Revitalizing Recovery: Unveiling the Transformative Impact of Physiotherapy in Rehabilitating a Neglected Case of Shoulder Hemiarthroplasty
Om C Wadhokar, Minal Dahiwadkar, Sakshi Rawal, Reetkaur Arora, Aakanksha Choudhari, Aishwarya Mali, Chaitanya A Kulkarni, Tushar J Palekar, Mayur Wanjari

TL;DR
This case study shows how physiotherapy helped improve recovery after shoulder surgery when rehabilitation was initially lacking.
Contribution
The paper highlights the transformative impact of a targeted physiotherapy protocol in rehabilitating a neglected shoulder hemiarthroplasty case.
Findings
The patient regained significant shoulder range of motion and muscle strength through physiotherapy.
Functional independence and quality of life improved after implementing a combined physiotherapy and pharmacological treatment plan.
Electrical muscle stimulation and targeted strengthening exercises were key components of successful rehabilitation.
Abstract
The shoulder joint has a complex anatomy and biomechanics. It is a ball and socket joint made by the articulation surface of the humeral head (ball) and glenoidal fossa (socket) of the scapula. Shoulder arthroplasty is done when parts of the shoulder joint are severely affected and damaged beyond repair. The damaged parts are replaced with artificial parts. Prosthetic implants are typically made of metal or plastic material. Implants come in various sizes and shapes. There are three types of surgical arthroplasty: total shoulder arthroplasty, partial shoulder arthroplasty, and reverse arthroplasty. Indications of shoulder arthroplasty may include osteoarthritis, fractures, rotator cuff injuries, osteonecrosis, and rheumatoid arthritis. This case study aims to provide a case of anteroinferior dislocation of the left shoulder with humeral head comminuted fracture confirmed by an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
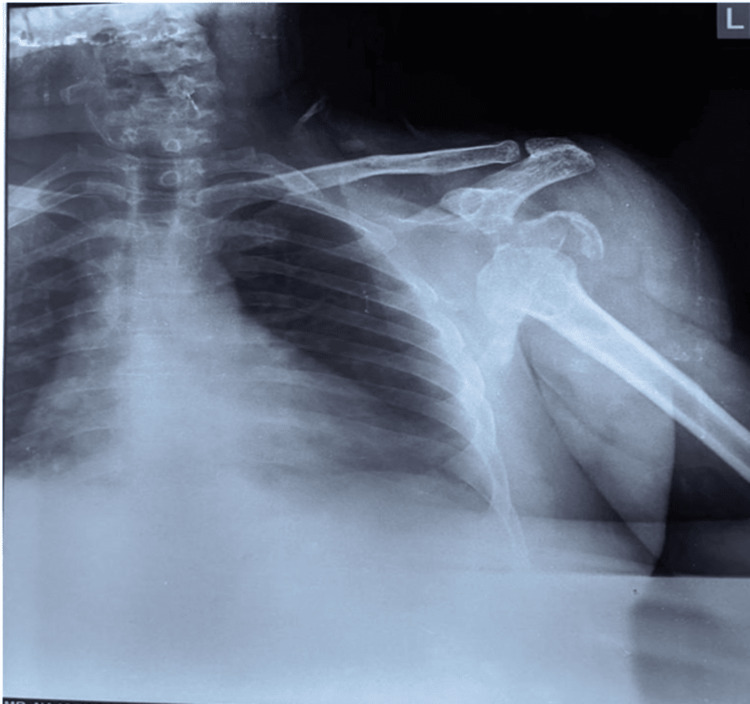 Figure 1
Figure 1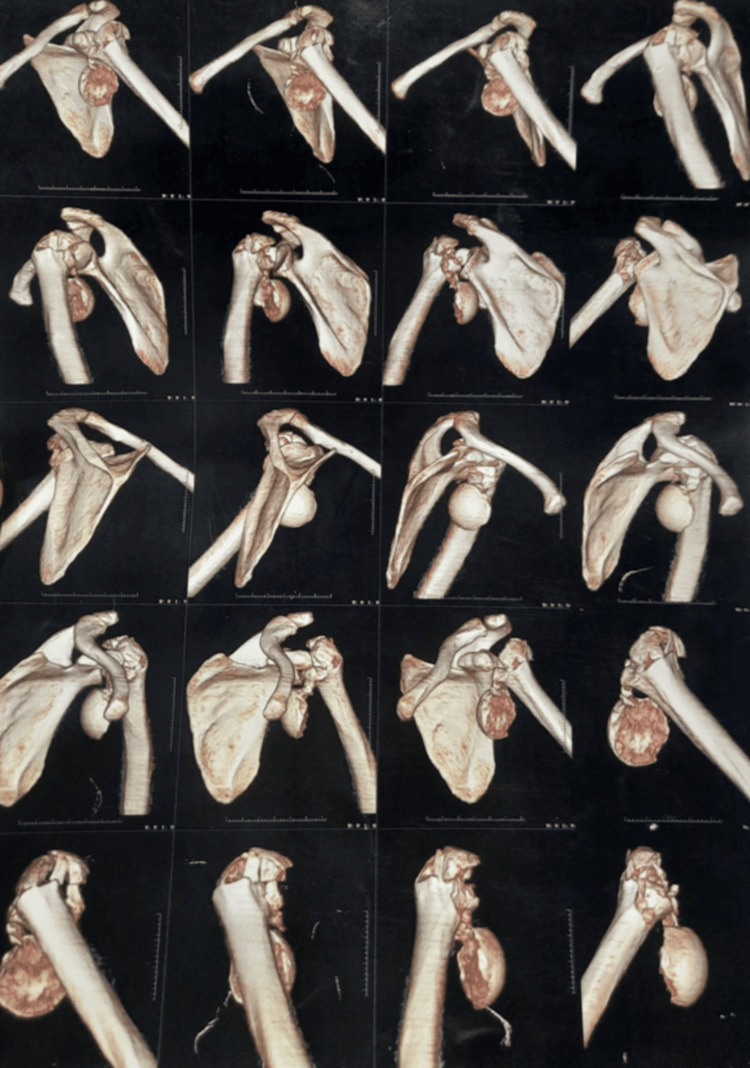 Figure 2
Figure 2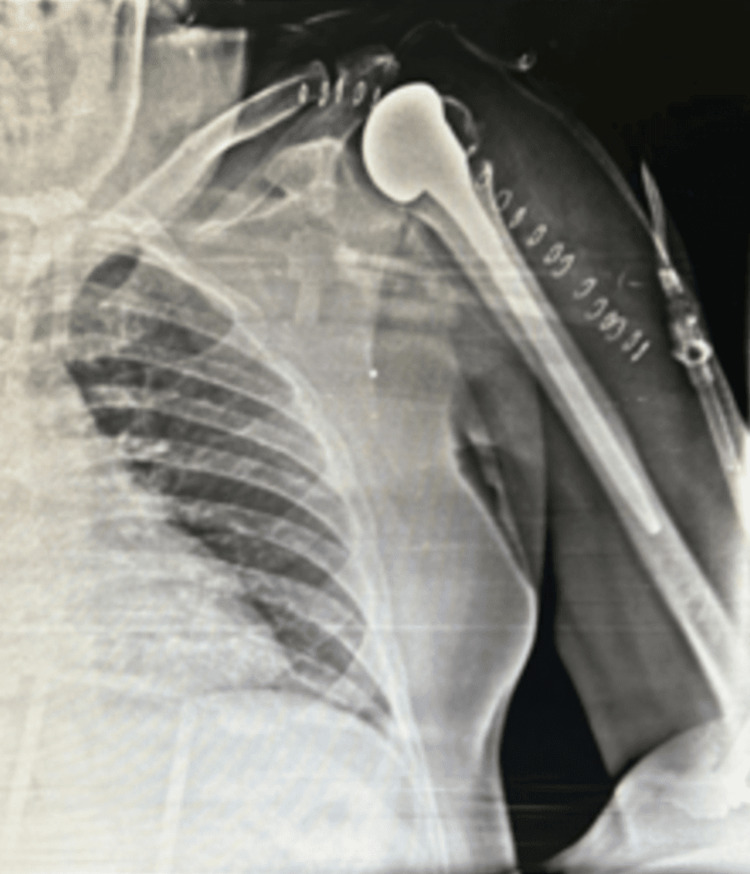 Figure 3
Figure 3| Joint | Movement | Active Left | Passive Left |
| Shoulder | Flexion | 0-10° | 0-120° |
| Extension | 0-10° | 0-35° | |
| Abduction | 0-5° | 0-90° | |
| Adduction | 5-0° | 90-0° | |
| Elbow | Flexion | 0-140° | 0-140° |
| Extension | 140-0° | 140-0° |
| Joint | Muscles | Grade |
| Shoulder | Flexors | 1/5 |
| Extensors | 1/5 | |
| Abductors | 1/5 | |
| Elbow | Flexors | 4/5 |
| Extensors | 4/5 | |
| Wrist | Flexors | 4/5 |
| Extensors | 4/5 |
| Short-Term Goals | Interventions | Dosage | Rationale |
| 1) Patient education | Educate the patient about the importance of exercise for improving the quality of life. | At the beginning of treatment on Day 1 | To make patient actively involved in the rehabilitation |
| 2) Pain reduction | Hot pack | Before proceeding the exercises 10 min over the anterior aspect of the shoulder | Reduce pain and promote healing and make soft tissue more pliable. |
| 3) Muscle activation | A) Electrical muscle stimulation over middle fibres of deltoid. B) Serratus anterior muscle activation. C) Rotator cuff muscle activation | A) Surged faradic current 30 contractions × 3 repetitions. B) & C) 10 repetitions 4 times in a day | To improve the contractility of the muscle and improve the strength of the musculature |
| 4) Increase muscle strength | A) Eccentric muscle strengthening for shoulder flexors and abductors. B) exercise with resistance band. | 10 repetitions 4 times in a day | To improve and maintain muscle strength |
| 5) Improve range of motion | A) Shoulder ROM exercises in gravity eliminating plane in available range and further progressing to against gravity. B) wand exercises. C) Shoulder wheel. D) Finger ladder | 15 repetitions 4 times in a day | To implement the required range of activities |
| 6) Improve flexibility | Gentle stretching manoeuver to anterior muscle pectoralis major | 3 sets of 30 seconds hold twice a day | Enhance flexibility thereby improving range |
| 7) Maintain posture | A) Shoulder shrugs, B) scapular sets | 15 repetitions 4 times in a day | To avoid depression of shoulder on one side |
| Long-Term Goals | |||
| 1) Improve neuromuscular control and muscle endurance | Stabilization exercises | Twice a day | To improve muscle endurance and control |
| Joint | Movement | Pre-treatment Active Left | Post-treatment Active Left |
| Shoulder | Flexion | 0-10° | 0-40° |
| Extension | 0-10° | 0-35° | |
| Abduction | 0-5° | 0-25° | |
| Adduction | 5-0° | 25-0° | |
| Elbow | Flexion | 0-140° | 0-140° |
| Extension | 140-0° | 140-0° |
| Joint | Muscles | Pre-treatment MMT | Post-treatment MMT |
| Shoulder | Flexors | 1/5 | 3+/5 |
| Extensors | 1/5 | 3+/5 | |
| Abductors | 1/5 | 3/5 | |
| Elbow | Flexors | 4/5 | 5/5 |
| Extensors | 4/5 | 5/5 | |
| Wrist | Flexors | 4/5 | 5/5 |
| Extensors | 4/5 | 5/5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Nerve Injury and Rehabilitation
Introduction
Shoulder hemiarthroplasty is a surgical procedure that replaces the shoulder joint with artificial materials like metal or plastic to restore function. Some types of shoulder arthroplasty are unconstrained total hemiarthroplasty, semi-constrained inversed shoulder prostheses, and humeral hemiarthroplasty [1]. These surgeries have exhibited <91% success, but about 14% of risks are noted. Some complications are glenoid or humeral head loosening, infection, instability, rotator cuff tear, and ectopic ossification. Revision surgeries are done in cases of complications [2]. Complications of shoulder hemiarthroplasty, according to a study, are pain from glenoid erosion, stiffness, avascular necrosis (AVN), and subscapularis tear. Total shoulder arthroplasty results in glenoid loosening, and shoulder hemiarthroplasty leads to glenoid erosion and stiffness in the long term [3]. After the surgery, range of motion, muscle activity, and proprioception are lost and have to be regained again. Physiotherapy plays a vital role in restoring these functions. For shoulder hemiarthroplasty, restoring the rotator cuff muscle strengthening and function is of utmost importance [4]. It also plays a vital role in shoulder arthroplasty patients, reinstating their shoulder range of motion, mobility, and activities of daily living [5].
Case presentation
A 58-year-old male with the dominance of the right side complained of severe pain and inability to perform left shoulder movements. These complaints commenced due to a road traffic accident on 13 April 2023. The patient had a fall over his left shoulder with a flexed elbow on a non-uniform road with stones from a two-wheeler. There was no history of loss of consciousness or any external bleeding. The patient was taken to a nearby hospital where a radiograph and CT scan of the left shoulder were obtained, which showed a displaced comminuted humeral head fracture with anteroinferior dislocation and fracture of the left shoulder (Figures 1, 2). Considering the severity of the comminuted fracture, left shoulder hemiarthroplasty was performed on 22 April 2023 (Figure 3). The patient was admitted for two weeks post-operation. He did not receive any physiotherapy treatment post-operation for one month due to a lack of awareness and knowledge about the same. He continued taking medications for pain relief. When the pain intensity increased, and he was unable to perform functional activities, the patient visited Dr. D. Y. Patil for physiotherapy OPD and physiotherapy rehabilitation treatment was started on 4 June 2023.
X-ray showing dislocation and fracture of the left shoulder joint.
CT scan showing fracture and dislocation of left shoulder joint.
Post-operative X-ray of the left shoulder joint
Clinical findings
The patient was assessed in a standing position with hands neutrally by the side of the body and head in a neutral position. On general examination, vitals were stable. In postural observation, left shoulder depression was observed. The scar was present over the anterior aspect of the left shoulder, which was 8cm long. When palpated, tenderness was absent over the shoulder region. On the numerical pain rating scale, the pain intensity was 9/10 while moving the shoulder joint in all planes and 2/10 while resting. The nature of the pain was intermittent, which aggravated while attempting to perform movements. On examination, the patient could not actively perform a specific shoulder range of motion. Initially, the patient could perform shoulder flexion, abduction, and internal rotation in a gravity-eliminating plane and the patient presented with a significant reduction in scapular mobility (Table 1). Pre-treatment strength assessment is mentioned in Table 2. On assessing the function based on the shoulder pain and disability index (SPADI), the score obtained was 86/130. The end feel of shoulder movements was empty due to pain. In sensory examination, superficial sensations, deep sensations, and cortical sensations were intact. No positive findings were captured in the gait except reduced arm swing on observation and balance assessment was normal.
Timeline
On 13 April 2023, the patient had a fall from a two-wheeler over the patient's left shoulder on a non-uniform road, from where he was taken to a nearby hospital where investigations were performed. The patient was operated on with left shoulder hemiarthroplasty on 22 April 2023. Post-operation, the patient was on pain medications, but no significant improvement was seen. So on 4 June 2023, he visited Dr. D. Y. Patil, physiotherapy outpatient department, and physiotherapy rehabilitation was started on the same day.
Diagnostic assessment
The day after the accident, an X-ray and CT scan were obtained in which a radiograph of the left shoulder revealed a displaced comminuted humeral head fracture with anterior dislocation of the left shoulder (Figure 1). CT scan revealed multiple small fragments in the adjacent soft tissue around the left shoulder. Also, glenohumeral joint effusion was noted which can be resolved by active physical therapy exercises helping them to drain in the lymph nodes nearby. The displacement of the humeral head was antero-inferiorly (Figure 2). The reports of Hb, WBC, RBC, and blood sugar levels were regular. As the fracture was highly impacted, the decision to operate it with shoulder hemiarthroplasty was taken into consideration. The post-operative radiograph showed a cemented unipolar implant, including a head resembling the humeral head placed in the glenoid cavity and steam reaching up to the upper 1/3rd of the shaft, indicating hemiarthroplasty (Figure 3). The patient was diagnosed as a postoperative case of left shoulder hemiarthroplasty.
Physiotherapy intervention
Physiotherapy intervention was built which consisted of short-term goals and long-term goals (Table 3). Short-term goals comprised the education of the patient regarding the condition and engaging the patient in all aspects of interventions. Prevention of muscle stiffness and post-operative complications and encompassing pain reduction techniques followed by re-education of muscle by electrical stimulation and increasing muscle strength was established. Eccentric strengthening helps in increasing strength when muscle fibres are lengthened. Implementation of a range of motion exercises in available range in gravity eliminating plane and further progressing to against gravity, along with wand exercises. The use of a shoulder wheel and finger ladder was also involved. Activation of muscle and stretching was incorporated. Long-term exercises were focused on maintaining short-term goals along with improving cardiopulmonary resilience and improving coordination through various exercises and helping the patient in returning back to normal recreational activities.
Follow-up and outcome are mentioned in Table 4 and Table 5.
Discussion
Shoulder hemiarthroplasty is a surgical procedure in which the shoulder joint is removed and substituted or replaced with artificial implants. The advantage is restoration of the functional mobility of the shoulder joint, in association with reducing pain and other complaints. Regaining the range of motion strength and following the restoration of functional activity of the shoulder joint are essential for patients to obtain a decent and good outcome post-surgery [6]. In the present case, the patient presented with left shoulder hemiarthroplasty with complaints of restricted range of motion and inability to perform functional activities of the left shoulder joint. Physiotherapy rehabilitation here can play an essential role in resolving patients' problem list as the root cause for impaired and restricted shoulder ranges. Physiotherapy can be effective in reducing pain, activating the muscles, and improving strength, thereby contributing to good functional status and good quality of life. In the given Table 1 are the ranges recorded at the beginning of the assessment where the surgery patient could still not perform initial ranges of shoulder flexion, abduction, extension, and internal-external rotation. Similarly, with altered ranges, the patient also lacked the strength in muscles to activate respective action at the joint level, which again is a contributing cause to loss of ranges. Table 3 states the strength of muscles on the first day of assessment. A tailored protocol with sufficient dosage and progression was introduced which showed a gradual progression in the range of motion and strength of the individual.
The given case study varies from other cases; there was an introduction of muscle stimulation using faradic current to see the effectiveness of pain reduction and muscle activation, which resulted in the improvement of ranges and muscle strength (Table 2 and Table 4). In addition to using electrical stimulation, there was the contribution of exercises that focused on muscle activation in the initial stages, which combined gave an improved functional response. The entire treatment protocol played a crucial role in reducing pain and boosting muscle strength, thereby increasing and enhancing ranges and functional self-dependence, and quality of life in patients with total shoulder hemiarthroplasty [7-10].
Conclusions
We conclude that the application of physical therapy rehabilitation in patients with shoulder hemiarthroplasty helps in improving the well-being of the patient. The case study differs in the occurrence of severe comminuted fracture of the head of the humerus along with dislocation which rarely occurs in road traffic accidents. Thus implementation of physical therapy plays a vital role in getting back a patient to normal daily activities by minimizing pain and enhancing functional range of motion and gaining required strength.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shoulder arthroplasty Eur Radiol Buck FM Jost B Hodler J 29372948182008 https://core.ac.uk/download/pdf/159152401.pdf 1861811710.1007/s 00330-008-1093-8 · doi ↗ · pubmed ↗
- 2Physiotherapy following elective orthopaedic procedures Haemophilia De Kleijn P Blamey G Zourikian N Dalzell R Lobet S 10811212 Suppl 32006 https://pubmed.ncbi.nlm.nih.gov/16684004/10.1111/j.1365-2516.2006.01266.x 16684004 · doi ↗ · pubmed ↗
- 3Reverse shoulder arthroplasty: the role of physical therapy on the clinical outcome in the mid-term to long-term follow-up Arch Orthop Trauma Surg Uschok S Herrmann S Pauly S Perka C Greiner S 134713521382018 https://pubmed.ncbi.nlm.nih.gov/29916056/2991605610.1007/s 00402-018-2977-y · doi ↗ · pubmed ↗
- 4Shoulder hemiarthroplasty: outcomes and long-term survival analysis according to etiology Orthop Traumatol Surg Res Gadea F Alami G Pape G Boileau P Favard L 6596659820122294439310.1016/j.otsr.2012.03.020 · doi ↗ · pubmed ↗
- 5Stemless shoulder arthroplasty Orthop Traumatol Surg Res Teissier J Teissier P 10346010920233694279310.1016/j.otsr.2022.103460 · doi ↗ · pubmed ↗
- 6Outcomes after bilateral shoulder arthroplasty: a systematic review J Shoulder Elbow Surg Polascik BA Chopra A Hurley ET 8618713220233656701510.1016/j.jse.2022.11.010 · doi ↗ · pubmed ↗
- 7Acute surgical management of proximal humerus fractures: ORIF vs. hemiarthroplasty vs. reverse shoulder arthroplasty J Shoulder Elbow Surg Yahuaca BI Simon P Christmas KN Patel S Gorman RA 2nd Mighell MA Frankle MA 04029202010.1016/j.jse.2019.10.01231948835 · doi ↗ · pubmed ↗
- 8Physical therapy management in a severe case of overlapping of bone post crush injury: a case report Cureus Kulkarni CA Wadhokar OC Joshi MV 0142022 https://pubmed.ncbi.nlm.nih.gov/36320958/10.7759/cureus.29708 PMC 961655836320958 · doi ↗ · pubmed ↗