Histological analysis of psoriasiform eruption associated with myelin oligodendrocyte glycoprotein antibody-associated disease
Saori Itoi-Ochi, Yukiho Kurosaki, Asako Ota, Akiko Miyazaki, Akiko Hosokawa, Misa Nakano, Toshiyuki Takahashi, Noriko Umegaki-Arao, Manabu Fujimoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
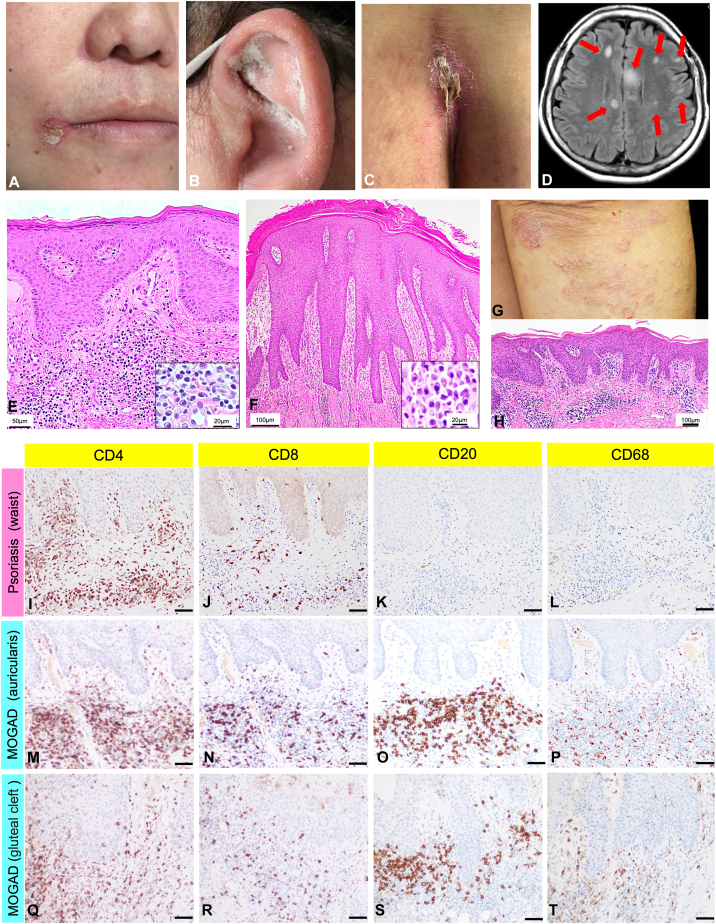 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsoriasis: Treatment and Pathogenesis · Cytokine Signaling Pathways and Interactions · Immunodeficiency and Autoimmune Disorders
Introduction
Myelin oligodendrocyte glycoprotein (MOG) is located on the surface of myelin and is mainly expressed in the central nervous system.1 Oligodendrocyte glycoprotein antibody-associated disease (MOGAD) is a recently identified autoimmune disease that causes inflammatory demyelination, including optic neuritis and encephalomyelitis.2 However, associated skin findings in MOGAD have not been reported.3 Here, we report a psoriasiform eruption in the setting of MOGAD, including histological analysis with a comparative assessment to psoriasis lesions in the same patient.
Case report
A 47-year-old Japanese woman presented with acute progressive decreased attention, gait disturbance, dysuria, and skin rash. She had a history of psoriasis, currently in remission. Clinical findings at the initial visit revealed scaly erythema on the tip of the nose, corners of the mouth, external ear, and gluteal cleft (Fig 1, A-C). Blood tests revealed a lymphocyte count of 590/μL (normal 1000-4800), C3 level of 63 mg/dL (normal 75-175), and IgG level of 2466 mg/dL (normal 600-1600). Serum IgG4, anti-double-stranded DNA antibodies, and other autoimmune markers tested were negative. Urinalysis revealed transient proteinuria, but renal biopsy findings were inconsistent with lupus nephritis. Magnetic resonance imaging of the brain and spinal cord demonstrated multiple gadolinium-enhancing lesions in the cerebral white matter, brain stem, and spinal cord located in C3 (C: cerrical spine), C7, and Th3 (Th: thoracic) (Fig 1, D). Cerebrospinal fluid (CSF) examination revealed an elevated cell count with mononuclear cell predominance (38/μL). CSF protein and myelin basic protein levels were elevated at 61 mg/dL and >2000 pg/mL, respectively, but oligoclonal bands were negative. Serum and CSF MOG antibodies were increased 128- and 32-fold, respectively, leading to a diagnosis of MOGAD (serum low positive, CSF positive, and supporting brain clinical/magnetic resonance imaging features).2 Skin biopsies, taken from the scaly erythema on the external ear and gluteal region, demonstrated hyperkeratosis and thickening of the epidermis, no loss of the granular layer, and infiltration of numerous plasma cells and lymphocytes in the upper to middle layers of the dermis (Fig 1, E and F). Direct immunofluorescence analysis was negative for IgG, IgA, IgM, and C3. To distinguish the skin eruption associated with MOGAD from her prior psoriasis lesions (Fig 1, G), we performed an immunohistochemical analysis. The skin biopsy taken from psoriasis 14 years ago showed hyperkeratosis with parakeratosis, regular elongation of rete ridges, loss of granular layer, and perivascular inflammatory cell infiltration (Fig 1, H). Immunohistologically, CD4-dominant T cells intensively infiltrated the perivascular region of the upper dermis, but very few CD20-positive B cells and CD68-positive macrophages were observed (Fig 1, I-L), which were considered typical for psoriasis.4 In the skin eruption associated with MOGAD on the external ear, CD4- and CD8-positive T cells, CD20-positive B cells, and CD68-positive macrophages briskly infiltrated the upper dermis (Fig 1, M-P). Similar findings were identified in skin biopsy from the intergluteal cleft (Fig 1, Q-T).Fig 1. Clinical, radiologic, histopathological, and immunohistochemical characteristics of the patient. A to C, Scaly erythematous plaques on the tip of the nose, corners of the mouth (A), external ear (B), and gluteal cleft (C). D, Brain magnetic resonance imaging reveals multiple hyperintense lesions on fluid-attenuated inversion recovery images (indicated by the red arrows) that are displayed on gadolinium-enhancing T1-weighted images as well. E and F, A skin biopsy of the scaly erythematous lesions on the external ear (E) and the gluteal cleft (F) revealed hyperkeratosis and thickening of the epidermis, no loss of the granular layer, and infiltration of numerous plasma cells and lymphocytes in the upper to middle layers of the dermis [hematoxylin and eosin staining; bar = (E) 50 μm, (F) 100 μm; inset bar = 20 μm]. G and H, Clinical and histopathologic findings of the rash diagnosed as psoriasis 12 years prior to the first. G, The skin eruptions are scattered in a disseminated manner on the head, trunk, and extremities. H, Scaly erythematous lesions reveal epidermal thickening and perivascular lymphocyte infiltration in the upper dermis (hematoxylin and eosin staining; bar = 100 μm). I to T, Immunohistochemical analysis of the scaly erythematous lesions using a rabbit monoclonal anti-CD4 (SP35) antibody (Roche, 790-4423) at 1:200 dilution, a rabbit monoclonal anti-CD8 (SP57) antibody (Roche, 790-4460) at 1:200 dilution, a mouse monoclonal anti-CD20 (L26) antibody (Roche, 760-2531), and a mouse monoclonal anti-CD68 (PG-M1) antibody (Dako, M 0876) at 1:100 dilution (bar = 50 μm). MOGAD, Myelin oligodendrocyte glycoprotein antibody-associated disease.
After methylprednisolone pulse therapy, oral prednisolone (40 mg/d) resolved the clinical finding of encephalomyelitis and all the lesions of scaly erythema. Prednisolone tapering to 12 mg/d caused no flare in skin findings.
Discussion
Recently, several studies reported that MOG functions as an essential target for autoantibodies and cell-mediated immune responses in MOGAD.5, 6, 7, 8 Previous studies have suggested that Th1 and Th17 cells are involved in autoimmune encephalomyelitis.5^,^6 In a case report, immunohistochemical analysis of brain biopsy specimens in MOGAD has revealed that CD3-positive T cells, CD20-positive B cells, and CD68-positive macrophages infiltrate around blood vessels.7 In addition, Takai et al conducted a brain biopsy on 11 cases of MOGAD, confirming infiltrated cells consisting mainly of CD4-dominant T cells, CD20-positive B cells, and CD68-positive macrophages in the perivascular space and demyelinating lesions. They concluded that CD4-predominant T-cell infiltration and perivascular macrophages are the characteristic findings of the acute phase of MOGAD, which is different from other demyelinating diseases.8 In our case, the patient presented with scaly erythema clinically indistinguishable from psoriasis. However, the distribution of her current lesions was different from those of her prior episodes of psoriasis. The histological and immunohistochemical analysis in our patient showed hyperkeratosis and parakeratosis with perivascular infiltrations of CD4-positive T cells in both the skin eruption associated with MOGAD and psoriasis, which would support the similarity in clinical appearance. Interestingly, we confirmed the presence of significant CD20-positive B cells and CD68-positive macrophages in the dermis in the lesions associated with MOGAD, consistent with the findings noted in brain biopsies of MOGAD previously reported. Because MOG protein expression is limited to the central nervous system,1 it would be unclear which molecules in the skin would induce the immune response in our MOGAD case. To the best of our knowledge, there are no previous reports of skin findings associated with MOGAD. Therefore, it is unclear whether skin eruption occurs in MOGAD patients with or without a history of psoriasis. However, considering the immunohistochemical findings of MOGAD demyelinating lesions by brain biopsy, the CD20-positive B cell and CD68-positive macrophage infiltration into the skin, as well as CD4-positive T cells, could be the trigger for psoriasis-like scaly erythema.
In the future, additional reports of MOGAD-related cutaneous finding may help to clarify the mechanisms and characteristics of MOGAD-related skin eruption.
Conflict of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schluesener H.J.Sobel R.A.Linington C.Weiner H.L.A monoclonal antibody against a myelin oligodendrocyte glycoprotein induces relapses and demyelination in central nervous system autoimmune disease J Immunol 1391987401640213500978 · pubmed ↗
- 2Banwell B.Bennett J.L.Marignier R.Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease: international MOGAD Panel proposed criteria Lancet Neurol 22202326828210.1016/s 1474-4422(22)00431-836706773 · doi ↗ · pubmed ↗
- 3Jurynczyk M.Messina S.Woodhall M.R.Myelin oligodendrocyte glycoprotein antibody-associated disease: an immunopathological study J Brain 140201731283138
- 4Vo S.Watanabe R.Koguchi-Yoshioka H.CD 8 resident memory T cells with interleukin 17A-producing potential are accumulated in disease-naïve nonlesional sites of psoriasis possibly in correlation with disease duration Br J Dermatol 181201941041210.1111/bjd.1774830737771 · doi ↗ · pubmed ↗
- 5Stromnes I.M.Cerretti L.M.Liggitt D.Harris R.A.Goverman J.M.Differential regulation of central nervous system autoimmunity by T(H)1 and T(H)17 cells Nat Med 14200833734210.1038/nm 171518278054 PMC 2813727 · doi ↗ · pubmed ↗
- 6Domingues H.S.Mues M.Lassmann H.Wekerle H.Krishnamoorthy G.Functional and pathogenic differences of Th 1 and Th 17 cells in experimental autoimmune encephalomyelitis P Lo S One 52010 e 1553110.1371/journal.pone.0015531 PMC 300042821209700 · doi ↗ · pubmed ↗
- 7Ikeda T.Yamada K.Ogawa R.The pathological features of MOG antibody-positive cerebral cortical encephalitis as a new spectrum associated with MOG antibodies: a case report J Neurol Sci 392201811311510.1016/j.jns.2018.06.02830048831 · doi ↗ · pubmed ↗
- 8Takai Y.Misu T.Kaneko K.Myelin oligodendrocyte glycoprotein antibody-associated disease: an immunopathological study Brain 14320201431144610.1093/brain/awaa 10232412053 · doi ↗ · pubmed ↗