduce the risk of recurrent ischemic cardiovascular events [29, 30]. In pregnant women, serum PCSK9 concentrations at delivery are significantly higher compared with nonpregnant women, and PCSK9 concentrations in cord blood are significantly lower than the corresponding maternal concentrations, indicating the unlikely contribution of maternal PCSK9 to cord blood concentrations [10]. Moreover, PCSK9 was previously associated with urgent cesarean delivery [31]. Previous studies in neonates showed that PCSK9 concentrations were significantly higher in neonates born small or large for GA compared with neonates born appropriate for GA. Also, PCSK9 concentrations in neonates showed a significant correlation with total and LDL cholesterol [12]. Another study in newborns showed that neonatal PCSK9 concentrations were a significant predictor of fetal LDL-cholesterol levels independent of small-for-GA status in multivariate analysis [13]. Our findings, demonstrating that cord blood PCSK9 concentrations were significantly higher in neonates born to overweight/obese mothers compared with neonates born to mothers with normal prepregnancy BMI, lend support to the notion that the proinflammatory state of being overweight, or obese, leads to elevated PCSK9 [32].
Maternal overweight status, obesity, and diabetes during pregnancy are considered proinflammatory states [1, 2]. Obesity is known to cause chronic endothelial activation and dysfunction [33, 34], excessive production of reactive oxygen species [35, 36], hyperinsulinemia and insulin resistance [37], and dyslipidemia [1]. In addition, exposure to an obesogenic maternal environment has been associated with abnormalities in placental metabolic regulation, leading to epigenetic modifications [38-40]. Placentas from diabetic or obese pregnancies show decreased expression of genes implicated in cholesterol utilization and LDL receptors, independent of the level of maternal cholesterol but likely resulting from high fetal insulin levels [19, 40]. Epigenetic remodeling during early life could constitute a molecular mechanism through which intrauterine stimuli can have an impact on gene regulation and DNA damage and repair [41-44]. A recent study showed hypomethylation of the PCSK9 gene in placentas of diabetic pregnancies compared with controls [45], and DNA methylation alterations in blood cells of offspring born to obese mothers have also been previously demonstrated [6].
Higher circulating PCSK9 levels were found in obese compared with nonobese adult subjects [46, 47], and female obese subjects with type 2 diabetes had the highest levels of PCSK9 within a group of young adults aged 15 to 26 years [9]. Taken together, these previous studies support that female sex and proinflammatory states such as overweight/obesity status, as well as intrauterine growth restriction and prematurity are associated with higher circulating PSCK9 concentrations, suggesting a possible impact of estrogens, epigenetics, and gestational maturation on metabolic states [12-14]. In our study, cord blood PCSK9 concentration was significantly associated with maternal overweight/obesity status, after adjusting for GA, birth weight, sex, and intrauterine growth restriction. We conclude that PCSK9 may be a useful biomarker of lipoprotein metabolism in fetal life because PCSK9 levels in the neonatal-placental circulation are susceptible to several conditions that affect lipoprotein regulation including maternal overweight status/obesity.
Our study has several limitations. Given the known association between obesity and insulin resistance, it is possible that we included women with undiagnosed insulin resistance within our nondiabetic mother group, two thirds of which were overweight or obese. In addition, we do not have data on maternal lipid profiles, circulating PCSK9 concentrations, or markers of glucose metabolism. Although in previous studies, PCSK9 levels have been correlated with markers of blood glucose homeostasis in patients with type 2 diabetes [48], in our retrospective study, we used stored samples that were of limited quantity and were not appropriately processed for lipid analysis, inflammation markers, or markers of glucose metabolism. Future longitudinal studies would be important in further delineating the relationship between maternal obesity or diabetes and infant PCSK9 levels.
Conclusions
Higher cord blood PCSK9 concentrations are significantly associated with maternal overweight/obesity status, after adjustment for GA, birth weight, sex, and intrauterine growth restriction; this finding may warrant larger, prospective, longitudinal studies to examine the utility of PCSK9 as a biomarker of lipoprotein metabolic profile in high-risk neonates and its potential predictive role in later metabolic syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ramsay JE, Ferrell WR, Crawford L, Wallace AM, Greer IA, Sattar N. Maternal obesity is associated with dysregulation of metabolic, vascular, and inflammatory pathways. J Clin Endocrinol Metab. 2002;87(9):4231‐4237.12213876 10.1210/jc.2002-020311 · doi ↗ · pubmed ↗
- 2Challier JC, Basu S, Bintein T, et al Obesity in pregnancy stimulates macrophage accumulation and inflammation in the placenta. Placenta. 2008;29(3):274‐281.18262644 10.1016/j.placenta.2007.12.010PMC 4284075 · doi ↗ · pubmed ↗
- 3Helle E, Priest JR. Maternal obesity and diabetes Mellitus as risk factors for congenital heart disease in the offspring. J Am Heart Assoc. 2020;9(8):e 011541.32308111 10.1161/JAHA.119.011541 PMC 7428516 · doi ↗ · pubmed ↗
- 4Gaillard R, Steegers EA, Duijts L, et al Childhood cardiometabolic outcomes of maternal obesity during pregnancy: the generation R study. Hypertension. 2014;63(4):683‐691.24379180 10.1161/HYPERTENSIONAHA.113.02671 · doi ↗ · pubmed ↗
- 5Perng W, Gillman MW, Mantzoros CS, Oken E. A prospective study of maternal prenatal weight and offspring cardiometabolic health in midchildhood. Ann Epidemiol. 2014;24(11):793‐800.e 1.25263237 10.1016/j.annepidem.2014.08.002PMC 4254266 · doi ↗ · pubmed ↗
- 6Alba-Linares JJ, Perez RF, Tejedor JR, et al Maternal obesity and gestational diabetes reprogram the methylome of offspring beyond birth by inducing epigenetic signatures in metabolic and developmental pathways. Cardiovasc Diabetol. 2023;22(1):44.36870961 10.1186/s 12933-023-01774-y PMC 9985842 · doi ↗ · pubmed ↗
- 7Carter AM . Evolution of placental function in mammals: the molecular basis of gas and nutrient transfer, hormone secretion, and immune responses. Physiol Rev. 2012;92(4):1543‐1576.23073626 10.1152/physrev.00040.2011 · doi ↗ · pubmed ↗
- 8Seidah NG, Garçon D. Expanding biology of PCSK 9: roles in atherosclerosis and beyond. Curr Atheroscler Rep. 2022;24(10):821‐830.35904732 10.1007/s 11883-022-01057-z PMC 9335453 · doi ↗ · pubmed ↗